Download presentation
Presentation is loading. Please wait.

1
Multidisciplinary Cancer Breast Management Locally Advanced Primary Breast Cancer

2
Multidisciplinary Cancer Breast Management Natural History of Disease Most cases of stage III breast cancer were once stage I breast cancer In poor countries, more than half of patients have locally advanced or metastatic disease at the time of diagnosis – Lack of education – Lack of screening

3
Multidisciplinary Cancer Breast Management Clinical Presentation “Grave clinical signs” – Skin ulceration – Skin edema – Tumor fixation to the chest wall – Axillary nodes larger than 2.5 cm – Fixed axillary nodes Satellite skin nodules and infraclavicular, internal mammary, and supraclavicular adenopathy

4
Multidisciplinary Cancer Breast Management Clinical Presentation of Stage III Breast Cancer Peau d’orangeLarge mass, edema, and erythema

5
Multidisciplinary Cancer Breast Management Clinical Presentation of Stage III, Locally Advanced (Inoperable) Disease Large primary breast cancerLocally advanced breast cancer
 Disease Large primary breast cancerLocally advanced breast cancer")
6
Multidisciplinary Cancer Breast Management Diagnostic Work-Up Distinguish benign from malignant disease Distinguish noninvasive from invasive disease Obtain pathologic diagnosis before treatment: – Percutaneous image-guided biopsy (preferred) -Core-needle biopsy -Fine-needle aspiration – Excisional biopsy
 -Core-needle biopsy -Fine-needle aspiration – Excisional biopsy")
7
Breast Cancer Up Until Now: Testing for 1 or 2 Specific Molecules Estrogen Receptor: 75% of breast cancers are ER+ HER-2: 20-25% of breast cancers are HER-2+ Multidisciplinary Cancer Breast Management

8
TNM Staging System for Advanced Breast Cancer T3 Tumor >5 cm T4 Invasion of the chest wall or to the skin (inflammatory breast cancer) T4aInvasion of the chest wall T4bEdema, thickening of the skin, or ulceration of the skin or surrounding skin nodules T4cSigns of both T4a and T4b T4dInflammatory cancer (breast is red, swollen, and warm) Greene FL, et al. AJCC Cancer Staging Manual, 6th ed, 2002.

9
Multidisciplinary Cancer Breast Management TNM Staging System for Advanced Breast Cancer (cont.) N2 Involvement of four to nine axillary lymph nodes or of internal mammary lymph nodes without axillary node involvement. N2a Involvement of four to nine axillary lymph nodes N2b Involvement of only internal mammary lymph nodes

10
Multidisciplinary Cancer Breast Management TNM Staging System for Advanced Breast Cancer (cont.) N3Involvement of 10 or more axillary lymph nodes or of the infraclavicular lymph nodes or of the internal mammary nodes with axillary node involvement N3aInvolvement of 10 or more axillary lymph nodes or of the infraclavicular lymph nodes N3bInvolvement of the internal mammary nodes and axillary nodes N3cInvolvement of the supraclavicular nodes
 N3Involvement of 10 or more axillary lymph nodes or of the infraclavicular lymph nodes or of the internal mammary nodes with axillary node involvement N3aInvolvement of 10 or more axillary lymph nodes or of the infraclavicular lymph nodes N3bInvolvement of the internal mammary nodes and axillary nodes N3cInvolvement of the supraclavicular nodes")
11
Multidisciplinary Cancer Breast Management Stage Classifications for Locally Advanced Breast Cancer StageIIBT2N1M0 T3N0M0 StageIIIAT0N2M0 T1N2M0 T2N2M0 T3N1M0 T3N2M0

12
Multidisciplinary Cancer Breast Management Stage Classifications for Locally Advanced Breast Cancer (cont.) StageIIIBT4N0M0 T4N1M0 T4N2M0 StageIIICAnyTN3M0 StageIVAnyT NM1
 StageIIIBT4N0M0 T4N1M0 T4N2M0 StageIIICAnyTN3M0 StageIVAnyT NM1")
13
Multidisciplinary Cancer Breast Management Survival According to Treatment Treatment No. of Patients 5-Yr. Survival (%) Surgery only2,45336 Radiation only2,38629 Surgery plus radiation4,24933 Chemotherapy, surgery, and radiation 1,92363 Giordiano SH. Oncologist. 2003;8:521-530.
 Surgery only2,45336 Radiation only2,38629 Surgery plus radiation4,24933 Chemotherapy, surgery, and radiation 1,92363 Giordiano SH. Oncologist. 2003;8:")
14
Personalizing Treatment to the Specific Tumor Multidisciplinary Cancer Breast Management

15
Systemic Therapy for Breast Cancer Goals: – Attain cure, prevent recurrence, eradicate micrometastases Appropriate treatments: – Tamoxifen or aromatase inhibitors for postmenopausal women – Ovarian ablation – Chemotherapy – Monoclonal antibody therapy – Supportive care

16
Multidisciplinary Cancer Breast Management Chemotherapy for Breast Cancer Improves disease-free and overall survival Durations of more than six months do not add major advantage Anthracycline-based combinations are better than combination of cyclophosphamide, methotrexate, and fluorauracil (CMF) Taxane-based combinations are more effective in the adjuvant setting Trastuzumab in the adjuvant setting improves disease-free and overall survival
 Taxane-based combinations are more effective in the adjuvant setting Trastuzumab in the adjuvant setting improves disease-free and overall survival")
17
Multidisciplinary Cancer Breast Management Neoadjuvant Chemotherapy Concept developed concurrently with adjuvant chemotherapy in the 1970s Treatment for locally advanced breast cancer (stage III disease) Allows for immediate assessment of tumor response Allows for the evaluation of new and novel agents
 Allows for immediate assessment of tumor response Allows for the evaluation of new and novel agents")
18
Multidisciplinary Cancer Breast Management Neoadjuvant Chemotherapy (cont.) Goals: – Decrease tumor size – Minimize surgery – Establish tumor sensitivity Appropriate treatments: – Chemotherapy – Tamoxifen or aromatase inhibitors – Radiation therapy
 Goals: – Decrease tumor size – Minimize surgery – Establish tumor sensitivity Appropriate treatments: – Chemotherapy – Tamoxifen or aromatase inhibitors – Radiation therapy")
19
Multidisciplinary Cancer Breast Management Clinical Rationale for Preoperative Chemotherapy: Excellent response rates for locally advanced breast cancer Efficacy of adjuvant chemotherapy for node- negative breast cancer Equivalent survival for breast-conserving surgery and mastectomy

20
Multidisciplinary Cancer Breast Management Advantages of Neoadjuvant Chemotherapy Increased rate of breast-conserving surgery Earlier treatment of micrometastases Treatment serves as in vivo chemosensitivity assay Improved rates of local control and disease-free survival

21
Multidisciplinary Cancer Breast Management Factors Influencing Decision to Use Neoadjuvant Chemotherapy in Operable Breast Cancer Does the patient need adjuvant chemotherapy based on information known prior to surgery? Would neoadjuvant chemotherapy potentially alter the extent of resection? Does the patient desire breast preservation? Would treatment benefit from knowledge of in vivo chemosensitivity?

23
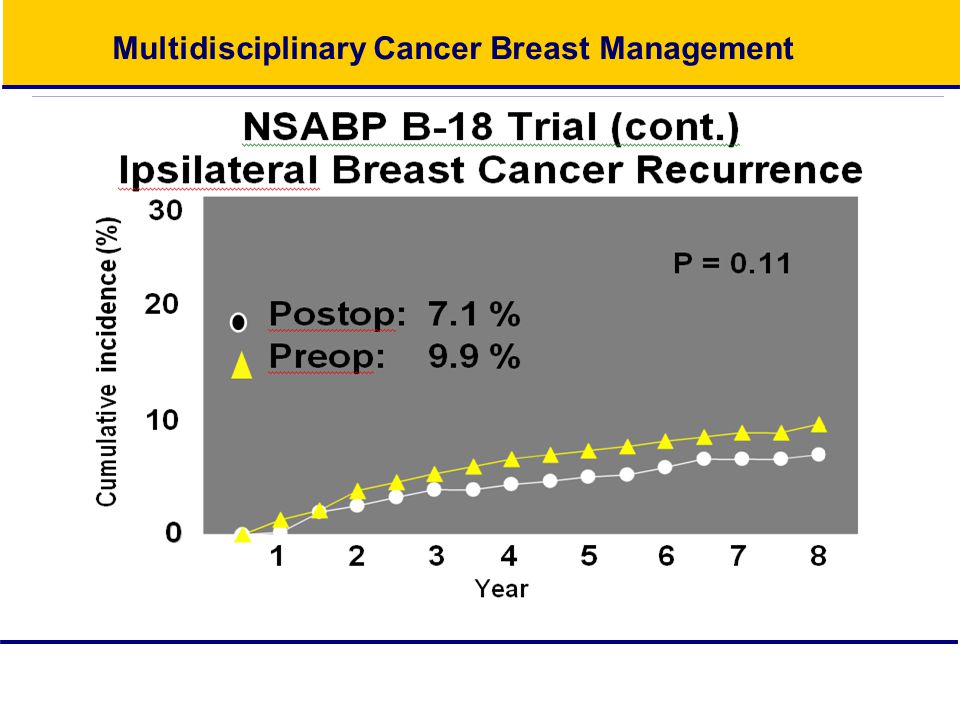
Multidisciplinary Cancer Breast Management NSABP B-18 Trial: Schema OperableBreastCancer Operable Breast Cancer Stratification Age Clinical tumor size Clinical node status Operation AC x 4 +TAMif>50yrs. + TAM if >50 yrs. AC x 4 +TAMif>50yrs. + TAM if >50 yrs. Operation

24
Multidisciplinary Cancer Breast Management

25
58% 40 % P < 0.01 % positive nodes 80 40 20 0 Postop. Chemotherapy Preop. chemotherapy

26
Multidisciplinary Cancer Breast Management

30
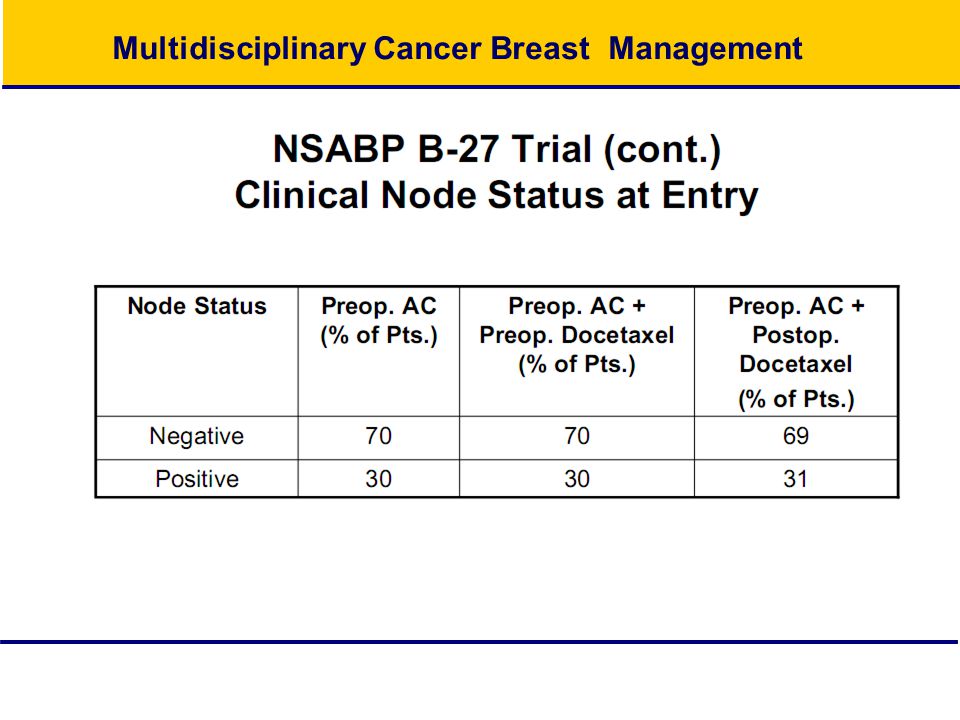
NSABP B-27 Trial Eligibility: Operable Breast Cancer Diagnosis by fine-needle aspiration or core biopsy Palpable on physical examination (T1c-3 N 0, M 0 / T 1-3, N 1, M 0) Movable in relation to chest wall and skin Nodes of any size but not fixed to each other or to adjacent structures No arm edema
 Movable in relation to chest wall and skin Nodes of any size but not fixed to each other or to adjacent structures No arm edema")
31
Multidisciplinary Cancer Breast Management

34
NSABP B-27 Trial (cont.) Grade of Tumor at Entry Tumor Grade Preop. AC (n = 2,400) Preop. or Postop. Docetaxel (n = 1,494) 12215 25040 31316 41024
 Preop. or Postop. Docetaxel (n = 1,494)")
35
Multidisciplinary Cancer Breast Management NSABP B-27 Trial (cont.) Treatment Regimen Chemotherapy:doxorubicin, 60 mg/m 2 cyclophosphamide, 600 mg/m 2 Docetaxel:100 mg/m 2 Tamoxifen:20 mg, orally, daily for five years (beginning on day 1 of chemotherapy) Radiation:Only for patients who had lumpectomy; done after surgery (arms I and II) and after treatment with docetaxel) (arm III)
 Treatment Regimen Chemotherapy:doxorubicin, 60 mg/m 2 cyclophosphamide, 600 mg/m 2 Docetaxel:100 mg/m 2 Tamoxifen:20 mg, orally, daily for five years (beginning on day 1 of chemotherapy) Radiation:Only for patients who had lumpectomy; done after surgery (arms I and II) and after treatment with docetaxel) (arm III)")
36
Multidisciplinary Cancer Breast Management NSABP B-27 Trial (cont.) Effect of Preoperative Docetaxel Compared with chemotherapy and surgery alone, chemotherapy and docetaxel followed by surgery led to increased rates of – Clinical response – Pathologic response – Downstaging of node disease – Lumpectomies
 Effect of Preoperative Docetaxel Compared with chemotherapy and surgery alone, chemotherapy and docetaxel followed by surgery led to increased rates of – Clinical response – Pathologic response – Downstaging of node disease – Lumpectomies")
37
Multidisciplinary Cancer Breast Management

40
cOR Multidisciplinary Cancer Breast Management

41
NSABP B-27 Trial (cont.) Effect of Postoperative Docetaxel Compared with chemotherapy and surgery alone, chemotherapy and surgery followed by docetaxel led to increased rates of disease-free and overall survival in subgroups of patients (according to nodes)
 Effect of Postoperative Docetaxel Compared with chemotherapy and surgery alone, chemotherapy and surgery followed by docetaxel led to increased rates of disease-free and overall survival in subgroups of patients (according to nodes)")
42
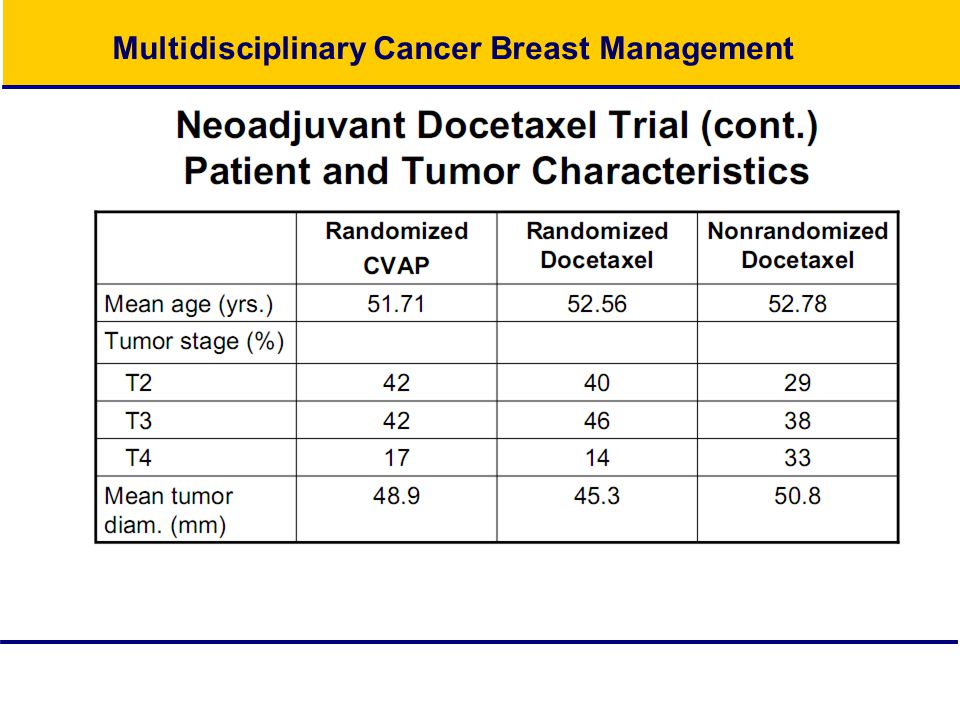
Multidisciplinary Cancer Breast Management Neoadjuvant Docetaxel Trial by Aberdeen Breast Group Randomized trial Single-agent docetaxel compared with anthracycline-based polychemotherapy regimen 145 patients Large (>3cm) or locally advanced (T3, T4, Tx N2) breast cancer No prior therapy
 or locally advanced (T3, T4, Tx N2) breast cancer No prior therapy")
43
Multidisciplinary Cancer Breast Management

45
Neoadjuvant Docetaxel Trial (cont.) Response Rates: First Phase Objective Clinical Response % of Pts. (N =145) Overall67 Complete16 Partial51 Stable disease32 Progressive disease1
 Overall67 Complete16 Partial51 Stable disease32 Progressive disease1.")
46
Multidisciplinary Cancer Breast Management Neoadjuvant Docetaxel Trial (cont.) Response Rates: Second Phase (Patients with Response) Objective Clinical Response CVP (N = 50) Docetaxel (N = 47) Overall6694* Complete3462 Partial (additional)32 Partial (maintained)306 Progressive disease40 *p = 0.001
 Response Rates: Second Phase (Patients with Response) Objective Clinical Response CVP (N = 50) Docetaxel (N = 47) Overall6694* Complete3462 Partial (additional)32 Partial (maintained)306 Progressive disease40 *p = 0.001")
47
Multidisciplinary Cancer Breast Management Neoadjuvant Docetaxel Trial (cont.) Response Rates: Second Phase (Patients without Response) Objective Clinical Response % of Pts. (N = 48) Overall55 Complete13 Partial42 Stable disease35 Progressive disease10
 Overall55 Complete13 Partial42 Stable disease35 Progressive disease10.")
48
Multidisciplinary Cancer Breast Management

50
Prospective Evaluation of Paclitaxel Versus Combination Chemotherapy With Fluorouracil, Doxorubicin, and Cyclophosphamide as Neoadjuvant Therapy in Patients With Operable Breast Cancer By Aman U. Buzdar, S. Eva Singletary, Richard L. Theriault, Daniel J. Booser, Vicente Valero, Nuhad Ibrahim, Terry L. Smith, Lina Asmar, Debra Frye, Nikki Manuel, Shu-Wan Kau, Marsha McNeese, Eric Strom, Kelly Hunt, Frederick Ames, and Gabriel N. Hortobagyi J Clin Oncol 17:3412-3417.

51
Weekly (wkly) paclitaxel (P) followed by FAC as primary systemic chemotherapy (PSC) of operable breast cancer improves pathologic complete remission (pCR) rates when compared to every 3-week (Q 3 wk) P therapy (tx) followed by FAC- final results of a prospective phase III randomized trial. Marjorie C Green, Aman U Buzdar, Terry Smith, Nuhad K Ibrahim, Vicente Valero, Marguerite Rosales, Massimo Cristofanilli, Daniel J Booser, Lajos Pusztai, Edgardo Rivera, Richard Theriault, Cynthia Carter, Sonja E Singletary, Henry M Kuerer, Kelly Hunt, Eric Strom, Gabriel N Hortobagyi Proc Am Soc Clin Oncol 21: 2002 (abstr 135) Pathologic Complete Remission Rates (Breast and Lymph Nodes) : Weekly vs. Q 3 Week Paclitaxel Node Positive Node Negative Weekly (n = 50)Q 3 Week (n= 51)Weekly (n = 68)Q 3 Week (n = 67) pCR 14 (28%)7 (13.7%)20 (29.4%)9 (13.4%) Weekly Paclitaxel is superior to q 3 weeks.
 Pathologic Complete Remission Rates (Breast and Lymph Nodes) : Weekly vs. Q 3 Week Paclitaxel Node Positive Node Negative Weekly (n = 50)Q 3 Week (n= 51)Weekly (n = 68)Q 3 Week (n = 67) pCR 14 (28%)7 (13.7%)20 (29.4%)9 (13.4%) Weekly Paclitaxel is superior to q 3 weeks..")
52
Biological Therapy: Targeting Factors That Allow a Cancer Cell to Develop, Survive and Spread

53
The HER Family of Receptors HER1 EGFR HER2 HER3 HER4 Tumor Cell Trastuzumab (Herceptin)Trastuzumab (Herceptin) Pertuzumab (Omnitarg)Pertuzumab (Omnitarg) LapatinibLapatinib Erlotinib (Tarceva)Erlotinib (Tarceva) Gefitinib (Iressa)Gefitinib (Iressa) Cetuximab (Erbitux)Cetuximab (Erbitux)
Trastuzumab (Herceptin) Pertuzumab (Omnitarg)Pertuzumab (Omnitarg) LapatinibLapatinib Erlotinib (Tarceva)Erlotinib (Tarceva) Gefitinib (Iressa)Gefitinib (Iressa) Cetuximab (Erbitux)Cetuximab (Erbitux)")
54
Drugs Targeting HER-2 in Breast Cancer HER-2 nucleus cancer cell cell division Trastuzumab (Herceptin) Anti-HER-2 Antibody (IV) HER-2 Oncogene: overexpressed in 20-25% of breast cancers Lapatinib (Tykerb) Dual HER-1/HER-2 (oral) Tyrosine Kinase Inhibitor
 Anti-HER-2 Antibody (IV) HER-2 Oncogene: overexpressed in 20-25% of breast cancers Lapatinib (Tykerb) Dual HER-1/HER-2 (oral) Tyrosine Kinase Inhibitor")
55
Multidisciplinary Cancer Breast Management Update on Studies with Trastuzumab Survival advantage with chemotherapy and trastuzumab in the metastatic setting Trastuzumab in adjuvant setting produced spectacular results with 50% decrease in recurrence Alternative approach is to introduce trastuzumab in the neoadjuvant setting, where response to therapy can provide an intermediate endpoint for the impact of trastuzumab on survival in early breast cancer

56
Recommendations From an International Expert Panel on the Use of Neoadjuvant (Primary) Systemic Treatment of Operable Breast Cancer: An Update Manfred Kaufmann, Gabriel N. Hortobagyi, Aron Goldhirsch, Suzy Scholl, Andreas Makris, Pinuccia Valagussa, Jens-Uwe Blohmer, Wolfgang Eiermann, Raimund Jackesz, Walter Jonat, Annette Lebeau, Sibylle Loibl, William Miller, Sigfried Seeber, Vladimir Semiglazov, Roy Smith, Rainer Souchon, Vered Stearns, Michael Untch, and Gunter von Minckwitz J Clin Oncol 24:1940-1949

57
Multidisciplinary Cancer Breast Management

60
Trials of Neoadjuvant Trastuzumab: Summary of Efficacy Preoperative clinical responses observed – Overall response rate, 70% to 90% – Clinical complete response, 15% to 30% – Pathologic complete response, approximately 18% Responses higher for patients with 3+ expression of HER2

61
Endocrine Therapy

62
Drugs Targeting Estrogen and It’s Receptor in Breast Cancer Estrogen Cell Growth and Division Estrogen Receptor SERMS (tamoxifen, raloxifene), SERDS (fulvstrant) Aromatase inhibitors, ovarian suppression
, SERDS (fulvstrant) Aromatase inhibitors, ovarian suppression")
63
Aromatase Inhibitors Adrenal Hormones CortisolAndrostenedioneAldosterone Estradiol TestosteroneEstrone Aromatase inhibitors block post-menopausal estrogen production Anastrozole (Arimidex) Letrozole (Femara) Exemestane (Aromasin)
 Letrozole (Femara) Exemestane (Aromasin)")
64
The relative efficacy of neoadjuvant endocrine therapy versus chemotherapy in postmenopausal women with ER positive breast cancer V. F. Semiglazov, V. Semiglazov, V. Ivanov, A. Bozhok, E. Ziltsova, R. Paltuev, G. Dashian, A. Kletzel, E. Topuzov and L. Berstein Journal of Clinical Oncology, Vol 22, No 14S 2004: 519 Methods: 121 postmenopausal women with ER(+) and/or PgR(+) breast cancer T2N1–2, T3N0–1, T4N0M0 assigned to NAT with either CT Dox 60 mg/m2 + Pac 200 mg/m2, every 3 weeks, 4 cycles, n=62 patients (pts), or HT with aromatase inhibitors, anastrazole 1 mg, n = 30 pts, 3 months). In CT arm the most frequent grade III/IV toxicity was alopecia ( 79.3 % ), neutropenia ( 43.1 %), cardiotoxicity (6.8 %), diarrhea (1.7%). HT was well tolerated. The most commonly adverse events were hot flushes (23.3%), vaginal discharge (6.6%), musculosskeletal disorders (1.7%). Note this does not give the pathologic CR rate.
 and/or PgR(+) breast cancer T2N1–2, T3N0–1, T4N0M0 assigned to NAT with either CT Dox 60 mg/m2 + Pac 200 mg/m2, every 3 weeks, 4 cycles, n=62 patients (pts), or HT with aromatase inhibitors, anastrazole 1 mg, n = 30 pts, 3 months). In CT arm the most frequent grade III/IV toxicity was alopecia ( 79.3 % ), neutropenia ( 43.1 %), cardiotoxicity (6.8 %), diarrhea (1.7%). HT was well tolerated. The most commonly adverse events were hot flushes (23.3%), vaginal discharge (6.6%), musculosskeletal disorders (1.7%). Note this does not give the pathologic CR rate..")
65
Primary Systemic Therapy of Breast Cancer Irina Sachelarie, Michael L. Grossbard, Manjeet Chadha, Sheldon Feldman, Munir Ghesani and Ronald H. Blum Oncologist 2006;11;574-589

66
Recommendations From an International Expert Panel on the Use of Neoadjuvant (Primary) Systemic Treatment of Operable Breast Cancer: An Update Manfred Kaufmann, Gabriel N. Hortobagyi, Aron Goldhirsch, Suzy Scholl, Andreas Makris, Pinuccia Valagussa, Jens-Uwe Blohmer, Wolfgang Eiermann, Raimund Jackesz, Walter Jonat, Annette Lebeau, Sibylle Loibl, William Miller, Sigfried Seeber, Vladimir Semiglazov, Roy Smith, Rainer Souchon, Vered Stearns, Michael Untch, and Gunter von Minckwitz J Clin Oncol 24:1940-1949

67
Multidisciplinary Cancer Breast Management

71
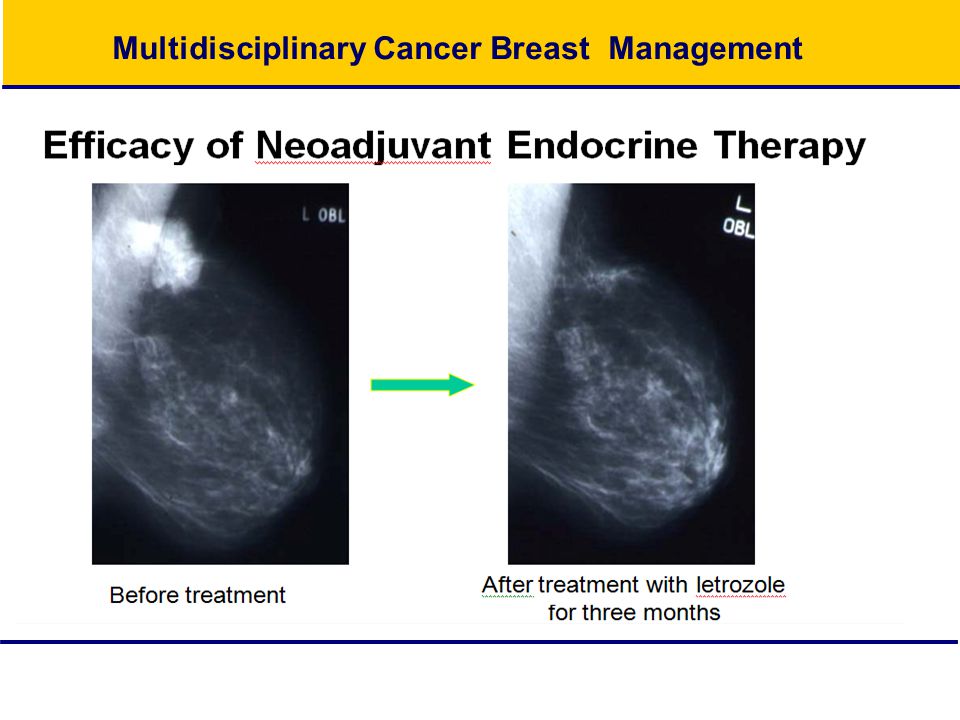
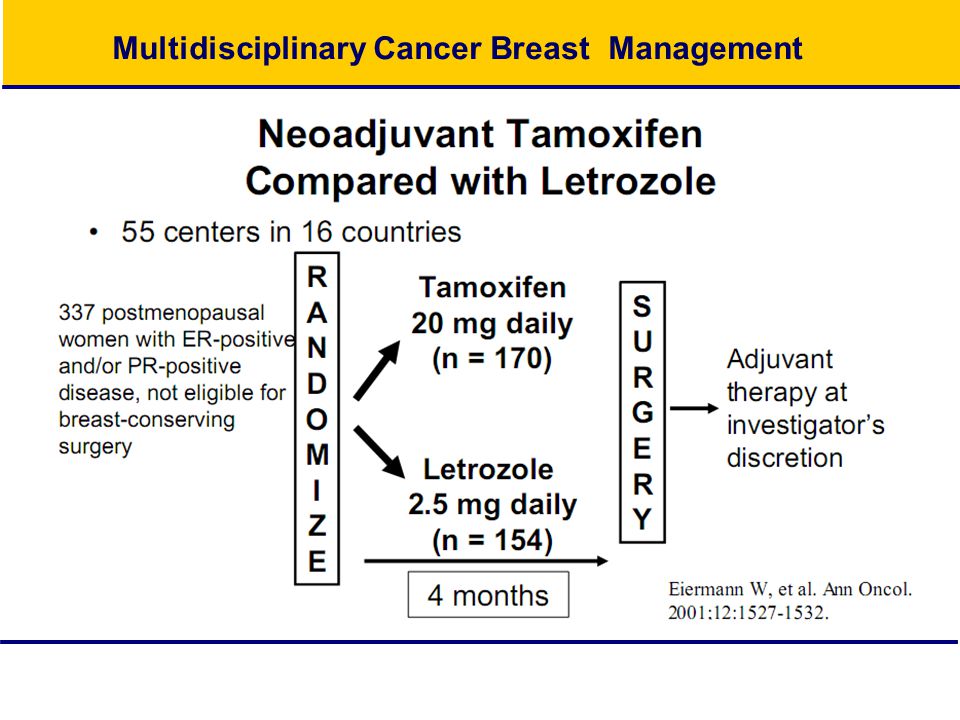
Letrozole Is More Effective Neoadjuvant Endocrine Therapy Than Tamoxifen for ErbB-1– and/or ErbB-2–Positive, Estrogen Receptor–Positive Primary Breast Cancer: Evidence From a Phase III Randomized Trial By Matthew J. Ellis, Andrew Coop, Baljit Singh, Louis Mauriac, Antonio Llombert-Cussac, Fritz Ja¨nicke, William R. Miller, Dean B. Evans, Margaret Dugan, Carolyn Brady, Erhard Quebe-Fehling, and Mieke Borgs J Clin Oncol 19:3808-3816.

72
Multidisciplinary Cancer Breast Management Preoperative Endocrine Therapy: Tamoxifen Compared with Aromatase Inhibitors Study P024IMPACTSemiglazovPROACT Drug(s) LETTAMANATAM ANA+ TAM EXETAMANATAM Duration16 wks.12 wks.16 wks.12 wks. No. of pts. 1541701131081093637163151 Response rate (%) 553637363989575040 BCS (%) 453546222639114738
 BCS (%)")
73
Recommendations From an International Expert Panel on the Use of Neoadjuvant (Primary) Systemic Treatment of Operable Breast Cancer: An Update Manfred Kaufmann, Gabriel N. Hortobagyi, Aron Goldhirsch, Suzy Scholl, Andreas Makris, Pinuccia Valagussa, Jens-Uwe Blohmer, Wolfgang Eiermann, Raimund Jackesz, Walter Jonat, Annette Lebeau, Sibylle Loibl, William Miller, Sigfried Seeber, Vladimir Semiglazov, Roy Smith, Rainer Souchon, Vered Stearns, Michael Untch, and Gunter von Minckwitz J Clin Oncol 24:1940-1949

74
Multidisciplinary Cancer Breast Management Radiation Therapy after Mastectomy According to Consensus Statement developed by American Society for Therapeutic Radiology and Oncology (ASTRO) Radiation therapy should be part of the treatment for stage III breast cancers and for disease that involves four or more lymph nodes At a minimum, the chest wall and the supraclavicular fossa should be treated with doses of at least 50 Gy
 Radiation therapy should be part of the treatment for stage III breast cancers and for disease that involves four or more lymph nodes At a minimum, the chest wall and the supraclavicular fossa should be treated with doses of at least 50 Gy")
75
Conclusions Neoadjuvant therapy: Increases the likelihood of breast conservation somewhat. Does not adversely affect survival excepting a small risk of locoregional failure. More is likely better – i.e. add the taxane Endocrine receptor status will affect the outcome and may need to be treated upfront, but chemo has more robust data. Randomized comparison of endocrine vs chemo vs both is currently lacking for the ER/PR + pt.

76
Does a cCR need surgery? Is Surgery Necessary After Complete Clinical Remission Following Neoadjuvant Chemotherapy for Early Breast Cancer? By A. Ring, A. Webb, S. Ashley, W.H. Allum, S. Ebbs, G. Gui, N.P. Sacks, G. Walsh, and I.E. Smith J Clin Oncol 21:4540-4545

Similar presentations














 Phase III trial comparing AC (x4)taxane (x4) with taxane (x8) as adjuvant therapy for node-positive breast cancer: Results of N-SAS-BC02.>")


 on the Efficacy.>")



 in combination with chemotherapy: pivotal metastatic breast cancer survival data 1.>")







