Download presentation
Presentation is loading. Please wait.

1
HYPERPARATHYROIDISM Hasan Aydın M.D. Endocrinology and Metabolism Yeditepe University Medical Faculty

2
Hyperparathyroidism A clinical syndrome characterized by –↑ PTH, –PTH induced bone resorption –Hypercalcemia

3
Types of Hyperparathyroidism - Primary - Secondary - Tertiary

4
Primary Hyperparathyroidism

5
Excessive, relatively uncontrolled secretion of PTH One or more hyperfunctioning parathyroid glands. Hypercalcemia, the biochemical hallmark Most patients today are relatively asymptomatic. Symptoms remarkably varied and vague.

6
Epidemiology Overall incidence is 42 in 100,000 Incidence increases with age Most patients with sporadic primary hyperparathyroidism are postmenopausal women with an average age of 55 years Female to male ratio is 2-3:1

7
Etiology and Pathogenesis Primary hyperparathyroidism is caused by …..Parathyroid adenoma – 80% …..Parathyroid hyperplasia – 15% …..Parathyroid carcinoma – 1-2% …..Approximately 10% are caused by “double adenoma” It can occur as part of at least three familial endocrinopathies …..MEN 1 …..MEN 2A …..Isolated familial hyperparathyroidism

8
Manifestations Renal Skeletal Gastrointestinal Neurologic-Neuromuscular Other

9
Symptoms and Signs Renal –hypercalciuria –nephrolithiasis –nephrocalcinosis –polyuria and polydipsia –renal insufficiency Neuromuscular –weakness –myalgia

10
Symptoms and Signs Neurologic and psychiatric - Memory loss - Confusion -Depression - Lethargy -Psychosis - Fatigue -Paresthesias Skeletal -Bone pain -Osteoporosis -Pathologic fractures -Bone cysts/brown tumors -Arthralgias -Chondrocalcinosis -Pseudogout and gout -Subperiosteal skeletal resorption

11
Symptoms and Signs Peptic ulcer –Zollinger-Ellison Syndrome ( MEN 1) Chronic pancreatitis
 Chronic pancreatitis")
12
Other Manifestations Polyuria, polydipsia, constipation ECG changes (shortened Q-T ) Band keratopathy, subconjunctival deposits Pruritus Ectopic calcifications ( lungs, kidneys, skin, arteries ) Hypertension
 Band keratopathy, subconjunctival deposits Pruritus Ectopic calcifications ( lungs, kidneys, skin, arteries ) Hypertension")
13
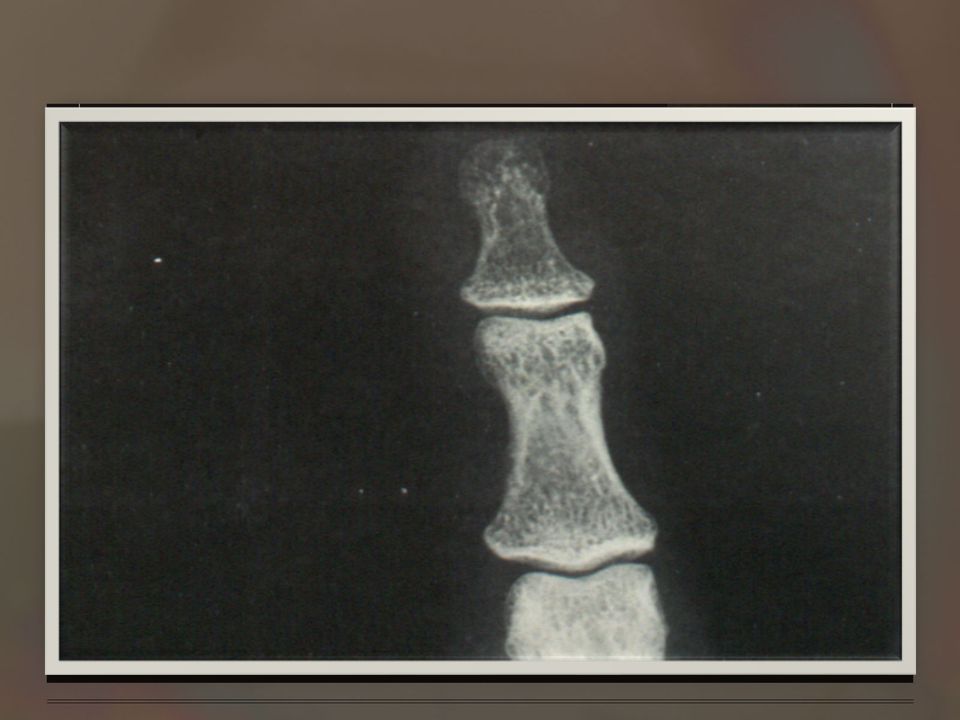
Hyperparathyroid Bone Disease Elevation of the alkaline phosphatase level Osteitis fibrosa cystica Subperiosteal resorption of cortical bone (phalanges) A salt-and-pepper appearance (in the skull) Bone cyst or brown tumors (jaw) Loss of the lamina dura of the teeth Osteoporosis (predominant loss of cortical bone)
 A salt-and-pepper appearance (in the skull) Bone cyst or brown tumors (jaw) Loss of the lamina dura of the teeth Osteoporosis (predominant loss of cortical bone)")
16
Osteitis Fibrosa Cystica

17
Classical Phrase

18
Laboratory Findings Hypercalcemia is universal (>10.6 mg/dL) Serum phosphorus is low normal (<3.5 mg/dl) or low (<2.5 mg/dl) Mild hyperchloremic metabolic acidosis PTH is elevated or high normal Alkaline phosphatase may be increased
 Serum phosphorus is low normal (<3.5 mg/dl) or low (<2.5 mg/dl) Mild hyperchloremic metabolic acidosis PTH is elevated or high normal Alkaline phosphatase may be increased")
19
Work-Up Rule out lithium or thiazide use Wrist, spine and hip DEXA Consider IVP or CT to evaluate for kidney stones Ionized calcium versus serum calcium—the debate rages on….

20
Differential Diagnosis Due to increased serum PTH –Primary and ''tertiary'' hyperparathyroidism –Nonhematologic malignant neoplasms Not due to increased serum PTH –Drug-induced (thiazide, furosemide, vitamin D, calcium, vitamin A, lithium) –Granulomatous (sarcoidosis, tuberculosis, berylliosis) –Genetic (familial hypocalciuric hypercalcemia) –Immobilization –Idiopathic –Nonhematologic malignant neoplasms –Malignant hematologic diseases –Nonparathyroid endocrine disease (Addison's disease, hyper and hypothyroidism)
 –Granulomatous (sarcoidosis, tuberculosis, berylliosis) –Genetic (familial hypocalciuric hypercalcemia) –Immobilization –Idiopathic –Nonhematologic malignant neoplasms –Malignant hematologic diseases –Nonparathyroid endocrine disease (Addison s disease, hyper and hypothyroidism)")
21
Differential Diagnosis of Osteitis Fibrosa Cystica Paget’s disease of bone Osteoporosis Osteomalacia Malignant diseases Polyostotic fibrous dysplasia Secondary hyperparathyrodism Pseudohypoparathyroidism

22
Differential Diagnosis of Nephrolithiasis/Nephrocalcinosis Gout Hyperoxaluria Renal tubular acidosis Pyelonephritis

23
Treatment Definitive treatment is surgical parathyroidectomy Cure rate for adenomas >95% (less for hyperplasia) No value in pre-op studies to localize parathyroid tumors The only localization study needed is to locate an experienced parathyroid surgeon No definitive medical therapy for hyperparathyroidism
 No value in pre-op studies to localize parathyroid tumors The only localization study needed is to locate an experienced parathyroid surgeon No definitive medical therapy for hyperparathyroidism")
24
In the asymptomatic patient, who should undergo surgery?

25
Indications for Surgery Overt clinical manifastations of primary hyperparathyroidism –Radiographic nephrolithiasis or documented renal stones –Reduced creatinine clearance (not otherwise explained) –Radiographically evident hyperparathyroid bone disease –Classical hyperparathyroid neuromuscular disease –Symptoms attributable to hypercalcemia per se –Previous episode of life threatening hypercalcemia Serum Ca concentration >12 mg/dL Low or declining bone mineral density –>2 SD below age/sex matched controls (any site) or –Vertebral osteopenia or –Declining vertebral bone mineral density Age younger than 50 years Uncertain prospect for successful monitoring –Patient requests surgery –Consistent followup seems unikely –Coexistent illness that may contribute to or confound detection of, disease progression
 –Radiographically evident hyperparathyroid bone disease –Classical hyperparathyroid neuromuscular disease –Symptoms attributable to hypercalcemia per se –Previous episode of life threatening hypercalcemia Serum Ca concentration >12 mg/dL Low or declining bone mineral density –>2 SD below age/sex matched controls (any site) or –Vertebral osteopenia or –Declining vertebral bone mineral density Age younger than 50 years Uncertain prospect for successful monitoring –Patient requests surgery –Consistent followup seems unikely –Coexistent illness that may contribute to or confound detection of, disease progression")
26
Other Considerations in Surgical Referral Neuropsychological abnormalities –Several studies document improvement in HRQL after parathroidectomy –Studies on neurobehavioral abnormalities have reported less consistent results with parathyroidectomy Cardiovascular abnormalities –Symptomatic patients suffer from increased cardiovascular mortality before and after treatment –Asymptomatic primary HPT is associated with LVH; some studies suggest this is reversible with parathyroidectomy –Primary HPT patients have increased calcifications of mitral and aortic valve Perimenopausal women –Asymptomatic primary HPT associated with increased bone turnover, reduced bone mineral density and higher risk for fractures

27
Pre-Operative Imaging High-resolution ultrasound –Sensitivity 65-85% for adenoma; 30-90% for enlarged gland –Results suboptimal in pts with multinodular thyroid disease, pts with short thick neck, ectopic glands (15-20%) –May be useful in detecting sestamibi scan negative adenomas CT with contrast/thin section –Sensitivity of 46-87% –Good for ectopic glands in the chest MRI –Sensitivity of 65-80% –Good for ectopic glands Sestamibi –85-95% accurate in localizing adenoma in primary HPT Sestamibi-SPECT –Sensitivity 60% for enlarged gland and 98% for solitary adenomas
 –May be useful in detecting sestamibi scan negative adenomas CT with contrast/thin section –Sensitivity of 46-87% –Good for ectopic glands in the chest MRI –Sensitivity of 65-80% –Good for ectopic glands Sestamibi –85-95% accurate in localizing adenoma in primary HPT Sestamibi-SPECT –Sensitivity 60% for enlarged gland and 98% for solitary adenomas")
28
Ultrasonographic Localization

29
Traditional Sestamibi Sestamibi-SPECT Scintigraphy Images

30
MRI Localization

31
Medical Management Primary HPT Bisphosphonates –Studies have shown increase in lumbar spine and femoral neck mineral density Calcimimetic agents (Cinacalcet) –For intractable case of primary HPT Estrogen –Dose required is high SERMs –Reduction in serum calcium and markers of bone turnover after 4 weeks
 –For intractable case of primary HPT Estrogen –Dose required is high SERMs –Reduction in serum calcium and markers of bone turnover after 4 weeks")
32
Medical Treatment Chronic moderate (12-15 mg/dL) hypercalcemia –The drug of first choice for most patients is pamidronate disodium. This is a biphosphanate drug that acts by inhibiting osteoclastic bone resorption. The initial dose is 60-90 mg by intravenous infusion over 4-24 hours. –Glucocorticoids-(hypercalcemia associated with hematologic malignancies)
.")
33
Medical Treatment Mithramycin- inhibition of bone resorption, (hematologic and solid malignant disorders). Phosphate- lncreases in serum phosphorus above 5 mg/dL should be avoided because of the danger of inducing extraskeletal calcifications. Calcitonin-4-8 IU/kg Estrogen Other agents- - and -adrenergic blockers and cimetidine

34
Medical Treatment Acute severe (> 15 mg/dL) hypercalcemia-. a. Hospitalization-(immobilization may increase serum calcium in some patients) b. Calcium restriction c. Reduction of digitalis d. Hydration and diuretics- 4-6 L of isotonic saline IV+ furosemide 20-100 mg every 1-2 hours or ethacrynic acid 10- 40 mg every 1-2 hours
 b. Calcium restriction c. Reduction of digitalis d. Hydration and diuretics- 4-6 L of isotonic saline IV+ furosemide mg every 1-2 hours or ethacrynic acid mg every 1-2 hours.")
35
Maintenance Regimen Furosemide ( 40-160 mg/d orally) or ethacrynic acid (50-200 mg/d orally), Sodium chloride tab (400-600 mEq/d orally) At least 3 L of fluid per day Other drugs- (1) Indomethacin- (2) Mithramycin-
 or ethacrynic acid ( mg/d orally), Sodium chloride tab ( mEq/d orally) At least 3 L of fluid per day Other drugs- (1) Indomethacin- (2) Mithramycin-")
36
Treatment Categories Criteria Preferred Treatment 1. One or more of the following: Surgical removal of Serum calcium > 11 mg/dl. parathyroid lesion Osteitis fibrosa cystica. Metabolically active nephrolithiasis Decreased renal function. Intractable peptic ulcer. Pancreatitis. Serious psychiatric disease. Severe hypertension.

37
Treatment Categories Unsuccessful surgery, or recurrence with manifestations; noted in category 1 Serum calcium < 11 mg/dl. Abnormal serum iPTH Absence of manifestations noted in category 1 Surgery contraindicated. Surgical removal of parathyroid lesion; preoperative localization may be indicated Surgical removal of parathyroid lesion or medical management Medical management for hypercalcemia and nephrolithiasis prevention

38
Extent of Parathyroidectomy Number of Glands Involved Procedure All 4 Removal of 3 glands and all but 35- 50 mg of the fourth gland Two or 3 Removal of all but half of a normal gland; suture tagging of remaining half. One Removal of involved gland; identification of remaining glands (often by biopsy)
.")
39
Ectopic Parathyroids In several studies the abnormal parathyroid glands were found in the following sites. –30 to 54 percent were in the neck. –16 to 34 percent were in the mediastinum. –14 to 39 percent were retro-esophageal. –5 percent were in the aortic arch area. –8 percent were in the upper cervical area. –A few were in the carotid sheath.

40
Secondary HPT Clinical presentation –Usually asymptomatic Diagnosis –Elevated PTH in the setting of low or normal serum calcium is diagnostic –If phosphorous is elevated, cause is renal –If phosphorous is low, other causes of vit D deficiency should be sought Prevention –Vit D replacement –Phosphorus binders Treatment –Medical Calcimimetic agents –Surgical Considered in cases of refractory severe hypercalcemia, severe bone disease, severe pruritis, calciphylaxis, severe myopathy

41
Secondary Hyperparathyroidism of Chronic Renal Failure Associated with prolonged stimulation of the parathyroid glands by chronic decreases in the concentration of ionic calcium in the blood. Serum iPTH progressively increases as glomerular filtration rate decreases below 40 ml/min. Increases in serum phosphorus concentrations at this same level of GFR (40 mU/min)
.")
42
Secondary Hyperparathyroidism of Chronic Renal Failure

43
Major Causes of Chronic Hypocalcemia in Renal Failure Dietary deficiency of vitamin D or calcium. Decreased intestinal absorption of vitamin D or calcium due to primary small bowel disease, short bowel syndrome, and postgastrectomy syndrome. Drugs that cause rickets or osteomalacia such as phenytoin, phenobarbital, cholestyramine, and laxatives. States of tissue resistance to vitamin D. Excessive intake of inorganic phosphate compounds. Pseudohypoparathyroidism. Severe hypomagnesemia. Chronic renal failure.

44
Tertiary Hyperparathyroidism –Develops in patients with long-standing secondary hyperparathyroidism, which stimulates the growth of an autonomous adenoma. –A clue to the diagnosis of tertiary hyperparathyroidism is intractable hypercalcemia and/or an inability to control osteomalacia despite vitamin D therapy. Surgical Referral - calcium- phosphate product > 70 - severe bone disease and pain -intractable pruritus - extensive soft tissue calcification with tumoral calcinosis -calciphylaxis

45
In Conclusion Primary hyperparathyroidism is mostly caused by an adenoma Most of the patient asymptomatic Definitive treatment with surgery Differentiated from secondary and tertiary hyperparathyroidism

46
T h a n k Y o u

Similar presentations









![Clinical aspects of common mineral disorders. hypocalcemia Normal [Ca2+] total = 8.5-10.5 mg/dl (2.12-2.62 mmol/L) Normal [Ca2+] ion = 4.65-5.25 mg/dL.](/15/4762424/big_thumb.jpg "Clinical aspects of common mineral disorders. hypocalcemia Normal [Ca2+] total = 8.5-10.5 mg/dl (2.12-2.62 mmol/L) Normal [Ca2+] ion = 4.65-5.25 mg/dL.>")










