Download presentation
Presentation is loading. Please wait.

1
Diabetes and Obesity- The Way Forward? Diabetes and Obesity- The Way Forward? Dr A K Gupta Feb 17, 2005

2
Structure of the session Diabetes- The Problem – Extent of the problem – Twin epidemic of obesity and diabetes – Cost to the individual and society Risk factors for diabetes – Role of obesity Evidence so far – Primary prevention –focus on obesity Group work: Discussion of few questions and issues

3
What Is Diabetes? Definition: Diabetes Mellitus is a group of metabolic diseases characterised by hyperglycaemia resulting from defects in insulin secretion, insulin action, or both. Associated with damage to: – Eyes – Kidneys – Vascular system – Nervous system

4
Diabetes- The Epidemic

5
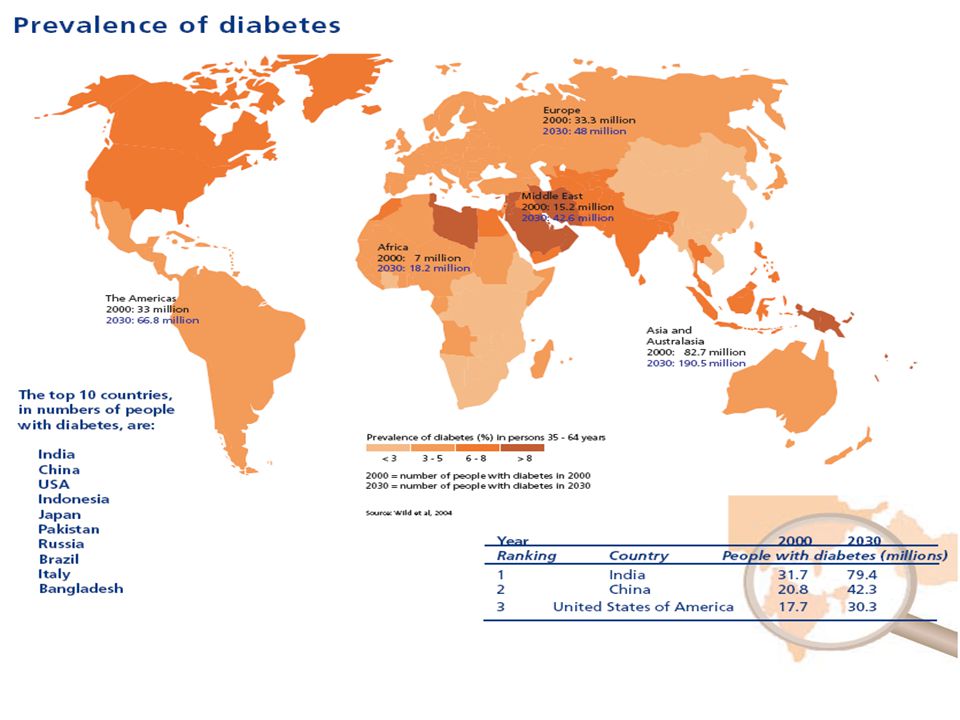
0 1995200020052010201520202025 2030 100 150 300 350 50 200 250 Diabetes – Prevalence Year 2000: 177 million Year 2030: 370 million. equivalent to 2/3 rd of europe population

7
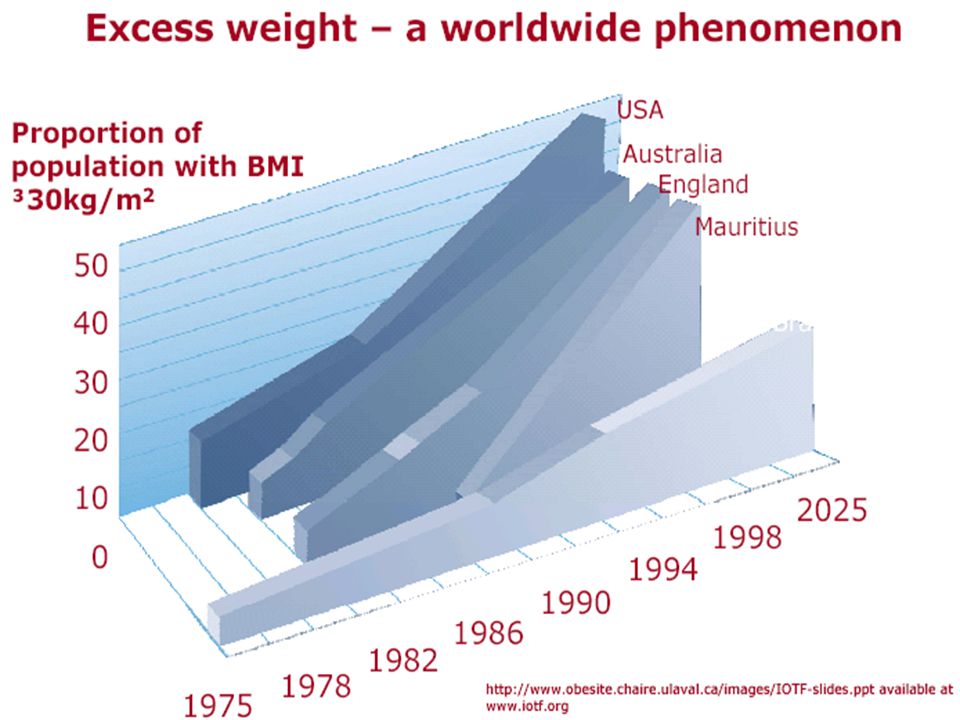
Obesity Obesity worldwide prevalence – 1995-200 million – 2000-300 million Developed world – US – prevalence estimates 1994:22.9% 1999: 30.5% 2008: 40% – UK: similar rates, tripling of prevalence between 1980 - 1997

9
Copyright restrictions may apply. Mokdad, A. H. et al. JAMA 2001;286:1195-1200. Prevalence of Obesity Among US Adults

10
Copyright restrictions may apply. Mokdad, A. H. et al. JAMA 2001;286:1195-1200. Prevalence of Diagnosed Diabetes Among US Adults

11
Diabetes caused by excessive weight

12
Diabetes : A dangerous disease

13
Diabetes : The Problems Retinopathy Common cause of blindness in people of working age in West Nephropathy 20% of all ESRD Erectile Dysfunction May affect up to 50% Macrovascular 2–4 x increased risk of CVD, 75% have hypertension 2–4 x increased risk of CVD, 75% have hypertension Foot Problems 15% develop foot ulcers; 5–15% need amputation The Audit Commission. Testing Times. A Review of Diabetes Services in England and Wales, 2000.

14
Mortality in Diabetes Diabetic patients without previous MI have as high a risk of MI as non-diabetic patients with previous MI New England Journal of Medicine 1998;339:229–234. Without previous MI previous MI With previous MI previous MI 7-year incidence of MI (%) 7 year follow-up
 7 year follow-up.")
16
Costs- Fact File Studies have shown that diabetes is a costly disease Type 2 diabetes accounted for between 3% and 6% of total healthcare expenditure in eight European countries Hospital in-patient costs are the largest single contributor to direct healthcare costs

17
Estimated total direct healthcare costs of diabetes in selected European countries Country General healthcare cost per patient (US$) Additional cost due to presence of diabetes (US$) Annual cost per patient with type 2 diabetes (US$) Belgium1,4951,6473,142 France1,9791,0092,988 Italy1,2591,6112,870 Sweden1,7108552,565 United Kingdom 1,1448812,025 Source: Diabetes Atlas, International Diabetes Federation
 Additional cost due to presence of diabetes (US$) Annual cost per patient with type 2 diabetes (US$) Belgium1,4951,6473,142 France1,9791,0092,988 Italy1,2591,6112,870 Sweden1, ,565 United Kingdom 1, ,025 Source: Diabetes Atlas, International Diabetes Federation")
18
Risk Factors for Type 2 DM Non Modifiable – Age (?40 or more) – First degree relative with Type 2 DM – Ethnicity – History of GDM Modifiable – BMI (?25 or more) – Habitual physical inactivity – ? Previously identified glucose intolerance Best single predictor – Presence of other “Syndrome X” abnormalities – ? Psychosocial Stress /and presence of major depressive episodes

19
Obesity and type 2 diabetes Chan et al (1994) and Colditz et al (1995)
 and Colditz et al (1995)")
20
Diabetes and Obesity Females of BMI >35 has 93 times the risk of developing diabetes compared to those with BMI<21 Increase in mean weight by one kg increase the risk of diabetes by 4.5% ( recent data - 9%) Ethnic populations e.G. Pima Indians, Samoans- changed lifestyles, become more obese- diabetes Not all obese have diabetes, but most of people with diabetes have excess weight

21
“58%of Diabetes Cases Globally Can Be Attributed to Body Mass Index Above 21 Kg/m2” Source: IDF Press Release August 25, 2003

22
Type 2 Diabetes: Fatness Vs Fitness Source: Wei et al 1999

23
‘Obesity and physical activity are the most preventable risk factors for diabetes, and could potentially lead to more than 50% reduction in prevalence of the diabetes’

24
Criteria for Undertaking Community- based Interventions Common and serious disease Strong causal relationships between risk factor levels and disease risk Predominantly social factors which determine risk levels e.g. lifestyle behaviours Established benefit and safety of interventions Potential for community control exists Added value to “community” based rather than individual based approach

25
Natural History of IGT IGT Normal 25% IGT 25% Diabetes 50% After 10 years

26
Prevention Studies in People with IGT: Downstream strategies Lifestyle interventions – Da Qing :Diet and Exercise – Malmo study : Diet and exercise – Finish Diabetes Prevention Study Lifestyle – DPP (Diabetes Prevention Study) Lifestyle, MF (Glitazone) Lifestyle interventions with pharmacological agents – FHS (Fasting Hyperglycaemia Study) Healthy Living and SU – EDIT (Early Diabetes Intervention Study): Acarbose and MF – STOP NIDDM : Acarbose
 Lifestyle, MF (Glitazone) Lifestyle interventions with pharmacological agents – FHS (Fasting Hyperglycaemia Study) Healthy Living and SU – EDIT (Early Diabetes Intervention Study): Acarbose and MF – STOP NIDDM : Acarbose")
27
DA QING - 1997, Diabetes Care, Pan et al Screened 110,660 Men and women in 33 health centres in China (all population > 25yrs) 577 IGT Diet / Exercise / Both / Control Mean Age 45 yrs Mean BMI 25.8 Kg/m2 6 yr FU, OGTT every 2 yrs
 577 IGT Diet / Exercise / Both / Control Mean Age 45 yrs Mean BMI 25.8 Kg/m2 6 yr FU, OGTT every 2 yrs")
28
Incidence of diabetes at or before 6-year evaluation Xiao-Ren et al, 1997

29
DA QING Results Reduction in risk of developing diabetes – Diet 31% – Exercise 46% – Both 42% Other results Lean group with exercise decreased risk with weight increase BMI overall- no change, but in BMI>25 it decreased by 1 Kg ? apply to European Population : older, more obese, socio-cultural issues, statistical issues Importance of physical activity apart from the weight control

30
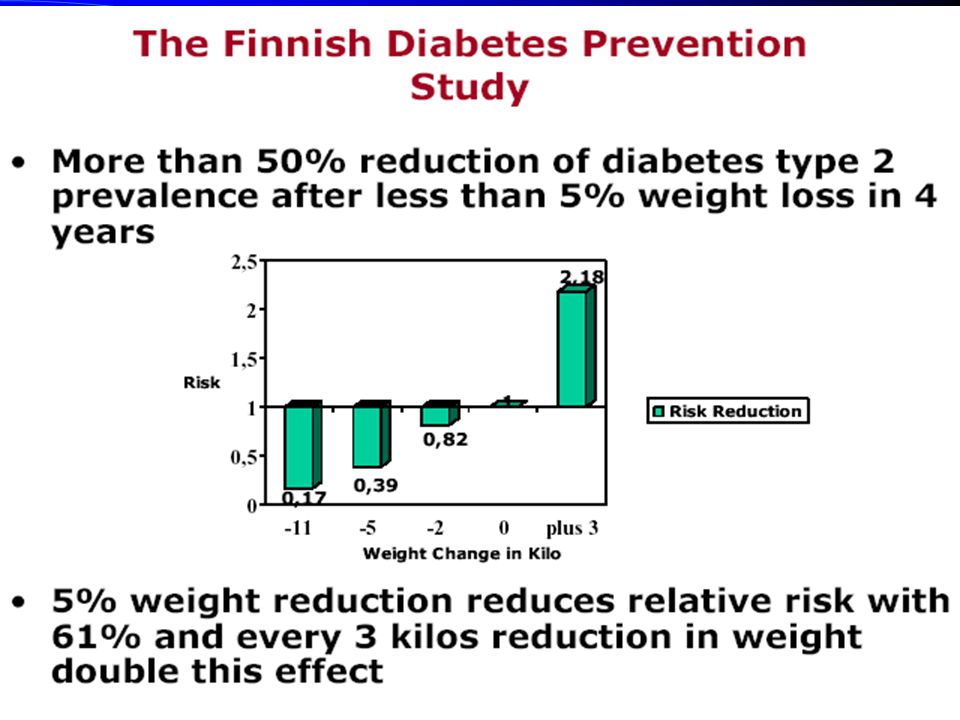
Finish Diabetes Prevention Study 522 - IGT BUT older and more obese – Aged 40-65 – Family History of diabetes / overweight – Age 55 yrs – BMI 31 Tuomilehto et al, NEJM, May 2001

31
Finish Diabetes Prevention Study Dietary and Exercise Intervention Goals – 5% weight loss – Total fat intake < 30% – Saturated fat intake <10% – Fibre >15gm per 1000 kcal – Moderate exercise for 30 mins every day Seven sessions in first year,1 session nutritionalist every 3 months throughout 4 year study

32
Success in achieving the goals of the intervention by one year according to treatment group Tuomilehto et al 2001

34
Finish Diabetes Prevention Study Risk of developing diabetes reduced by 58% after 4 years 11% vs 23% Cumulative risk of developing diabetes NNT = 8

35
Diabetes Prevention Programme (DPP) 27 centres 3234 participants > Or = 25 years BMI > or = 24 (22 for indo Asian) IGT 45% – American Indian, African American, Hispanic American, Asia American, pacific islanders
 27 centres 3234 participants > Or = 25 years BMI > or = 24 (22 for indo Asian) IGT 45% – American Indian, African American, Hispanic American, Asia American, pacific islanders")
36
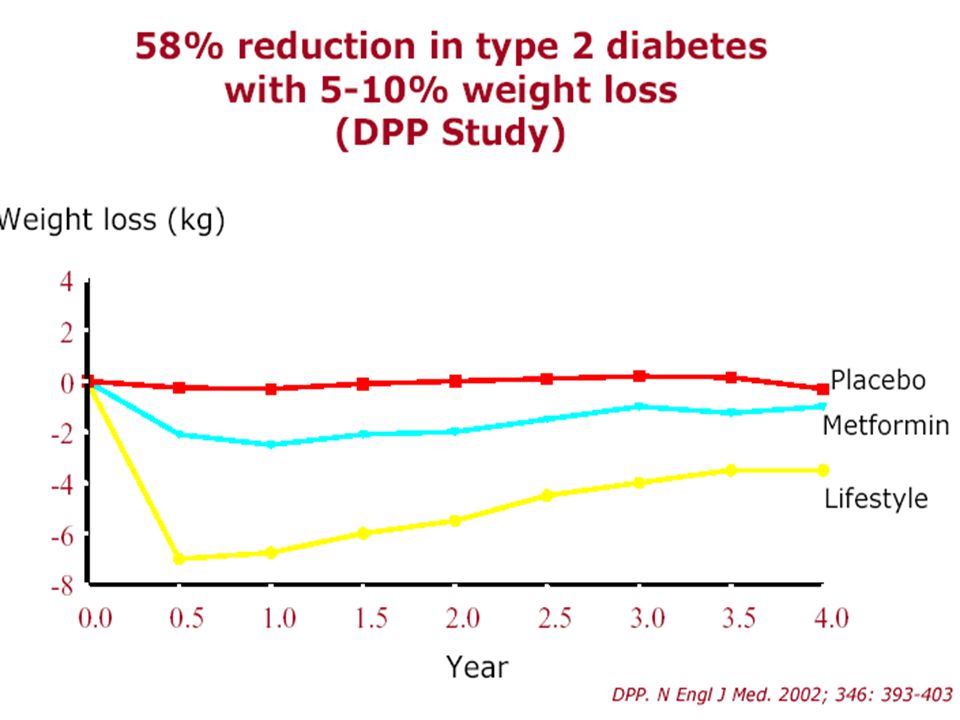
DPP Average Age 51 Years BMI 34 Lifestyle intervention Weight reduction 7% Low fat diet Exercise for 150 mins per week OR metformin 850mgs BD

37
DPP Trial stopped 1 year early, after 2.8 yr of follow-up 29% Diabetes in controls 14% in Diet and exercise 22% in Metformin 3 year DataRisk Reduction 58% whole group 71% those aged >60yrs 31% Metformin (less effect in older and less obese)
")
39
Cost of Prevention Total cost $174.3 million Diet and exercise prevented diabetes in 162 people Metformin prevented diabetes in 77 people (237 people did not develop diabetes over 3 yrs) NNT = 7 for life style intervention NNT= 14 for Metformin Costs per person over 3 yr excluding research cost Metformin $2542 Life style intervention $2780
 NNT = 7 for life style intervention NNT= 14 for Metformin Costs per person over 3 yr excluding research cost Metformin $2542 Life style intervention $2780")
40
Obesity and IGT Total 136 subjects with IGT and mean BMI of 48 27 controls 109 bariatric surgery Control group 22.2% developed diabetes Surgical group 0.91% developed diabetes 25-30 fold reduction in risk of diabetes Long et al Diabetes Care 1994

41
Obesity Swedish Obese Subjects (SOS) 845 controls 845 bariatric surgery 2 yr FU Mean Age 48 yrs BMI 40-42 Sjostrom et al Obesity Research 1999
 845 controls 845 bariatric surgery 2 yr FU Mean Age 48 yrs BMI Sjostrom et al Obesity Research 1999")
42
Weight Loss in SOS Sjostrom et al, 1999 months

43
XENDOS 3300 patients, BMI>30 Xenical or placebo for 4 years – With diet / exercise advice 2 weekly for 6/12, then monthly Xenical group lost 6.9kg, control 4.1kg Xenical group 37% less likely to develop DM NNT = 36

44
Other interventions Midstream intervention – Obese patients- pound for pound ( treatment group monthly newsletter and 4 session of couselling- 12 mths) – Children – Gestational diabetes Upstream intervention – Best – North Karelia study – Stanford five city project
 – Children – Gestational diabetes Upstream intervention – Best – North Karelia study – Stanford five city project")
45
Group Work Briefly discuss the following questions Your abstract/article: read the abstract,and if possible, share the evidence during discussion Provide the examples from your practice wherever possible.

46
Question 1 Given a perfect world, what ‘ideally’ should be done to reduce the twin burden of diabetes and obesity. What will be an ‘ideal’ programme in our setting ( think there are no constraints) 5 min
 5 min.")
47
Question 2 List possible constraints in implementation of the ideal programme in our setting e.g. Attitudes of people concerned- health care professionals and general population Any solutions to those constraints?

48
Customer Profiles - Driving Change Lifestyle Technology Economics Type 2 Yesterday Low motivation moderately mobile Average Age: 60 overweight not well informed low awareness Type 2 +10 years Average Age: 45 physically inactive obese Aware but indifferent better informed/ “connected” consumer power “quick-fix” remedies

49
Current Scenario Focus on treatment and prevention of complications – secondary prevention ( mainly individual based) Needs a ‘paradigm’ shift- from secondary prevention to primary prevention Three strategies for primary prevention- – Upstream- whole population – Midstream- special high risk groups eg children, elderly etc – Downstream- high risk ‘individuals’
 Needs a ‘paradigm’ shift- from secondary prevention to primary prevention Three strategies for primary prevention- – Upstream- whole population – Midstream- special high risk groups eg children, elderly etc – Downstream- high risk ‘individuals’")
50
Question-3 Pros and Cons of various primary prevention focus groups?

51
Primary prevention vs secondary prevention

52
Primary Prevention – why?

53
The way forward Structured programme geared towards prevention Commitment of more resources- Costs need to be considered as investment More Education to the users especially the socially deprived Implementation of the intensive programmes of management to curtail the costs.

Similar presentations