Download presentation
Presentation is loading. Please wait.

1
Monocyte/Macrophage Disorders
Northeast Regional Medical Center/KCOM

2
Granuloma Annulare Localized Generalized Macular Deep Perforating
In HIV In Lymphoma

3
Granuloma Annulare Common, Idiopathic, all races
50% patients IgM and C3 in vessels LCV changes sometimes seen Suggests Ab mediated vasculitis Common in HIV patients EBV sometimes found Occurs in resolved lesions Zoster

4
GA - Histology Classic – histiocytes palisading around “necrobiotic” collagen. Granulomas located in the upper dermis with perivascular lymphocytic infiltrate Necrobiosis – “altered” collagen, paler grayer hue, fragmented, haphazardly arranged, more compact. Mucin prominent in older lesions.

5
GA- Histology Interstitial – diffuse dermal infiltrate between collagen bundles consisting of histiocytes, monocytes, neutrophils. “Skip” areas of normal dermis seen. Interstitial mucin often seen. May be adjacent to classic granulomas

6
Interstitial GA NLD Upper dermis “Skip areas” Mucin Deep dermis, subQ
No “skip” areas No mucin

13
Localized GA Young adults Acral Annular, scalloped
White or pink flat topped papules spread peripherally 75% clear in 2 yrs 25% last 8 yrs

19
Diffuse GA MC women past middle age Diabetes reported in 20% cases
MC neck, upper trunk, shoulders MC form of GA seen in HIV. Clears spontaneously in 3-4 years. Difficult to treat.

23
Subcutaneous GA Aka Deep, Pseudorheumatoid Nodule
MC children, boys > girls 2:1 MC ages 5-12. Acral distribution History of trauma preceding lesion Asymptomatic but often an extensive workup is done to rule out JRA.

25
Perforating GA MC dorsum of hands Papules with central keratotic core
Core represents transdermal elimination of degenerated or “necrobiotic” material in center of palisaded histiocytes.

27
GA in HIV disease GA may occur at all phases of HIV disease.
Typically papular lesions 60% Diffuse, 40% Localized Photodistributed and perforating lesions may occur

28
GA and Lymphoma Rare Atypical presentation: Facial or Palmar Painful
Any type of lymphoma can occur. Lymphoma may occur before or after the GA.

29
GA- Treatment Biopsy, IL, Cryo, topical Vit. E, Excision
GENERALIZED: Problematic Oral steroids, high dose but high relapse rate – diabetes complicates Dapsone, Nicotinomide, SSKI, Cyclosporine, Accutane.

30
Annular Elastolytic Giant Cell Granuloma of Meischer/Actinic Granuloma of O’Brien

31
AGOB – Photo- distribution, papules and plaques
Annular Elastolytic Giant Cell Granuloma of Meischer/Actinic Granuloma of O’Brien Variants of GA. AEGCG – solitary atrophic thin yellow plaque on the forehead, NLD-like. AGOB – Photo- distribution, papules and plaques

32
Histo: Like GA, but with Giant Cells, Elastophagocytosis

33
Histo: Like GA, but with Giant Cells, Elastophagocytosis

34
Histo: Like GA, but with Giant Cells, Elastophago-cytosis

35
Photoexacerbated GA

36
Granuloma Mulitforme of Leiker
Similar histology to AEGCG & AGOB Only Central Africa, Adults > 40 yrs old. Upper Trunk and Arms Begin as small papules, expand into round or oval plaques 15cm wide and as much as 4mm in height. Must rule out tuberculoid leprosy.

37
Granuloma Mulitforme of Leiker

38
Sarcoidosis Multisystem Disease Lungs, lymph nodes, skin and eyes MC.
10x more frequent in blacks in US Women under age 40 Irish, African, Afro-Caribbean. Presence inversely proportional to the incidence of TB and/or Leprosy.

39
Sarcoidosis Etiology unknown HLA-A1 – Lofgren’s syndrome
HLA-B13 – Chronic & Persistent form HLA-B8 HLA-DR3 Final common pathway is granuloma formation

40
NON-CASEATING GRANULOMAS COMPOSED OF EPITHELIOID CELLS AND OCCASIONAL LANGERHAN’S GIANT CELLS

41
“NAKED” GRANULOMAS “NAKED” meanse a sparse rather than a dense infiltrate. Lymphocytes, macrophages & fibroblasts may occur

43
Asteroid Body inside a multinucleated giant cell

44
SCHAUMANN OR CONCHOIDAL BODIES ARE COMPOSED OF CALCIUM CARBONATE
SCHAUMANN OR CONCHOIDAL BODIES ARE COMPOSED OF CALCIUM CARBONATE. THEY ARE EASILY MISSED (LEFT) IF NOT VIEWED UNDER POLARIZED LIGHT (RIGHT)
 IF NOT VIEWED UNDER POLARIZED LIGHT (RIGHT)")
45
Sarcoidosis AKA…. Besnier-Boeck-Schaumann Disease Boeck’s sarcoid
Besnier’s lupus pernio Schaumann’s benign lymphogranulomatosis

46
Sarcoid Skin Involvement
Anywhere from 9% to 37% of cases. 2 types: specific and non-specific Specific: granulomas on biopsy Non-Specific: reactive, Erythema Nodosum Skin findings may occur before, during or after systemic findings.

47
Sarcoid – like syphillis, mimics many other dz’s
Papules, nodules, plaques. Subcutaneous nodules. Scar sarcoid, erythroderma. Ulcerations, verrucous. Ichthyosiform, hypomelanotic

48
Papular Sarcoid MC form AKA Miliary Sarcoid
Face, eyelids, neck, shoulders May involute to macules Ddx: syringomas

49
Papular Sarcoid

50
Papular Sarcoid

51
Papular Sarcoid

52
Papular Sarcoid

53
Annular Sarcoidosis Central clearing Hypo-pigment-ation Atrophy
Scarring Favor head & neck Assoc. with chronic sarcoidosis

54
Annular Sarcoidosis

55
Hypopigmented Sarcoid
May be the earliest sign of sarcoidosis in blacks. MC extremities Visually macular, but often have a palpable dermal or subQ component in center of lesion

56
Hypopigmented Sarcoid

57
Lupus Pernio Violaceous Nose, cheeks, lips Forehead, ears
43% associated with punched out bone lesions. 37% Ocular lesions Nasal perforation

58
Punched-Out Lytic lesions, Bone Cysts

59
Ulcerative Sarcoidosis

60
Lupus Pernio

61
Lupus Pernio

62
Lupus Pernio

63
Lupus Pernio

64
Darier-Roussy Sarcoid
5% or fewer of patients with sarcoidosis have subcutaneous nodules.

65
Darier-Roussy (SubQ)
")
66
Scar Sarcoid

67
Scar Sarcoid

68
Erythrodermic Sarcoid
Extremely Rare Begins as erythematous patches that become confluent.

69
Ichthyosiform Sarcoid
Legs Arms No palpable component

70
Ichthyosiform Sarcoid

71
Alopecia Occurs in 2 settings; 1) Existing plaques extend onto scalp.
--leads to permanent scarring. 2) Macular lesions appear on scalp resembling Alopecia Areata --may be permanent or reversible
 Macular lesions appear on scalp resembling Alopecia Areata. --may be permanent or reversible.")
72
Morpheaform Sarcoid Rare Dermal Fibrosis Simulates Morphea
Antimalarials may help.

73
Morpheaform Sarcoid

74
Morpheaform Sarcoid

75
Mucosal Sarcoid Pinhead sized papules
Grouped or fused together to form a plaque.

76
Erythema Nodosum in Sarcoid
MC nonspecific cutaneous finding in sarcoidosis Young females Anterior shins Good prognosis Lofgren’s Syndrome = fever, arthralgias, hilar adenopathy, fatigue, EN

77
Systemic Sarcoidosis MC – Lungs Ocular 20-30%
Bones & Liver 20%, elevated Alk Phos. Renal, Hypercalcemia Heart, CNS, Spleen Elevated ACE levels to follow disease activity only.

78
Heerfort’s Syndrome Parotid gland enlargement
Lacrimal gland enlargement Uveitis Fever Sarcoidosis

79
Mikulicz’s Syndrome Sarcoidosis with enlargement of the;
Lacrimal glands Submaxillary and Parotid glands. Problematic: numerous conditions involving enlarged partoid glands have since been named after Dr. Mikulicz.

80
CXR- Hilar Adenopathy

81
Sarcoidosis in Fingers

82
Sarcoidosis in Fingers

83
CNS

84
Candle-wax drippings – granulomatous uveitis

85
Sarcoid - Treatment Systemic Corticosteroids Antimalarials
Methotrexate Thalidomide

86
Non-X Histocytoses Juvenile Xanthogranuloma
Benign Cephalic Histiocytosis Solitary/Multicentric Reticulohistiocytosis Generalized Eruptive Histiocytoma Necrobiotic Xanthogranuloma Xanthoma Disseminatum Papular Xanthoma Indeterminate Cell Histiocytosis Progressive Nodular Histiocytoma Hereditary Progressive Mucinous Histiocytosis Rosai-Dorfman Disease Sea-Blue Histiocytosis

87
Juvenile Xanthogranuloma (JXG)
MC Non-Langerhans’ histiocytosis 1st year of life, usu. white males 80% are solitary, well demarcated, firm, rubbery red to pink with yellow tinge Regress in 3-6 years with atrophy. Ocular involvement rare, MC iris Assoc. with NF-1 and JCML

89
JXG Histopathology Non-encapsulated
Infiltrate in the upper and mid reticular dermis Mononuclear cells with abundant amphophilic cytoplasm that is poorly lipidized or vacuolated.

90
MULTINUCLEATED “FOAM” CELLS aka TOUTON GIANT CELLS ALONG WITH EOS, NEUTS, LYMPHS.
STAINS: + CD1 + FACTOR XIIIa - S100

91
Benign Cephalic Histiocytosis
Rare Males 2:1, Onset 6-12 months of age Begins on head, cheeks, spreads to neck and upper trunk Multiple reddish yellow papules 2-3mm, may coalesce into a reticulate pattern. Involute over 2 to 8 years with atrophy

92
BENIGN CEPHALIC HISTIOCYTOSIS
DIFFUSE DERMAL INFILTRATION OF NON-LIPIDIZED HISTIOCYTIC CELLS, S-100 NEGATIVE

93
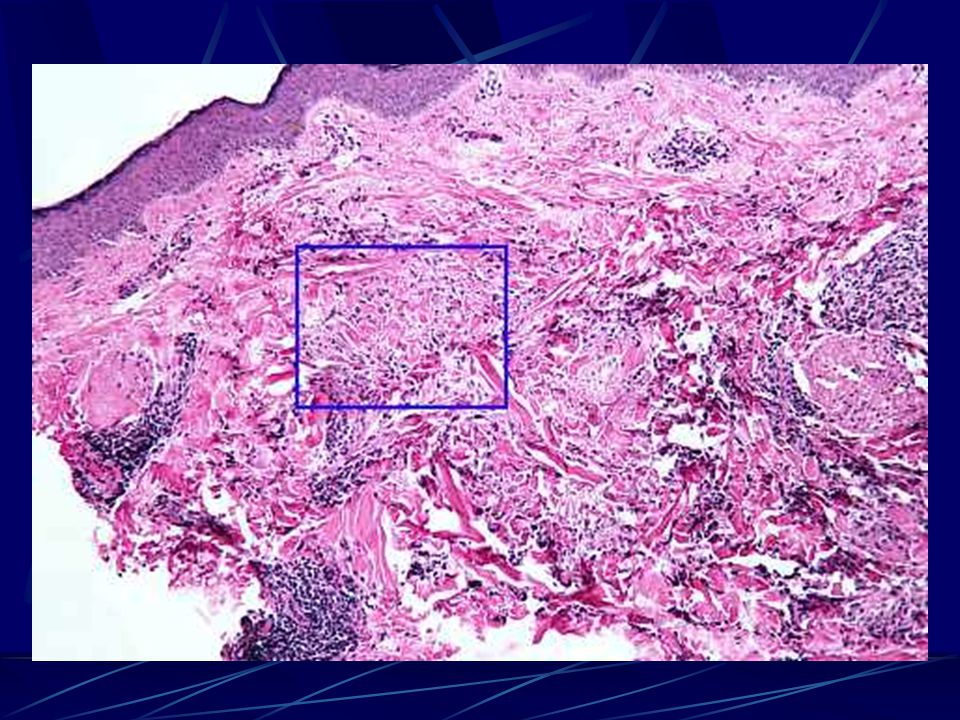
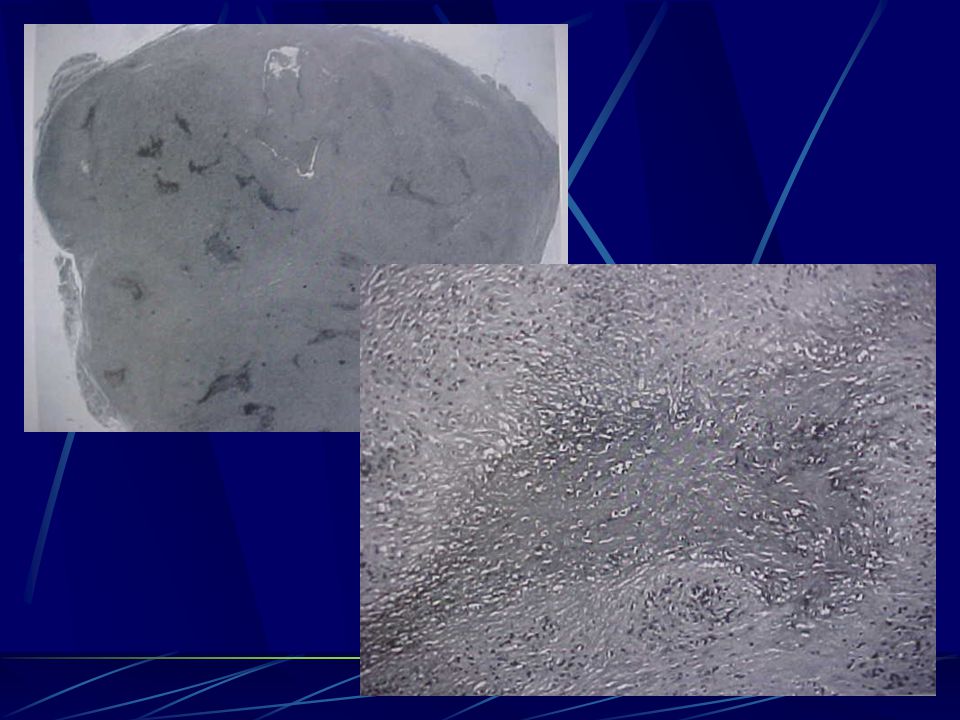
Reticulohistiocytosis
Solitary form – aka Reticulohistiocytic Granuloma or Reticulohistiocytoma Solitary form has no systemic involvement Multicentric form – aka Multicentric Reticulohistiocytosis Underlying malignancy in 30%

94
Reticulohistiocytic Granuloma

95
Reticulohistiocytic Granuloma: Multinucleate Giant Cells, Histiocytes, Lymphocytes with some stroma fibrosis

96
Multicentric Reticulohistiocytosis
Multisystem disease, 5th decade, F>M. 90% Face & hands, red-brown papules and nodules Paronychia: “coral bead” appearance Joints symmetrically involved with mutilating arthritis, telescoping shortening of digits, doigts en lorgnette, opera-glass fingers, RF is negative 1/3 have high cholesterol, xanthelasma

97
“Coral Bead” Paronychia

98
Classic Ground Glass Touton Giant Cells, PAS +

99
90% Face & Hands

100
Tx: Multicentric Reticulohisticytosis
Treatment is problematic because mutilating arthritis requires immunosuppressive therapy. Immunosuppressive therapy can worsen underlying malignancies Prednisone, Antimalarials, MTX, Cytoxan, PUVA, Nitrogen mustard.

101
Generalized Eruptive Histiocytoma
Widespread symmetric papules, trunk and proximal extremities, come in crops Progressive development of new lesions over several years with eventual spontaneous involution to hyper-pigmented macules Flesh, brown or violaceous papules Controversy: is this just xanthoma disseminatum? MRH? Indeterminate cell histiocytosis?

102
Generalized Eruptive Histiocytoma

103
GENERALIZED ERUPTIVE HISTIOCYTOMA:
DERMAL INFILTRATE OF NON-LIPIDIZED MONONUCLEAR HISTIOCYTES, S-100 IS NEGATIVE

104
GENERALIZED ERUPTIVE HISTIOCYTOMA:
DERMAL INFILTRATE OF NON-LIPIDIZED MONONUCLEAR HISTIOCYTES, S-100 IS NEGATIVE

105
Necrobiotic Xanthogranuloma (NXG)
Multisystem disease of older adults Characteristic periorbital yellow plaques that resemble xanthelasmas except that they are deep, firm, indurated and may extend into the orbit Trunk & proximal extremity lesions are orange-red plaques with an active red border and an atrophic border with superficial telangiectiasias.

106
NXG: Periorbital yellow plaques that resemble xanthelasmas except that they are deep, firm, indurated, may involve the orbit

107
NXG: Trunk & proximal extremity lesions are orange-red plaques w/ active red border & an atrophic border with superficial telangiectasias

108
NXG: conjunctivitis, keratitis, scleritis, uveitis, iritis, ectropion or proptosis

109
NXG: Process extends into the fat, obliterating fat lobules
NXG: Process extends into the fat, obliterating fat lobules. Extensive zones of degenerated collagen or “necrobiosis” surrounded by palisaded macrophages.

110
NXG: Foam Cells with abundant infiltrate of lymphocytes, plasma cells

111
NXG: Cholesterol Clefts

112
NXG and Malignancy 80% IgG monoclonal paraproteinemia (Kappa)
Bone marrow may show plasmacytosis, anemia, leukopenia, myeloma, myelodysplastic syndromes. Cause unknown, course progressive Treat aimed at paraproteinemia: Melaphan, Chlorambucil, Corticosteroids, Plasmapheresis, Alpha Interferon-2b

113
Xanthoma Disseminatum
Serum lipids are normal, MC young males Mucocutaneous, discreet, disseminated Intertriginous distribution Diabetes Insipidus 40% due to xanthomatous infiltration of the pituitary gland. Chronic and Benign, may persist, may involute spontaneously after some years

114
XD - Periorbital

115
XD - Axillary

116
XD - Pathology Xanthoma Cells Eosinophilic Histiocytes
Numerous Touton giant cells Inflammatory cell infiltrate usually present.

117
Papular Xanthoma Small yellowish papules Localized or generalized
No tendency to merge into plaques Aggregates of foam cells in the dermis without a cellular or histiocytic phase Absence of inflammatory cells.

118
Indeterminate Cell Histiocytosis
Dermal precursors of Langerhan’s cells S-100 positive CD1 positive NO BIRBECK GRANULES! Chronic without spontaneous involution No systemic involvement

119
Progressive Nodular Histiocytosis
Superficial papules & deeper nodules Diffuse, symmetrical, non-flexural. Larger lesions may ulcerate, become painful Face lesions may coalesce into leonine facies General health is good

120
Progressive Nodular Histiocytosis
Histo: DF-like, few Toutons, lacks the PAS+ ground glass giant cells of MRH. Stains positive for Vimentin, CD68, Factor XIIIa Stains negative for S-100 and CD34

121
Hereditary Progressive Mucinous Histiocytosis in Women
AD or X-linked Few to numerous flesh to red-brown papules up to 5mm in diameter Face, arms, forearms, hands, legs Onset 2nd decade Slow progression, no tendency to spontaneous involution, no systemic involvement

122
Hereditary Progressive Mucinous Histiocytosis in Women
May histologically differentiate from other non-X histiocytoses as follows: Familial pattern Abundant mucin + Alcian blue staining Lack of lipidized and multinucleated cells

123
Rosai-Dorfman Disease
Aka Sinus Histiocytosis with Massive Lymphadenopathy Onset 1st or 2nd decade of life Fever, massive cervical LAD, polyclonal hyperglobulinemia, leukocytosis, anemia, elevated SED rate. Males and blacks MC. Skin involvement in 43% of cases Most patients with skin lesions are > age 40

124
Rosai-Dorfman Disease
Isolated or disseminated yellow-brown papules or nodules, or macular erythema. Large annular lesions resembling GA may occur. HHV-6 identified in numerous reports. May clear spontaneously Skin biopsy non-specific unless emperipolesis is present but lymph node pathology is characteristic…..

125
Rosai-Dorfman Disease – LN Biopsy
Expansion of the sinuses by large foamy histiocytes admixed with plasma cells CD4, Factor XIIIa and S-100 positive No Birbeck granules

126
RDD - Emperipolesis – Histiocytes engulf plasma cells and lymphocytes

127
RDD - Emperipolesis

128
RDD - Treatment Radiation Chemotherapy Systemic corticosteroids
Thalidomide

129
Sea-Blue Histiocytosis
Familial or Acquired Characteristic and diagnostic cell is a histiocyte containing cytoplasmic granules that stain as follows: Blue-green with Geimsa Blue with May-Gruenwald

130
Sea-Blue Histiocytosis
Lesions include papules, eyelid swelling and patchy gray pigmentation of the face and upper trunk. Infiltrates marrow, spleen, liver, lymph nodes, lungs and skin in some cases. Similar findings seen in patients with Myelogenous leukemia and Neimann-Pick Disease, and following prolonged use of IV fat supplementation

131
Sea-Blue Histiocytosis – Bone Marrow

132
X-type Histiocytoses Hashimoto-Pritzker Histiocytosis X
aka Congenital Self-Healing Reticulohistiocytois Histiocytosis X Aka Letterer-Siwe Aka Hand-Schuller Christian Aka Eosinophilic Granuloma

133
Hashimoto-Pritzker Onset: birth or very soon thereafter
Solitary or multinodular Red, brown, pink or dusky Lesions > 1 cm characteristically ulcerate as they resolve Asymptomatic, resolves in 8 to 24 weeks

134
Hashimoto-Pritzker

135
Hashimoto-Pritzker Before and After

136
Hashimoto-Pritzker

137
Hashimoto-Pritzker

138
EM: 10-25% of cells have Langerhans’ cell granules, but this does not distinguish Hashimoto-Pritzker from Histiocytosis X.

139
H&E: large mononuclear cells & multinucleated giant cells with ground glass or foamy cytoplasm

140
HASHIMOTO-PRITZKER S-100 stain CD1a stain

141
H-P MANAGEMENT Must rule out Histiocytosis-X as both present similarly
Rule out systemic involvement with physical exam, CBC, LFT, Bone survey. If any of the above are abnormal, consider liver-spleen scan and bone marrow biopsy.

142
Histiocytosis X Proliferation of Langerhans’ cells
MC-Bone, Skin, Lymph, Lungs, Liver and Spleen, Endocrine glands, CNS. Children age 1-4 years old Lymphs are clonal, but not as atypical appearing as lymphoma cells – debate as to whether this is neoplastic v. reactive

143
Histiocytosis X RESTRICTED TYPES:
A) Biopsy proven skin rash without other involvement B) Monostotic lesions, with or without diabetes insipidus, LAD or rash C) Polyostotic lesions with or without diabetes insipidus, LAD or rash.
 Biopsy proven skin rash without other involvement. B) Monostotic lesions, with or without diabetes insipidus, LAD or rash. C) Polyostotic lesions with or without diabetes insipidus, LAD or rash.")
144
Histiocytosis X EXTENSIVE TYPE:
A) Visceral involvement with or without bone lesions, diabetes insipidus, LAD or rash but WITHOUTsigns of organ dysfunction of lung, liver or hematopoetic system B) Visceral involvement with or without bone lesions, diabetes insipidus, LAD or rash but WITH signs of organ dysfunction.
 Visceral involvement with or without bone lesions, diabetes insipidus, LAD or rash but WITHOUTsigns of organ dysfunction of lung, liver or hematopoetic system. B) Visceral involvement with or without bone lesions, diabetes insipidus, LAD or rash but WITH signs of organ dysfunction.")
145
Histiocytosis X Distribution
MC is Letterer-Siwe: Tiny red, red-brown or yellow papules that are widespread but favor the intertriginous areas, behind ears and scalp. Lesions may erode or weep. In children, LS distribution is assoc. with multisystem disease, but in adults 25% have disease limited to skin only.

146
Histicytosis X - scalp

147
Often mistaken for SD, but focal hemorrhage is present

148
Often mistaken for SD, but focal hemorrhage is present

152
Histiocytosis X - TX Skin only: topical steroids, nitrogen mustard, PUVA, Interferon Alpha. extensive disease but without organ dysfunction: oral corticosteroids Extensive disease with orgain dysfunction: Vinblastine, Cyclosporine, Radiation. Refractory: 2-chlorodeoxyadenosine

153
SLICK RICK SAYS: “DON’T FORGET TO TURN IN YOUR TEST QUESTIONS”
THE END SLICK RICK SAYS: “DON’T FORGET TO TURN IN YOUR TEST QUESTIONS”

Similar presentations