Download presentation
Presentation is loading. Please wait.

1
Combination Prevention as a Strategy Towards a Sustainable HIV free generation
Paper presented at the 6Th Joint Biennial HIV and AIDS Sector Review November Dar es salaam . Blue Pearl Hotel, Ubungo Plaza. BY R.O.SWAI, MD

2
Structure of Presentation
Background on evolution of HIV prevention strategies over time. Definition of CP and its rationale, Description of categories of combination prevention interventions and their key features Planning for combination prevention interventions Levels of evidence for Combination Prevention Interventions Implementing combination Prevention Take home messages

3
Prevention of HIV Transmission-1
HIV is a blood borne virus that is transmitted mainly through: Sexual behaviours, especially through penetrative sexual intercourse (vaginal or anal) with an infected person Sharing of HIV contaminated needles and syringes Mother to child transmission during pregnancy, labour and breast feeding Transfusion of blood and blood products
 with an infected person. Sharing of HIV contaminated needles and syringes. Mother to child transmission during pregnancy, labour and breast feeding. Transfusion of blood and blood products.")
4
Prevention of HIV Transmission-2
Prevention has been the cornerstone of the global HIV/AIDS response Initial HIV prevention efforts primarily focused on behavioural and biomedical strategies targeting individual sexual behaviours For almost two decades , Abstinence, Be faithful and Condom use (“ABC”), was the dominant prevention approach
, was the dominant prevention approach.")
5
Prevention of HIV Transmision-3
Initially, little attention was placed on social, cultural and material factors that shape and constrain the behaviours that put individuals at risk of contracting HIV. In late 1980s and early 1990s ABC approach was adopted by many governments, international organizations and NGOs. In 1996, discovery of HAART, diverted attention from HIV prevention strategies to scale up of treatment programmes.

6
Prevention of HIV Transmision-4
The formation of GFATM and PEPFAR two huge funding bodies, marked the start of large HIV prevention strategies delivered on global scale Despite these developments, during mid 2000s, it was evident that “ABC ’’approach alone was not enough to bring HIV under control. Societal constraints were recognized to be very effective in reducing the choices and autonomy of women, young people and marginalized groups in their sexual choices and individual behavior is often heavily influenced by broader socioeconomic, cultural, and environmental factors. (UNAIDS, 2011)
")
7
Status of Global HIV Prevention Efforts
With over 30 years of prevention efforts, HIV incidence and prevalence are still alarmingly high. About 2.3 million people were newly infected with HIV worldwide in 2012 and a total of 35.3 million people were living with HIV in2012. Human suffering toll due to HIV/AIDS is high (1.6 million adult and child deaths in 2012) and costs for lifetime ART for all 35.3 million PLHIV are exorbitant. Prevention is the single most important challenge of the global response to HIV/AIDS.
 and costs for lifetime ART for all 35.3 million PLHIV are exorbitant. Prevention is the single most important challenge of the global response to HIV/AIDS.")
8
Limitations of Global HIV Prevention Efforts.
Arsenal of effective prevention interventions is limited Implementation of effective prevention interventions at sufficient scale and intensity according to need has been difficult Interventions are scattered across geographic areas -as a result, synergies of multiple interventions are not realized. No sufficient targeting to key populations especially in concentrated and mixed epidemics No sufficient linkage of services, Prevention to prevention and prevention with other services.( PEPFAR,2009.)
")
9
Limitations of ABC Approach
The “ABC’’ approach was considered inadequate to control HIV because it had failed to take into account the diverse contents and behaviours that sustain HIV transmission.(different epidemics each requiring different responses) Prevention efforts should be tailored at individual level, community level and population level. Some countries considered as HIV prevention success stories, modified the “ABC” approach by implementing additional specific interventions based on the characteristic of their national HIV epidemics.
 Prevention efforts should be tailored at individual level, community level and population level. Some countries considered as HIV prevention success stories, modified the ABC approach by implementing additional specific interventions based on the characteristic of their national HIV epidemics.")
10
International Consensus on Combination Prevention
Combination Prevention concept was conceived in by the Global HIV Prevention Group Highlighted in discussions during 2008 IAC in Mexico with emphasis on refocusing HIV response on prevention. 2009 UNAIDS Outcome Framework acknowledged the role of CP in changing the trajectory of AIDS epidemic 2009 HIV/AIDS Implementers Meeting highlighted the need for partners to redouble efforts to achieve CP

11
Definition of Combination Prevention of HIV
“….rights-based, evidence-informed, and community-owned programmes that use a mix of biomedical, behavioural, and structural interventions, prioritised to meet the current HIV prevention needs of particular individuals and communities, so as to have the greatest sustained impact on reducing new infections.’’ (UNAIDS ,2010)
")
12
Rationale of Combination Prevention Concept
Virtually every sustained public health success has depended on the strategic combination of biomedical, behavioural and structural prevention strategies to address individual level risks and to create a more enabling environment for health (Wohlfeiler & Ellen, 2007). For the HIV response, countries that were successful in sustained reductions in new HIV infections, used a combination prevention approach. Such countries included Thailand , Uganda and Brazil .(UNAIDS, 2010)
. For the HIV response, countries that were successful in sustained reductions in new HIV infections, used a combination prevention approach. Such countries included Thailand , Uganda and Brazil .(UNAIDS, 2010)")
13
Prevention Success Story - Uganda
Was the first clear prevention success story in Sub Saharan Africa Implemented combined strategies included: Efforts to change social norms regarding partnership outside marriage (Zero grazing,) Investment in condoms (love carefully) Visible involvement of leaders at all levels of society Commitment to destigmatization of HIV Empowerment of PLHIV and affected communities
 Investment in condoms (love carefully) Visible involvement of leaders at all levels of society. Commitment to destigmatization of HIV. Empowerment of PLHIV and affected communities.")
14
Impact of Ugandan Prevention Success Story
The percentage of young people who were sexually active fell by more than half between and 1995. Ugandans were significantly less likely to have multiple sex partners than people living in neighbouring countries HIV prevalence among pregnant women was 15% in and dropped to 5% in ( UNAIDS, 2001)
")
15
Prevention Success Story - Thailand
Based on Strategic Information ,noted that the epidemic had shifted from IDU to sex workers and their clients. Therefore instituted a programme of: Community inclusion and caring for PLHIV High visibility of HIV through mass communication programme Promotion and provision of HTC Strengthening of STI services Built capacity of community based organizations Promoted 100% condom campaign in brothels Promoted male social norms changes regarding sex outside marriage New HIV infections declined from 143,000 in 1991 to 91,000 in (UNAIDS ,2006)
")
16
Prevention Success Story - Brazil
Brazil is noted for: Integration of prevention with treatment programmes Strong political support for a vigorous response Substantial resources allocated to key populations; PWUD, SW, MSM, trans gender people Massive condom promotion Provided access to quality STI services Community based social marketing to raise awareness and reduce risky behaviour Response grounded on human rights principles, social solidarity and community empowerment.

17
Impact of Brazilian Prevention success story
The World Bank had predicted in that 1.2 million Brazilians would be infected by 2000, however, fewer than 600,000 were living with HIV in (UNAIDS 2010).
.")
18
Common Themes in Prevention Success Stories
High-level involvement of political leadership, civil society and religious leaders Environmental and contextual factors e.g. socio- cultural, economic and legal factors that condition risk behavior ( broad based behaviour change). High visibility and open communication regarding HIV, sex, stigma and discrimination Interventions based on specific epidemic profile:eg Target “key populations” ( IDUs, MSMs, SW and clients) as appropriate No single intervention was found efficacious to bring HIV epidemic under control
. High visibility and open communication regarding HIV, sex, stigma and discrimination. Interventions based on specific epidemic profile:eg Target key populations ( IDUs, MSMs, SW and clients) as appropriate. No single intervention was found efficacious to bring HIV epidemic under control.")
19
Core programmatic components of Combination Prevention
Combination Prevention recognizes 3 broad categories of interventions: Behavioural Biomedical Structural

20
Behavioural Interventions
Include a range of sexual behavior change communication programs that use various communication channels (e.g., mass media, community-level, and interpersonal) to disseminate behavioral messages designed to encourage people to reduce behaviors that increase risk of HIV and increase protective behaviors (e.g., risks of having multiple partners and benefits of using a condom correctly and consistently). Behavior interventions also are aimed to increase the acceptability and demand for biomedical interventions. (PEPFAR, 2011).
 to disseminate behavioral messages designed to encourage people to reduce behaviors that increase risk of HIV and increase protective behaviors (e.g., risks of having multiple partners and benefits of using a condom correctly and consistently). Behavior interventions also are aimed to increase the acceptability and demand for biomedical interventions. (PEPFAR, 2011).")
21
Behavioural interventions include:
Sex education Harm reduction Peer education Mass communication messages through social media, press, advertising, campaigns, radio, etc Voluntary Counselling and Testing (VCT) Stigma and discrimination reduction programmes Cash transfer programmes
 Stigma and discrimination reduction programmes. Cash transfer programmes")
22
Biomedical Interventions
Are those that directly influence the biological systems through which the virus infects a new host, such as blocking infection (e.g., male and female condoms), decreasing infectiousness (e.g., ART as prevention), or reducing acquisition/infection risk (e.g., voluntary medical male circumcision). (PEPFAR ,2011)
, decreasing infectiousness (e.g., ART as prevention), or reducing acquisition/infection risk (e.g., voluntary medical male circumcision). (PEPFAR ,2011)")
23
Examples of biomedical interventions
Male and females condoms Male circumcision Voluntary Counselling and Testing (VCT) Testing and treatment of sexually transmitted Infections(STI) Needle Exchange Programmes (NEP) Opinoid Substitution Treatment (OST) Universal healthcare precautions Blood screening Antiretroviral drugs for Prevention of mother to child transmission (PMTCT), Pre exposure Prophylaxis (Prep) Post Exposure prophylaxis (PEP); and Treatment as Prevention (TasP) Microbicides and Vaccines The Lancet 372 (9637)56
 Testing and treatment of sexually transmitted Infections(STI) Needle Exchange Programmes (NEP) Opinoid Substitution Treatment (OST) Universal healthcare precautions. Blood screening. Antiretroviral drugs for Prevention of mother to child transmission (PMTCT), Pre exposure Prophylaxis (Prep) Post Exposure prophylaxis (PEP); and Treatment as Prevention (TasP) Microbicides and Vaccines The Lancet 372 (9637)56.")
24
Structural interventions-1
Address the critical social, legal, political, and environmental enablers that contribute to the spread of HIV. Five categories can be used to describe structural interventions: legal and policy reform, reducing stigma and discrimination against people living with HIV and marginalized groups, gender inequality and gender-based violence, economic empowerment and other multi-sectoral approaches, and education. (PEPFAR ,2011.)
")
25
Structural Interventions-2
Also, Structural interventions seek to address underlying factors that make individuals or groups vulnerable to HIV infection; these may be social, economic, political, or environmental. (Rao G,et al ,2008.)
")
26
Examples of Structural Interventions
Decriminalizing sex work; homosexuality and drug use Law reforms to protect people living with HIV and address gender inequalities Interventions that address poverty: e.g. microfinance programmes; programmes for gender based violence Addressing stigma and discrimination towards key populations Kim J. et al, (2011) The Lancet 372 (9637)
 The Lancet 372 (9637)")
27
Key Features of Combination Prevention Interventions-1
Carefully tailored to national and local needs and conditions- i.e. they are based on current information on the modes of transmission, the populations or groups most at risk of exposure and transmission, and the context that shape their risk and vulnerability They are strategic mix of structural as well as biomedical and behavioral approaches that are required to meet the needs of those groups, focusing both on their immediate risks and underlying causes of vulnerability. Through structural interventions they create a more enabling environment for prevention action.

28
Key Features of Combination Prevention Interventions-2
Are planned to operate synergistically and consistently over time, on the multiple levels that reinforce or challenge risk behaviour. Investments prioritized strategically and with the full engagement of affected communities, mobilizing resources in the community, the private sector, government and internationally to achieve needed participation, coverage and continuity.

29
Key Features of Combination Prevention Interventions-3
They require, benefit from, and invest in enhanced partnership and coordination in the design, resourcing and management of programmes, with special attention to investment in decentralized and community responses. They incorporate sufficient flexibility to permit ongoing assessment, improvement of strategies, and use of new tools and approaches to enable strategies to evolve in response to epidemiological, technological, or social changes.

30
Evidence of Impact Review of selected Interventions:
Male and female condoms HIV Testing and Counselling (HTC) Control of Sexually Transmitted Infections (STI) Voluntary Male Medical Circumcision(VMMC) Microbicides for HIV Prevention ART Treatment for HIV Prevention (TasP) Behavioural Interventions
 Control of Sexually Transmitted Infections (STI) Voluntary Male Medical Circumcision(VMMC) Microbicides for HIV Prevention. ART Treatment for HIV Prevention (TasP) Behavioural Interventions.")
31
Levels of evidence for elements of Combination Prevention .
The highest level and most powerful evidence of any intervention is impact on HIV incidence(avert new infections). Other types of evidence include; behavioral and biological outcomes
. Other types of evidence include; behavioral and biological outcomes.")
32
Evidence of Impact of Condoms
Male condoms have about 90% efficacy in preventing sexual transmission and acquisition of HIV and other STIS including gonorrhea, chlamydia and Trichomoniasis when used correctly and consistently. 100% condom use campaign brought down the HIV epidemic inThailand. Female condoms efficacy is also high about 80-90%; Use of condoms also appear to reduce risk of HSV associated diseases(genital warts and cervical cancer). Guidance for the Prevention of Sexually Transmitted HIV infections, PEPFAR 2011.
. Guidance for the Prevention of Sexually Transmitted HIV infections, PEPFAR")
33
How to make Condom Programming for HIV Prevention Successful:
Regular, sufficient, and uninterrupted supply of male and female condoms Demand creation with emphasis and focus at all high risk settings (e.g. alcohol venues) for casual and commercial sex; and reach mobile populations, uniformed forces, prisons, MSM Emphasize secondary prevention among PLHIV and among discordant couples. Use Pregnant women as entry point for condom use in couples. Destigmatize use of condom. Do not link it with sex work/casual sex or lack of trust.
 for casual and commercial sex; and reach mobile populations, uniformed forces, prisons, MSM. Emphasize secondary prevention among PLHIV and among discordant couples. Use Pregnant women as entry point for condom use in couples. Destigmatize use of condom. Do not link it with sex work/casual sex or lack of trust.")
34
Evidence of HIV Testing and counselling for HIV Prevention
Limited population-level impact of HTC shown for HIV prevention except in discordant couples and for HIV + clients (most of whom will take measures not to infect others). BUT HIV Counselling and testing (VCT, PITC, home based testing)has been shown to be: Essential entry point for PMTCT and Care and treatment and linkage and referral to other services May contribute to opening up the epidemic and to reducing stigma and discrimination Critical and useful in identifying discordant couples For HCT to make impact on behaviour change, services must be of high quality and accessible on continuous basis
. BUT HIV Counselling and testing (VCT, PITC, home based testing)has been shown to be: Essential entry point for PMTCT and Care and treatment and linkage and referral to other services. May contribute to opening up the epidemic and to reducing stigma and discrimination. Critical and useful in identifying discordant couples. For HCT to make impact on behaviour change, services must be of high quality and accessible on continuous basis.")
35
HTC contribute to opening up and to reducing stigma and discrimination
In Tanzania , in 2007, following the Head of State and First Lady taking the HIV test in public, stigma around HIV and testing melted away. In a period of one year that followed that event , about 5 million people came forward for Voluntary counselling and testing. Before that , in period of ten years, only two million people tested for HIV. Ever since, the momentum of testing has continued and cumulatively about 20 million people have tested.

36
4/16/2017

37
Section of the crowd attending the launching day- July 14, 2007
4/16/2017

38
4/16/2017

39
4/16/2017

40
4/16/2017

41
People of different social backgrounds and status waiting for the testing
4/16/2017

42
Evidence of STI Control for HIV Prevention-1
STIs including those asymptomatic increase susceptibility to HIV infection 2-5 fold for several reasons: Direct damage/disruption to genital mucosa Inflammatory process increase proliferation of immune cells that are also target for HIV Higher HIV load in genital secretions Among 7 randomized control studies conducted to date, only one of them ,conducted in Tanzania was able to demonstrate decline of HIV by 40% as a result of STI treatment

43
Evidence of STI Control for HIV Prevention-Syndromic Management
Syndromic Management is OK BUT: Misses asymptomatic infections, especially in women women; Does not treat viral STIs In many countries in ESA, viral STIs now predominate, esp Herpes Simplex Virus-2 and will not respond to syndromic management Syndromic management greatly reduced bacterial STIs, so it has probably contributed to lower peaks in HIV prevalence Syndromic management is not a proven prevention strategy for HIV but should form part of package for AIDS related services

44
Evidence of Voluntary Medical Male circumcision for HIV Prevention -1
Voluntary Medical Male circumcision is the surgical removal of the foreskin from the penis by trained medical personnel under aseptic conditions For past 20 years, over 45 observational studies have shown that MC reduces heterosexual transmission of HIV significantly In West Africa, where MC is widely practised, the population level effect of MC was observed by keeping the prevalence of HIV low for many years

45
Evidence of VMMC circumcision for HIV Prevention-2
Three Randomized Clinical Trials carried out in Orange Farm, South Africa (2005); Kisumu, Kenya (2006) and Rakai, Uganda (2006) - all showed that VMMC reduced men's risk of HIV acquisition by % Extended follow up of participants at up to 5years post trial indicated that the protective effect increased to 68% Modelling suggests that MC could avert 5.7 million infections and 3 million deaths over next twenty years in SSA
; Kisumu, Kenya (2006) and Rakai, Uganda (2006) - all showed that VMMC reduced men s risk of HIV acquisition by % Extended follow up of participants at up to 5years post trial indicated that the protective effect increased to 68% Modelling suggests that MC could avert 5.7 million infections and 3 million deaths over next twenty years in SSA.")
46
Evidence of VMMC circumcision for HIV Prevention-3
VMMC must be combined with behaviour change especially partner reduction, counselling and testing and condom use and treatment of STI WHO and UNAIDS recommend that VMMC should be actively promoted as part of preventive efforts in settings where circumcision rates are low and HIV prevalence is high No evidence of VMMC in preventing HIV infection in penile anal intercourse. The effect of circumcision on male to female HIV transmission has not been extensively and conclusively researched. Some studies have shown protective effect while others did not. Regardless of direct benefit to women, properly implemented VMMC programme that lower HIV prevalence in male population would thereby also reduce women's risk of exposure to men infected with HIV Weiss at al (2009).The Lancet Infectious Diseases 9(11)
.The Lancet Infectious Diseases 9(11)")
47
Evidence of Microbicides for HIV Prevention
In 2010, South African Researchers in a project named CAPRISA 004, found that 1% tenofovir gel reduced women’s risk of acquiring HIV from male partners by 39% overall and maximal reduction of 54% in women who were most adherent. This study involved 889 high-risk women who used 1% tenofovir gel vaginally up to 12 hours before intercourse and within 12 hours after intercourse. Also noted in the CAPRISA trial that Tenofovir 1% inhibits HSV-2 replication, and reduced acquisition of HSV-2. These interventions are awaiting further trials,

48
Evidence of HIV Treatment for HIV Prevention (T4P)
In May 2011, research findings from clinical trial HPTN 052 involving 1763 serodiscordant couples in 13 sites in 9 countries in Africa, Asia and United states showed that ART can reduce HIV transmission by 96% 27 HIV transmissions occurred in the 877 couples in delay group compared to 1 transmission in 886 couples in the immediate group (p<0.0001) Previous to that, metanalysis estimated the level of treatment for Prevention (T4P) to be 92%
 Previous to that, metanalysis estimated the level of treatment for Prevention (T4P) to be 92%")
49
Evidence of Behaviour Interventions for Prevention of Sexual Transmission of HIV
Behavioral interventions promote a range of objectives related to reducing HIV transmission. These include: Abstinence Delay of sexual debut Monogamy Fidelity Partner reduction

50
Categories of Behavioral Interventions
Behavioural interventions fall under two broad categories: Standalone interventions that seek to minimize sexual risk behaviurs or increase protective behaviour Supportive interventions that seek to optimize biomedical interventions by creating demand for service and improve adherence and after care

51
Evidence of Impact of behavioural Interventions
Mass media has been demontrated changes in intermediary indicators such as ;Knowledge, risk perception and self efficacy Mass media has also been linked to positive behavioural outcomes such as ; delay in sexual debut, decrease in numbers of sexual partners, increase in condom use and utilization of HTC and PMTCT services Mass media is most effective when used to promote branded products and programmes and to compliment other community and interpersonal activities -(Guidance for the Prevention of Sexually Transmitted HIV infections, PEPFAR 2011).
.")
52
Planning for Combination Prevention.
Knowing the realities of a county is the basis for identifying, selecting and funding the most appropriate and effective HIV prevention measures Should be an open , inclusive and transparent process to identify key prevention priorities and guide resources allocation. Key stakeholders: PLHIV, Strategic Govt Ministries, Key affected populations, Women groups ,Private sector, Community and cultural leaders, and Individuals with relevant research and evaluation expertise (UNAIDS,2011.)
")
53
Key milestones in Combination Prevention Planning Process-1
An effective portfolio of HIV prevention interventions is based on having and using accurate and comprehensive information about both the epidemic and the current response, commonly referred to as ―Know Your Epidemic, Know Your Response. This involves: Identifying relatives modes of transmission modes – sex , IDU Identification of key affected populations and most in need of services.

54
Key milestones in Combination Prevention Planning Process-2
Identification of geographic patterns including urban/rural prevalence, which will enable focus services where most needed Estimating the size of key populations affected to guide implementation Document structural factors (social, legal, economic and cultural) e.g punitive laws and gender imbalance that might fuel risk and vulnerability of HIV.
 e.g punitive laws and gender imbalance that might fuel risk and vulnerability of HIV.")
55
Key milestones in Combination Prevention Planning Process-3
Describing the current national response to help undertake gap analysis. This includes mapping all prevention activities with geographical and population coverage Articulating a coordinated mix or combination that is tailored to meet the local needs of the epidemic .

56
Implementing Combination Prevention
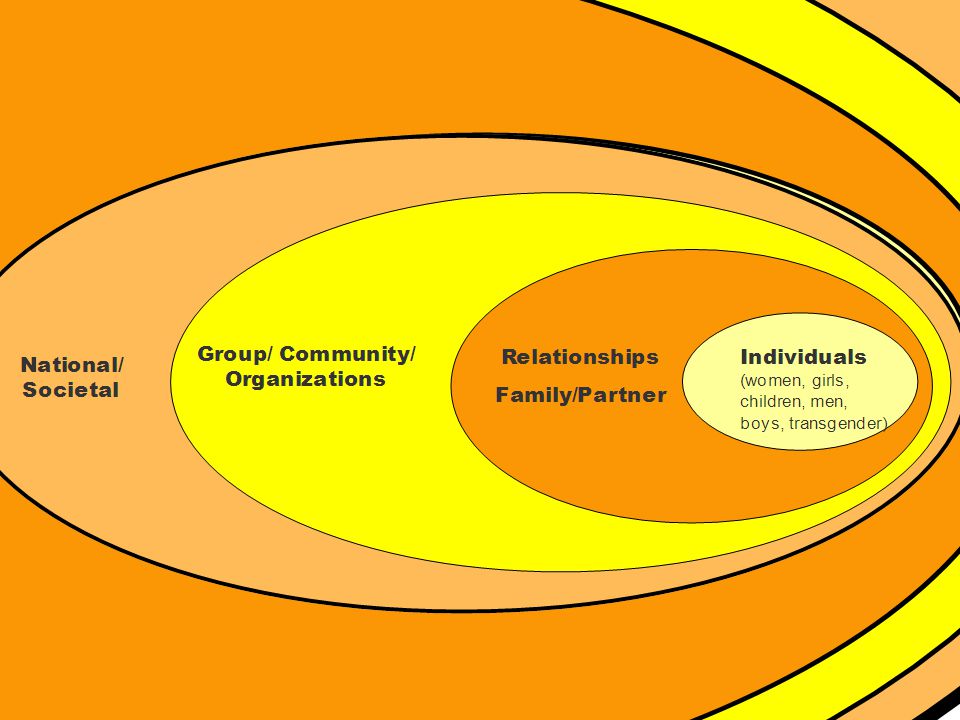
Different classes of prevention strategies should operate at multiple levels (individual, relationship, community and societal) These strategies should respond to the needs of particular audiences and modes of HIV transmission and make efficient use of resources through prioritization, partnership and engagement of affected communities UNAIDS Prevention Reference Group
 These strategies should respond to the needs of particular audiences and modes of HIV transmission and make efficient use of resources through prioritization, partnership and engagement of affected communities. UNAIDS Prevention Reference Group.")
58
Challenges of Combination Prevention Implementation
CP widely acknowledged but seldom and poorly implemented; why: Failure to address key populations at risk Failure to focus resources on primary prevention routes and unexplained variations from year to year Deficit of structural interventions to address causes of vulnerability Inadequate prevention services for People living with HIV ( UNAIDS Discussion Paper ,2010.)
")
59
Take Home Messages HIV prevention response focusing on individuals with biomedical and behavioural interventions is not sufficient to bring the HIV epidemic under control. Combination prevention is a strategic, evidence informed combination of biomedical, behavioural and structural strategies in a human rights framework. Combination Prevention is the right approach for a sustained, long term response that will lead to an AIDS free generation.

60
Conclusion What is the status of Implementation of Combination Prevention in the Tanzanian HIV/AIDS Response? Is the scale, intensity and quality of CP sufficient? Do Prevention portfolios focus on populations and behaviors that actually drive the epidemic and at the location where the risk behaviors are most likely to occur?

61
Thank you.

Similar presentations








>")










