Download presentation
Presentation is loading. Please wait.

3
INTRODUCTION

4
Pervasive developmental disorders (PDDs) are complex neurodevelopmental disorders characterized by core deficits in three major domains Social interaction and social relatedness Verbal and nonverbal communication Restricted interests and/or repetitive or stereotyped behaviors
 are complex neurodevelopmental disorders characterized by core deficits in three major domains Social interaction and social relatedness Verbal and nonverbal communication Restricted interests and/or repetitive or stereotyped behaviors")
5
Classification of PDDS Autism Asperger’s syndrome Childhood disintegrative disorder Pervasive developmental disorder not otherwise specified Rett’s syndrome

6
Autism It is characterized by qualitative behavioral abnormalities in the domains of communication, reciprocal social interaction and interests, and activities that are repetitive, restricted and stereotyped, that appear before 3 years of age

7
Asperger’s Syndrome It shares the social-relatedness impairment and the presence of restricted interest and/or repetitive behavior, but requires that the child have no delay in language development.

8
Childhood disintegrative disorder It is a clinical syndrome characterized by disintegration of mental functions and regression of acquired language and intellectual functions after a period of normal development up to 3-4 years in children

9
Pervasive developmental disorder not otherwise specified The diagnosis of PDD-NOS is made in individuals with some, but not all features of autistic disorder (either quantitatively or qualitatively). Social deficits are always present, along with some degree of impaired communication or restricted interests/repetitive behaviors.

10
Rett’s syndrome It is a rare disorder occurring almost exclusively in females. There is an initial period of normal development followed by regression in social and language skills that can be confused with autism.

11
Etiology of PDDs: Genetic causesParental causesPerinatal and obstetric factorsMetallic elementsImmunological disordersCognitive theoriesMetabolic disordersInfectionsGastrointestinal factors

12
Core symptoms Deficits in reciprocal social interaction Deficits in communication Deficits in interests and activities Associated features RegressionImpaired attentionMotor impairmentsSavant syndromeVisual disordersSensory impairments Inflammatory disorders Epilepsy Symptoms of PDDs

13
AIM OF THE WORK

14
This study is designed to formulate and apply Autism Diagnostic Interview (Lord et al, 1994) as a tool for evaluating Egyptian children with pervasive developmental disorders in order to detect its accuracy in quantifying the autistic features among different subtypes of these disorders.
 as a tool for evaluating Egyptian children with pervasive developmental disorders in order to detect its accuracy in quantifying the autistic features among different subtypes of these disorders.")
15
SUBJECTS

16
The study was applied on 80 children with age ranging from 2 to 6 years. They were divided into 3 groups: ◦ Group I: (PDD): 35 children referred with a diagnostic query regarding possible PDDs, with exclusion of children suffering from sensory deprivation and brain damage. ◦ Group II: (normal children): 25 children. ◦ Group III: (mentally retarded): 20 children with exclusion of children suffering from sensory deprivation and brain damage.
: 35 children referred with a diagnostic query regarding possible PDDs, with exclusion of children suffering from sensory deprivation and brain damage. ◦ Group II: (normal children): 25 children. ◦ Group III: (mentally retarded): 20 children with exclusion of children suffering from sensory deprivation and brain damage..")
17
METHODS

18
Each child was subjected to the protocol of evaluation for delayed language development which consists of three levels of evaluation Elementary diagnostic proceduresClinical diagnostic aids Interview protocol and administration

19
Parent's interview: It includes complaint and analysis of symptoms, personal history, search of etiological factors, child’s developmental history, family history, and child’s medical history. Examination: Measurement of growth parameters, examination of skin,muscle tone and reflexes. Elementary diagnostic procedures Clinical diagnostic aidsInterview protocol and administration

20
Elementary diagnostic procedures Evaluation of the various aptitudes by formal testing Audiological evaluation Language evaluation Clinical diagnostic aids Interview protocol and administration

21
Elementary diagnostic procedures Evaluation of the various aptitudes by formal testing Stanford Binet Intelligence scale: to assess cognitive age ( mental age ),verbal and abstract I.Q Vineland social maturity scale: to obtain social age and social quotient Childhood autism Rating Scale (CARS) Gilliam autism Rating Scale (GARS) Childhood attention adjustment survey ( CAAS ) : is a brief survey for identifying behavior problems Audiological evaluation Language evaluation Clinical diagnostic aids Interview protocol and administration Methods
,verbal and abstract I.Q Vineland social maturity scale: to obtain social age and social quotient Childhood autism Rating Scale (CARS) Gilliam autism Rating Scale (GARS) Childhood attention adjustment survey ( CAAS ) : is a brief survey for identifying behavior problems Audiological evaluation Language evaluation Clinical diagnostic aids Interview protocol and administration Methods")
22
Elementary diagnostic procedures Evaluation of the various aptitudes by formal testing Audiological evaluation Language evaluation Clinical diagnostic aids Interview protocol and administration Methods

23
Elementary diagnostic procedures Evaluation of the various aptitudes by formal testing Audiological evaluation Language evaluation Arabic language test : formal assessment of language components and detection of language age and language abilities. TACS (test of acquired communication skills ), to evaluate the prelinguistic skills Clinical diagnostic aids Interview protocol and administration Methods
, to evaluate the prelinguistic skills Clinical diagnostic aids Interview protocol and administration Methods.")
24
Elementary diagnostic procedures Clinical diagnostic aids Autism diagnostic interview (ADI-R) was translated and formulated to suit Egyptian culture and children. ADI-R Interview Protocol was with the informant (a parent or caregiver with the child being assessed). The assessed individual is not present during the interview. The interview typically takes l h to 2 hours to administer and score Interview protocol and administration
. The assessed individual is not present during the interview. The interview typically takes l h to 2 hours to administer and score Interview protocol and administration.")
25
The interview consists of eight main sections: Interview protocol and administration 1) The background questions about the subject’s family and education as well as on the diagnosis that have been applied and the medication that has been used. 2) This is followed by introductory questions, which are designed to provide a general picture of the subject’s behavior. This is necessary in order to provide an adequate framework for the further detailed questioning that follows. This includes item 1(current concerns about the child) Elementary diagnostic procedures Clinical diagnostic aids 3) The third section provides an account of early developmental milestones (item 2 through 8) 4) This is followed by questioning on the age at which key language skills were acquired and on the question as to whether there has been any period involving a loss of language skills after they have been acquired, or a general loss of other skills (item 9 through 28). 5) Language and communication functioning (items 29 to 49). 6) Social development and play (items 50 to 66).7) Interests and behaviors (items 67 to 79).8) The last section (items 80 to 93) deals with a range of general behaviors that are of clinical importance – such as aggression, self injury, the occurrence of possible epileptic features.
 This is followed by introductory questions, which are designed to provide a general picture of the subject’s behavior. This is necessary in order to provide an adequate framework for the further detailed questioning that follows. This includes item 1(current concerns about the child) Elementary diagnostic procedures Clinical diagnostic aids 3) The third section provides an account of early developmental milestones (item 2 through 8) 4) This is followed by questioning on the age at which key language skills were acquired and on the question as to whether there has been any period involving a loss of language skills after they have been acquired, or a general loss of other skills (item 9 through 28). 5) Language and communication functioning (items 29 to 49). 6) Social development and play (items 50 to 66).7) Interests and behaviors (items 67 to 79).8) The last section (items 80 to 93) deals with a range of general behaviors that are of clinical importance – such as aggression, self injury, the occurrence of possible epileptic features..")
26
The data was analyzed using statistical software package (SPSS version 16). The following statistical tests were used: Correlation Coefficient(r) Student t- test One way ANOVA Coefficient of reliability( Cronbach’s alpha ) Statistical Analysis
 Student t- test One way ANOVA Coefficient of reliability( Cronbach’s alpha ) Statistical Analysis.")
27
The test reliability was done by correlation between: Each domain to the total ADI-R score. Each domain with the other 2 domains. Each sub domain to its domain. Reliability

28
Face validity (5 phoniatricians judged the test) Construct validity was assessed by administering the test to 35 cases of PDD and 25 normal children Criterion-Related Validity: to check the performance of the test against some criterion Convergent Validity Divergent validity Concurrent validity Validity
 Construct validity was assessed by administering the test to 35 cases of PDD and 25 normal children Criterion-Related Validity: to check the performance of the test against some criterion Convergent Validity Divergent validity Concurrent validity Validity")
29
RESULTS

30
Mean age in months for the 3 groups.

31
Sex distribution in the 3 groups.

32
Comparison between means of the 3 groups as regards Stanford Binet Intelligence

33
Comparison between means of the 3 groups as regards CARS, GARS, VSMS

34
Correlation studies Correlation of ADI-R score with CARS Correlation of ADI-R score with CARS as regards mental age

35
Correlation studies Correlation of ADI-R scores with GARS

36
Correlation studies Correlation of ADI-R with TACS

37
Comparing means in between groups in domain A

38
Comparing means in between groups in domain B

39
Comparing means in between groups in domain C

40
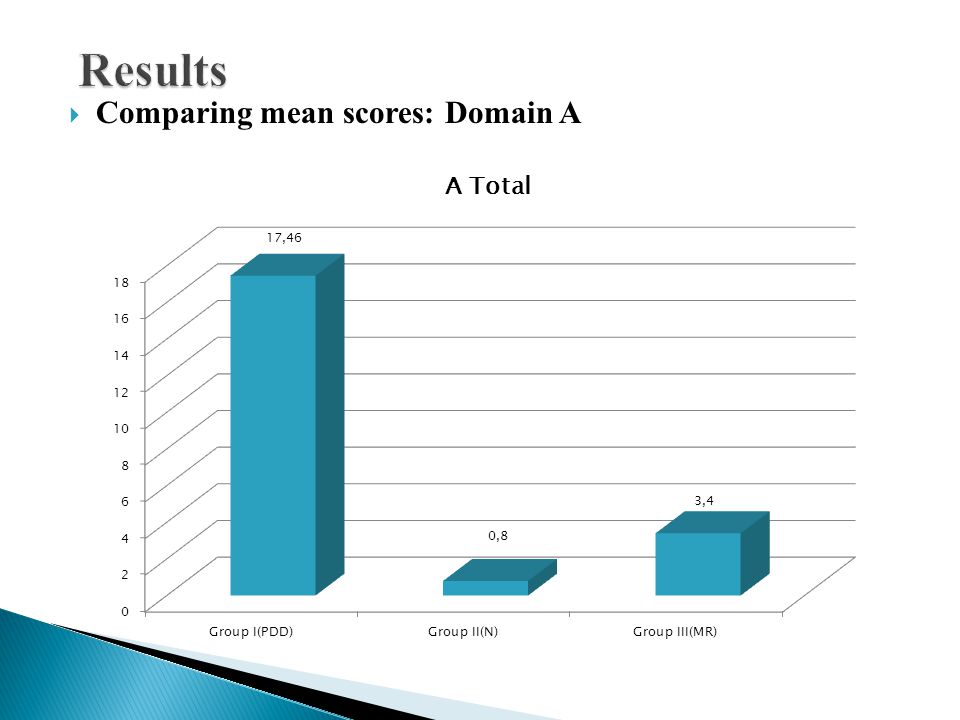
Comparing mean scores: Domain A

42
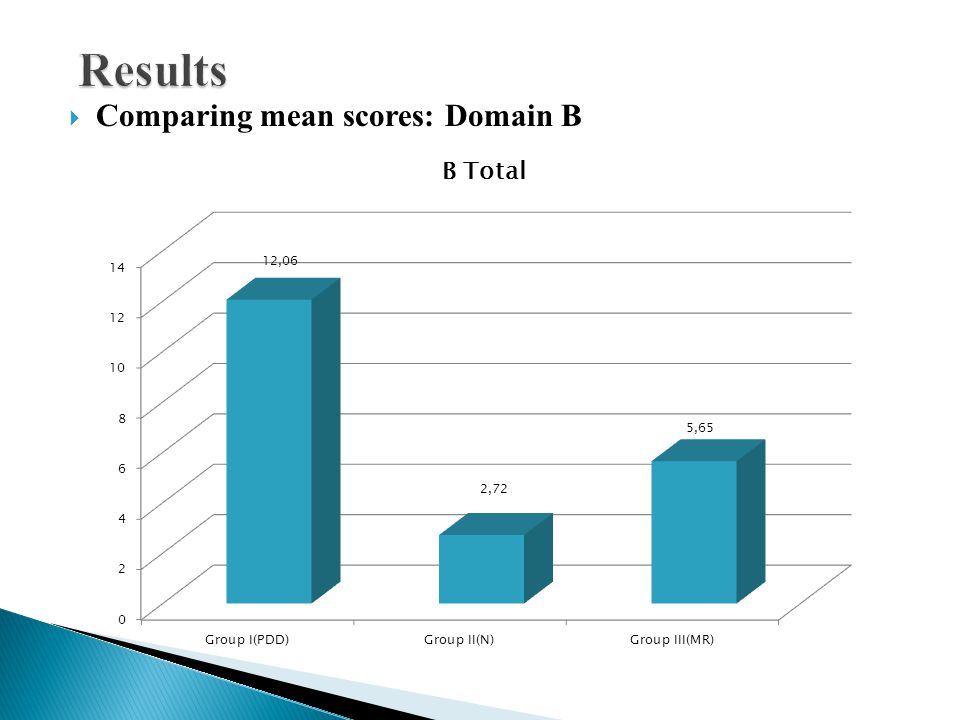
Comparing mean scores: Domain B

44
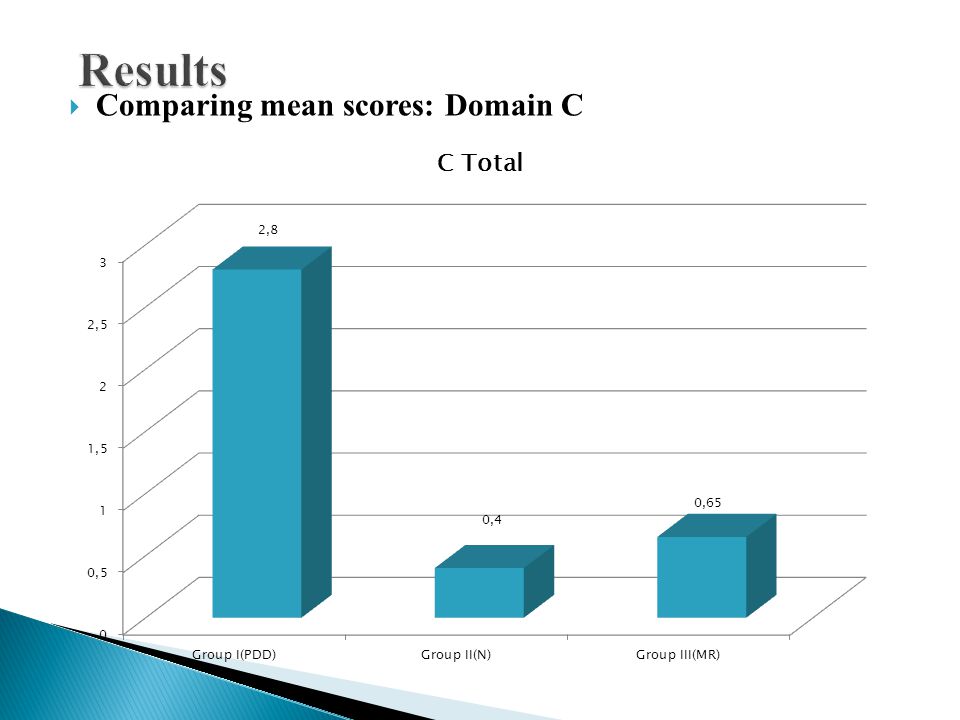
Comparing mean scores: Domain C

46
Reliability Correlation between domains A, B, C and total ADI-R score. Correlation between domains rp Total ADI-R score with domain A0.9850.001*** Total ADI-R score with domain B0.9460.001*** Total ADI-R score with domain C0.3680.01**

47
Reliability Correlation between each sub domain to its main domain.

48
Comparison between the original cutoff values and the new cutoffs NV: non verbal, V: verbal

49
Differential diagnosis: The number of children who crossed cutoff values in all domains in group I (PDD) was 26 and were diagnosed as autism. The number of children who crossed cutoff in domain A, B were 5 (suspected to be PDD-NOS ), 2 crossed cutoff in domain B only and 2 didn’t cross cutoffs in all domains.
, 2 crossed cutoff in domain B only and 2 didn’t cross cutoffs in all domains..")
50
CONCLUSION

51
1. The results of the Arabic version of ADI-R test were highly significant and were capable of discriminating between children with and without PDDs (normal, MR). 2. The high validity and reliability of the formulated test proves its sensitivity and objectivity. 3. The obtained cut-off values were near to those of the original test except for minimal differences
. 2. The high validity and reliability of the formulated test proves its sensitivity and objectivity. 3. The obtained cut-off values were near to those of the original test except for minimal differences.")
52
RECOMMENDATIONS

53
The autism diagnostic interview test is recommended to be used in mental ages above 18 months due to better sensitivity and specificity. Further evaluation is required for differentiation of other types of PDD (other than autism). Application of the test on a larger study group for its further validation.
. Application of the test on a larger study group for its further validation..")
54
American Academy of Pediatrics. The pediatrician’s role in the diagnosis and management of autistic spectrum disorder in children. Pediatrics 2001; 107: 1221- 26. American Psychiatric Association, Diagnostic and Statistical Manual of Mental Disorders (4th ed text rev), American Psychiatric Association, Washington, DC (1994). Folstein S, Rutter M. Infantile autism: A genetic study of 21 twin pairs. J Child Psychol Psychiatry 1997; 18: 297–321. Filipek PA, Filipek PJ. The screening and diagnosis of autistic spectrum disorders. J autism Deve Disord 1999; 29: 439–84. Volkmar FR, Klin A, Cohen DJ. Childhood disintegrative disorder. Handbook of autism and pervasive developmental disorders.2 nd ed. New York Wiley 1997: 47– 59. Walker DR, Walker A, Thompson L. Specifying PDD-NOS: A comparison of PDD-NOS, asperger syndrome, and autism. Journal of the American Academy of Child and Adolescent Psychiatry 2004; 43: 172–80.
, American Psychiatric Association, Washington, DC (1994). Folstein S, Rutter M. Infantile autism: A genetic study of 21 twin pairs. J Child Psychol Psychiatry 1997; 18: 297–321. Filipek PA, Filipek PJ. The screening and diagnosis of autistic spectrum disorders. J autism Deve Disord 1999; 29: 439–84. Volkmar FR, Klin A, Cohen DJ. Childhood disintegrative disorder. Handbook of autism and pervasive developmental disorders.2 nd ed. New York Wiley 1997: 47– 59. Walker DR, Walker A, Thompson L. Specifying PDD-NOS: A comparison of PDD-NOS, asperger syndrome, and autism. Journal of the American Academy of Child and Adolescent Psychiatry 2004; 43: 172–80..")
55
Spence JS, Sharifi P, Wiznitzer M. Autism Spectrum Disorder: Screening, Diagnosis and Medical evaluation. Seminars in Pediatric Neurology 2004; 11: 186- 95. Plauché Johnson C, Myers SM.Council on Children with Disabilities: Identification and evaluation of children with autism spectrum disorders. Pediatrics 2007; 120: 1183–1215. Groen BW, Zwiers PM, Jan van der Gaa R, Buitelaar KJ. The phenotype and neural correlates of language in autism: An integrative review Neuroscience and Biobahavioral Reviews 2008; 32: 1416-25.

56
Thank You

Similar presentations









: Early Screening & Diagnostic Assessment Laura Grofer Klinger, Ph.D. University of Alabama.>")









 A range of pervasive developmental disorders, with onset in childhood, that adversely affect a pupil's functioning and.>")
