Download presentation
Presentation is loading. Please wait.

1
Overweight Children Prevalence, Problems, and Solutions (?) David L. Gee, PhD FCSN 547 – Nutrition Update Summer 2004

4
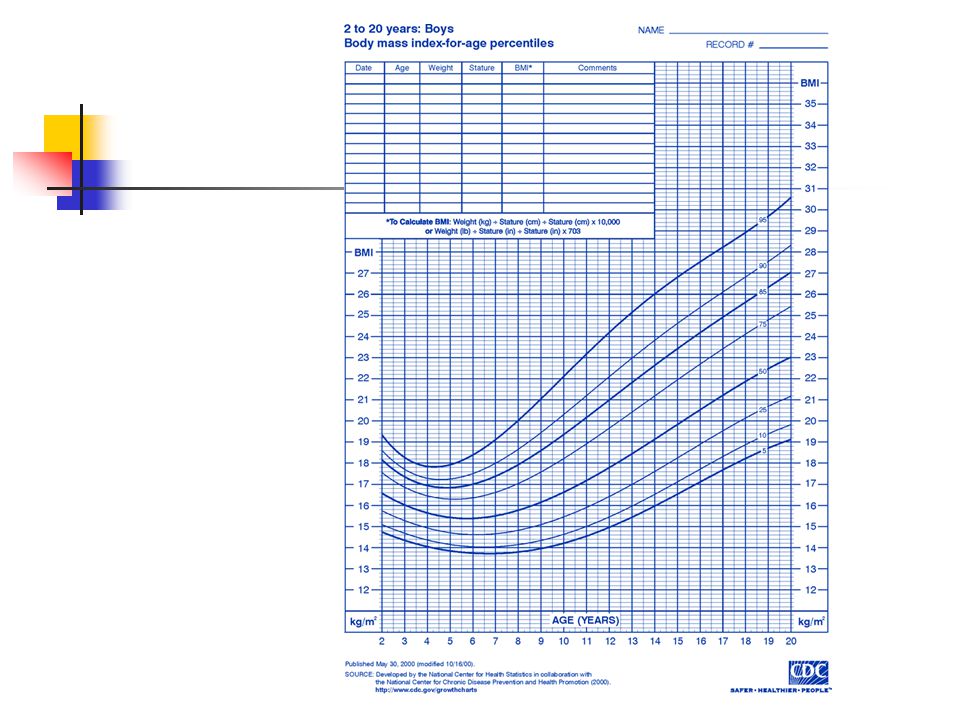
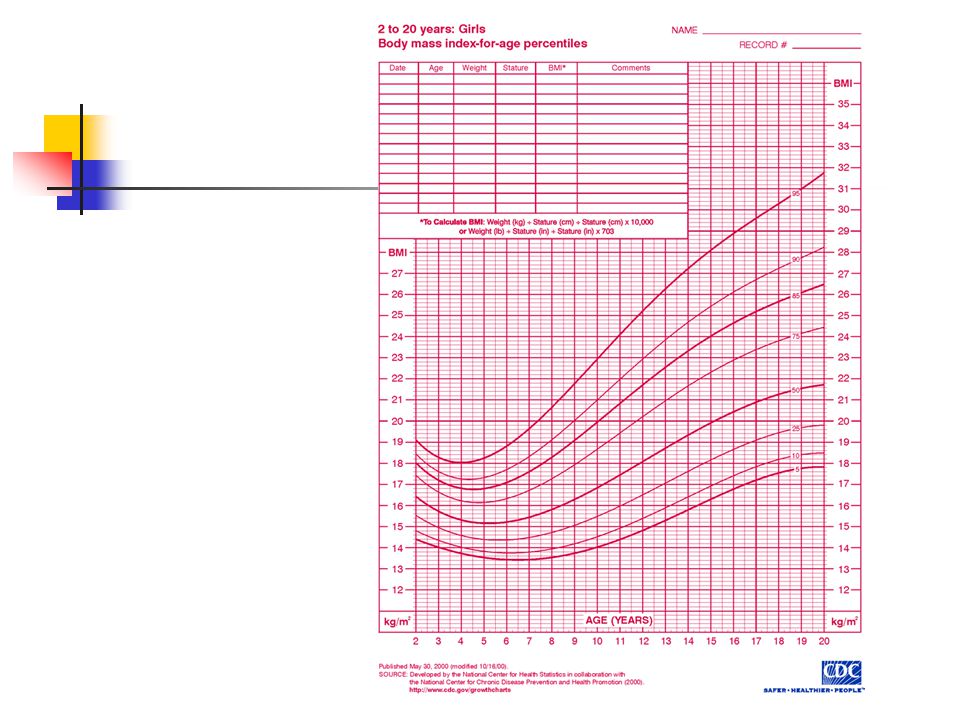
Assessment of Overweight in Children 1997 Expert Panel The Maternal and Child Health Bureau, Health Resources and Services Administration, the Department of Health and Human Services PEDIATRICS Vol. 102 No. 3 September 1998, p. e29 Recommends that BMI be routinely used to screen children for overweight Defined Overweight as a BMI for age over the 95 th percentile Risk for overweight as a BMI for age between the 85 th and 95 th percentile

7
Is a child’s BMI useful in predicting adult obesity?

9
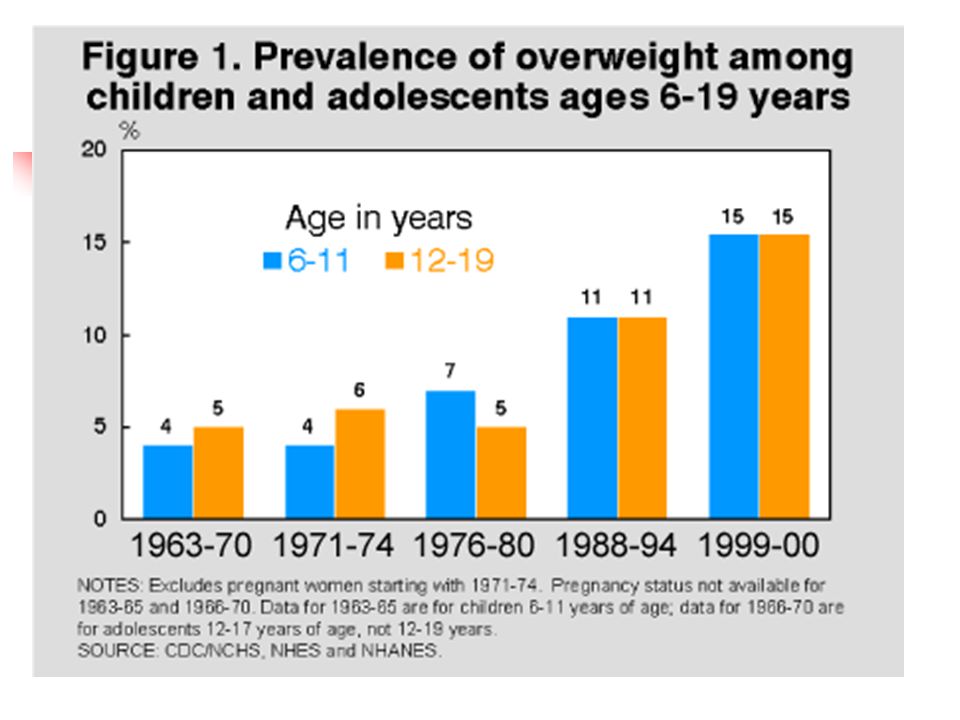
Prevalence of Overweight Children in the US

10
Prevalence of Overweight and Obesity Among US Children, Adolescents, and Adults, 1999-2002 A. Hedley et al. JAMA 2004; 291: 2847-2850 (June 16)
.")
11
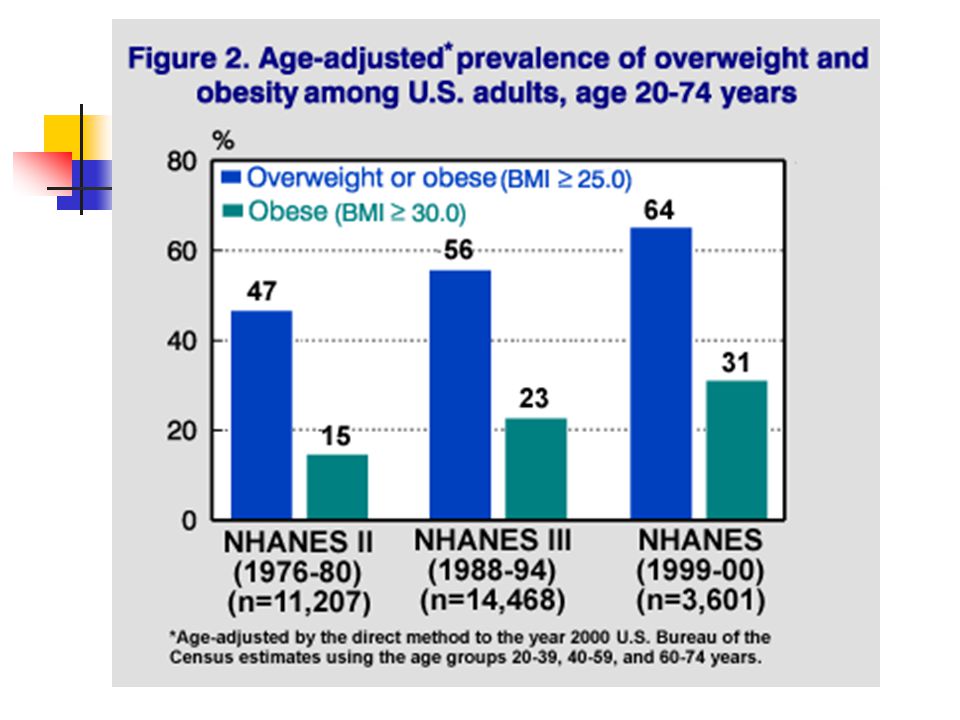
Prevalence of Overweight and Obesity Among US Children, Adolescents, and Adults, 1999-2002 NHANES 1999-2000 N=4115 adults N=4018 children 2001-2002 N=4390 adults N=4258 children Adult prevalence 65.1% overweight or obese 30.4% obese 5.1% extreme obese (BMI>40)
")
12
Prevalence of Overweight and Obesity Among US Children, Adolescents, and Adults, 1999-2002 Children 6-19 yrs 31% at risk for overweight or overweight 16% overweight At risk for overweight or overweight by age 2-5 = 22.6% 6-11 = 31.2% 12-19 = 30.9%

13
Prevalence of Overweight and Obesity Among US Children, Adolescents, and Adults, 1999-2002 At risk for overweight or overweight by gender Boys = 31.8% Girls = 30.3% At risk for overweight or overweight By ethnicity White = 28.2% (29.2%b, 27%g) Black = 35.4% (31%b, 40%g) Mexican-American = 39.9% (42.8%b, 36.6%g)
 Black = 35.4% (31%b, 40%g) Mexican-American = 39.9% (42.8%b, 36.6%g)")
14
Type 2 Diabetes in the Young The evolving epidemic (review article) Z. Bloomgarden Diabetes Care 2004 (Apr); 27:998-1010
; 27:")
15
Type 2 Diabetes in the Young The evolving epidemic Prevalence NHANES III (1988-1994) ~3000 subjects, 12-19 yo IFG: 17.6 per 1000 HbA1c>6%: 3.9 per 1000 Diabetes (all types): 4.1 per 1000 Extrapolate: ~600,000 US adolescents with some degree of glycemic abnormality How many with Type 2 diabetes?
 ~3000 subjects, yo IFG: 17.6 per 1000 HbA1c>6%: 3.9 per 1000 Diabetes (all types): 4.1 per 1000 Extrapolate: ~600,000 US adolescents with some degree of glycemic abnormality How many with Type 2 diabetes")
16
Type 2 Diabetes in the Young The evolving epidemic Prevalence Sinha et al., NEJM 346:802-810, 2002 167 obese adolescents and children 4% prevalence of Type 2 DM All in Hispanic and black adolescents IGT 16% obese white 27% obese black 26% obese Hispanic (UK study found risk of Type 2 DM 13.5 times greater in Asian than white children)
")
17
Prevalence of T2 diabetes has increased significantly (2-3X) among Indian children in the past 30 years.
 among Indian children in the past 30 years.")
18
Type 2 Diabetes in the Young The evolving epidemic Prevalence Trends 10 fold increase from 1982-1994 in Cincinnati J. Ped. 128:608-615, 1996 % of diabetic children w/ T2 increased from 9.4% (1994) to 20% (1998) (Florida) Pub. Health Rep. 117:373-379, 2002 ~1/3rd of children w/ diabetes have T2 in OH, AR, CA(Hispanics) Diabetes Care 22:345-354, 1999
 to 20% (1998) (Florida) Pub. Health Rep. 117: , 2002 ~1/3rd of children w/ diabetes have T2 in OH, AR, CA(Hispanics) Diabetes Care 22: ,")
19
Type 2 Diabetes in the Young The evolving epidemic Prevalence Other factors: Gender Girls 1.7 times more likely than boys Diabetes Care 22:345-354, 1999 Family History 2/3 rd of children w/ T2DM with at least one parent with T2DM Diabetes Care 23:381-389, 2000

20
Type 2 Diabetes in the Young The evolving epidemic Prevalence Other factors (1998 study from India) Low birthweight High prepubertal weight
 Low birthweight High prepubertal weight")
21
Type 2 Diabetes in the Young The evolving epidemic Screening Prevalence of T2DM in young low but growing Prevalence of overweight growing rapidly Screening of all children not cost effective ~$10,000 per case found (Japan/Taiwan study) ADA/AAP Consensus Position Diabetes Care 2000 Testing >10yr if BMI > 85 th pct with 1 o or 2 o relative with DM, at risk ethnic group, or signs of insulin resistance (metabolic syndrome)
 ADA/AAP Consensus Position Diabetes Care 2000 Testing >10yr if BMI > 85 th pct with 1 o or 2 o relative with DM, at risk ethnic group, or signs of insulin resistance (metabolic syndrome)")
22
Obesity and the Metabolic Syndrome in Children and Adolescents R. Weiss et al. NEJM 350:2362-74,2004

23
Obesity and the Metabolic Syndrome in Children and Adolescents Metabolic Syndrome Cluster of metabolic abnormalities associated with insulin resistance Diagnosis of Metabolic Syndrome in Adults Three or more of the following: Abdominal Obesity men > 40” waist circumference women > 35” waist circumference Hypertriglyceridemia (>150 mg/dl) Low HDL men < 40 mg/dl women < 50 mg/dl Pre-hypertension (>130/>85 mmHg) Pre-diabetes (> 110 mg/dl)
 Low HDL men < 40 mg/dl women < 50 mg/dl Pre-hypertension (>130/>85 mmHg) Pre-diabetes (> 110 mg/dl)")
24
Obesity and the Metabolic Syndrome in Children and Adolescents Methods 439 obese children/adolescents 31 overweight siblings 20 non-obese siblings 41% white, 31% black, 27% Hispanic Administered oral GTT Measured BP, plasma lipids, C-reactive protein

25
Obesity and the Metabolic Syndrome in Children and Adolescents Criteria for Metabolic Syndrome in Children Obesity (instead of waist circumference) Obese = z-score >2.0 for BMI Moderate Obese = z-score 2.0-2.5 Severe Obese = z-score > 2.5 Metabolic values TG: > 95 th pct HDL-C: < 5 th pct Glucose intolerance following OGTT Insulin resistance = [fasting glu]x[fasting plasma insulin]/22.5
![Obesity and the Metabolic Syndrome in Children and Adolescents Criteria for Metabolic Syndrome in Children Obesity (instead of waist circumference) Obese = z-score >2.0 for BMI Moderate Obese = z-score Severe Obese = z-score > 2.5 Metabolic values TG: > 95 th pct HDL-C: < 5 th pct Glucose intolerance following OGTT Insulin resistance = [fasting glu]x[fasting plasma insulin]/22.5](http://images.slideplayer.com/16/5005760/slides/slide_25.jpg "Obesity and the Metabolic Syndrome in Children and Adolescents Criteria for Metabolic Syndrome in Children Obesity (instead of waist circumference) Obese = z-score >2.0 for BMI Moderate Obese = z-score Severe Obese = z-score > 2.5 Metabolic values TG: > 95 th pct HDL-C: < 5 th pct Glucose intolerance following OGTT Insulin resistance = [fasting glu]x[fasting plasma insulin]/22.5")
26
Obesity and the Metabolic Syndrome in Children and Adolescents Anthropometric & Metabolic Characteristics Non-obeseOverweightModerate Obese Severe Obese BMI 18.424.533.440.6 Glucose (mg/dl,<0.05) 87.486.890.590.2 Insulin uU/ml,<.001 10.314.631.338.6 Insulin resistance <.001 2.23.127.058.69 Triglycerides Mg/dl, <.001 48.483.1104.696.5
 Insulin uU/ml,< Insulin resistance < Triglycerides Mg/dl, <")
27
Obesity and the Metabolic Syndrome in Children and Adolescents Anthropometric & Metabolic Characteristics Non-obeseOverweightModerate Obese Severe Obese HDL-C Mg/dl,<.001 58.546.741.139.9 LDL-C Mg/dl, p=.41 92.295.598.197.3 Systolic BP mmHg,<.001 106116121124 IGT %,.01 03.2314.419.9 CRP Mg/dl,.001.01.05.13.33

28
Obesity and the Metabolic Syndrome in Children and Adolescents Prevalence Overall 38.7% in moderately obese 49.7% in severely obese 39% in severely obese blacks “…metabolic syndrome is far more common among children and adolescents than previously reported…prevalence increases directly with the degree of obesity.”

29
Prevalence of metabolic syndrome increases with degree of insulin resistance

30
Health-Related Quality of Life of Severely Obese Children and Adolescents J. Schwimmer et al JAMA 289:1813-1819 (Apr 9, 2003)
.")
31
Health-Related Quality of Life of Severely Obese Children and Adolescents Health-related QOL Physical functioning Emotional functioning Social functioning School functioning 106 children & adolescents mean age = 12 yrs (+3) Mean BMI = 34.9 (+9.3) (z-score=2.6) Compared with 401 healthy and 106 cancer pediatric patients
 Mean BMI = 34.9 (+9.3) (z-score=2.6) Compared with 401 healthy and 106 cancer pediatric patients")
32
Obese children and adolescents reported significantly lower health-related QOL in all domains compared with healthy controls.

33
Obese children were more likely to have impaired health-related QOL than healthy controls and were similar to children and adolescents with cancer.

34
Health-Related Quality of Life of Severely Obese Children and Adolescents Conclusions: Obese children and adolescents reported impairment of total and all domains of QOL Likelihood of impaired QOL was 5.5 times greater in obese than healthy Obese children and adolescents reported similar impairment of QOL as in cancer patients undergoing chemotherapy Lower than children with rheumatoid arthritis, type 1 diabetes, congenital heart disease.

35
Children’s Food Consumption Patterns Have Changed over Two Decades (1973- 1994): The Bogalusa Heart Study T. Nicklas et al., JADA 104:1127-1140 (2004)
.")
36
Children’s Food Consumption Patterns Have Changed over Two Decades (1973- 1994): The Bogalusa Heart Study One 24-hr dietary recall Seven surveys of 10 yr-olds 1584 children surveyed
: The Bogalusa Heart Study One 24-hr dietary recall Seven surveys of 10 yr-olds 1584 children surveyed")
37
Amount of food consumed at schools and restaurants Increased, while the amount consumed in ‘other’ decreased.

38
The amount of dessert and candy consumed decreased, While the amount of salty snacks increased.

39
Egg and pork consumption decreased, while consumption of cheese, beef and poultry increased.

40
Consumption of fats/oils and breads/cereals decreased, while consumption of fruits/juices and mixed meats increased.

41
Milk consumption decreased while consumption of sweetened beverages increased.

42
Total consumption and consumption at lunch and dinner Increased, while consumption of snacks decreased.

43
Children’s Food Consumption Patterns Have Changed over Two Decades (1973- 1994): The Bogalusa Heart Study Findings that may contribute to childhood obesity More food consumed at restaurants More fruits and fruit juices More cheese, mixed meat, beef, and poultry More salty snacks More sweetened beverages and less milk More food consumed at lunch and dinner More total food consumed
: The Bogalusa Heart Study Findings that may contribute to childhood obesity More food consumed at restaurants More fruits and fruit juices More cheese, mixed meat, beef, and poultry More salty snacks More sweetened beverages and less milk More food consumed at lunch and dinner More total food consumed")
44
Children’s Food Consumption Patterns Have Changed over Two Decades (1973- 1994): The Bogalusa Heart Study Surprising findings Less food consumed at places other than home, school, restaurants Less fats and oils Less dessert and candy Less food consumed outside of meals (snacks)
: The Bogalusa Heart Study Surprising findings Less food consumed at places other than home, school, restaurants Less fats and oils Less dessert and candy Less food consumed outside of meals (snacks)")
45
Parent Weight Change as a Predictor of Child Weight Change in Family- Based Behavioral Obesity Treatment B. Wrotniak et al. Arch. Pediatr. Adolesc. Med. 158: 342-347 (Apr. 2004)
.")
46
Parent Weight Change as a Predictor of Child Weight Change in Family-Based Behavioral Obesity Treatment Family-based behavioral treatment Parenting techniques Reinforcement Stimulus control Environmental restructuring Obese parents make similar behavioral changes

47
Parent Weight Change as a Predictor of Child Weight Change in Family-Based Behavioral Obesity Treatment Participants 142 obese children (8-12yo) and at least one parent attended family-based weight control program 2-year study with measurements at 6, 12, and 24 months
 and at least one parent attended family-based weight control program 2-year study with measurements at 6, 12, and 24 months")
48
Parent Weight Change as a Predictor of Child Weight Change in Family-Based Behavioral Obesity Treatment Both child and parents lost significant amounts of weight over 6 and 24 months

49
Parent Weight Change as a Predictor of Child Weight Change in Family-Based Behavioral Obesity Treatment Parents who lost the most weight had children who lost the most weight.

50
Parent Weight Change as a Predictor of Child Weight Change in Family-Based Behavioral Obesity Treatment Conclusions: “Parent z-BMI change was a significant predictor of child z-BMI change over 6 and 24 months.” “…youth benefit the most from parents who lose the most weight in family-based behavioral programs.” “…support the inclusion of parents into family-based programs for their children.”

51
Reducing children’s television viewing to prevent obesity: A randomized controlled trial. T. Robinson JAMA 282:1561-1567 (1999)
.")
52
Reducing children’s television viewing to prevent obesity: A randomized controlled trial. Many observational studies have found associations between television viewing and child/adolescent adiposity. Reviewed in AAP’s Policy Statement Pediatrics 112:424-430 (2003) 25% children watch >4hrs TV/day BMI of children who watch >4hrs per day significantly greater than those watching < 2hrs per day TV in child’s bedroom significant predictor of overweight
 25% children watch >4hrs TV/day BMI of children who watch >4hrs per day significantly greater than those watching < 2hrs per day TV in child’s bedroom significant predictor of overweight.")
53
Reducing children’s television viewing to prevent obesity: A randomized controlled trial. 192 3 rd & 4 th grade children in two matched public elementary school Intervention group 18-lesson, 6-month classroom curriculum to reduce TV, videotape, and videogame use Measures at 0 and 8 months

54
Reducing children’s television viewing to prevent obesity: A randomized controlled trial. Compared to controls, children in intervention group had statistically significant relative decreases in BMI, TSF, waist circumference, and W/H ratio.

55
Reducing children’s television viewing to prevent obesity: A randomized controlled trial. The intervention significantly decrease children’s television viewing and video game use.

56
Reducing children’s television viewing to prevent obesity: A randomized controlled trial. However, reducing television viewing did not significantly reduce: Frequency of snacking in front of TV Daily servings of high-fat foods Or increase Overall physical activity Fitness “Reducing television… may be a promising, population-based approach to help prevent childhood obesity.”

57
Useful references American Academy of Pediatrics – Policy Statement Pediatrics 112:424-430(2003) Society for Nutrition Education Guidelines for Childhood Obesity Prevention Programs: Promoting Healthy Weight in Children J. Nutr. Ed. Behav. 35:1-3 (2003) Childhood and Adolescent Overweight: The Health Professional’s Guide to Identification, Treatment, and Prevention. M Mullen & J Shield ADA 2004
 Childhood and Adolescent Overweight: The Health Professional’s Guide to Identification, Treatment, and Prevention. M Mullen & J Shield ADA")
58
Addressing the issues of childhood and adolescent obesity July 25, Monday class debate You are either a group of RD’s lobbying in support for population-based approaches for preventing and treating overweight in children Nay-sayers who support status quo and believe strongly in personal responsibility and individual freedom

59
Addressing the issues of childhood and adolescent obesity July 25, Monday class debate On Thursday, July 22, RD’s must provide a brief list of their proposed population-based approaches to the naysayers. Debate format 10 minute presentation by RD’s 3-5 minute rebuttal by naysayers 3-5 minute response by RD’s

60
Addressing the issues of childhood and adolescent obesity July 25, Monday class debate School Board RDs: DO, AC, ED SQ: NA, KW Community RDs: KL, CV, LenaG SQ: KD, LK State/Federal RD’s: NS, LauraG, SL, SC SQ: DK, RS

Similar presentations

















 David L. Gee, PhD FCSN 547 – Nutrition Update Summer 2004.>")


