Download presentation
Presentation is loading. Please wait.

1
The Pancreas 1 1

2
Outline Introduction Congenital anomalies Anatomy Acute pancreatitis
Pancreatic pseudo cysts Chronic pancreatitis Complications Pancreatic neoplasm Pancreatic cancers 2

3
Introduction Complex lobulated organ Retro-peritoneal
Exocrine and endocrine portion(digestive enzyme and hormones respectively) Endocrine pancreas :less than 1% of pancreas. Secretes insulin, somatostatin and glucagon.(discussed in endocrinology) Disorders of exocrine Pancreas includes: Congenital ,Acute/Chronic Pancreatitis, Neoplasm and Cystic fibrosis. 3
 Endocrine pancreas :less than 1% of pancreas. Secretes insulin, somatostatin and glucagon.(discussed in endocrinology) Disorders of exocrine Pancreas includes: Congenital ,Acute/Chronic Pancreatitis, Neoplasm and Cystic fibrosis. 3.")
4
Congenital anomalies Several anatomical variants. Most are not clinically significant. Pancreatic divisum =>most common clinically(incidence is 3-10%) =>Failure of fusion of the dorsal pancreatic primordium with the ventral primordium. =>the bulk of the pancreas drains through the minor sphincter =>Predisposes to chronic pancreatitis The other congenital anomalies are very rare Agenesis (usually incompatible with life) Annular pancreas – abnormal fusion =>duodenal obstruction Ectopic pancreas – stomach, duodenum, jejunum, ileum and meckel diverticulum.- inflammation and mucosal bleeds. 4 4
 =>Failure of fusion of the dorsal pancreatic primordium with the ventral primordium. =>the bulk of the pancreas drains through the minor sphincter. =>Predisposes to chronic pancreatitis. The other congenital anomalies are very rare. Agenesis (usually incompatible with life) Annular pancreas – abnormal fusion =>duodenal obstruction. Ectopic pancreas – stomach, duodenum, jejunum, ileum and meckel diverticulum.- inflammation and mucosal bleeds")
5
Anatomy – Ductal system
5 5

6
Pancreatic Acinar 6

7
Acute Pancreatitis Inflammation of Pancreas Potentially reversible
Acute alcohol/Gallstone are the leading cause. Common, incidence 10/20 cases per 100,000 >200,000 admissions/yr in U.S. Mostly mild ~10% complicated and severe ~10,000 deaths/year 7 7

8
What is the leading cause of Acute pancreatitis?

9
GET SMASHED G all stones E thanol T rauma S teroids
M umps, mycoplasma and coxsakiae A utoimmune S corpions H yperlipidaemia, hypercalcemia E RCP D rugs (thiazide diuretics, azathioprine, procainamide, frusemide, estrogens, methyl dopa) 9 9
")
10
Mechanisms of Acute Pancreatitis
Etiology dependent No established pathogenesis Three widely accepted pathways: - Pancreatic duct obstruction - Primary Acinar cell injury -Defective transport of Pro-enzymes 10 10

11
11

12
Acute Pancreatitis 12 12

13
Acute Pancreatitis Morphology: Variable picture;
from Mild inflammation and edema to severe necrosis of the parenchyma and hemorhage. 13 13

14
Clinical Presentation
Pain - “steady, dull”- epigastric/upper quadrant, radiation to the back Commonly worse on supine position No peritoneal sign - since retroperitoneal location Nausea/Vomitting Fever 14 14

15
Clinical Presentation
Hypotension/Shock (30~40%) Plasma exudation to retroperitoneal space Increased peripheral vascular permeability Hemorrhage Vomiting Peripheral vasodilatation 15 15
 Plasma exudation to retroperitoneal space. Increased peripheral vascular permeability. Hemorrhage. Vomiting. Peripheral vasodilatation")
16
Cutaneous signs of hemorrhagic pancreatitis
Grey Turner Sign Cullen Sign 16 16

17
Labs Serum amylase Rises in AP 2~12hrs after onset and stays up for 3~5 days The magnitude of elevation is not related to prognosis Sensitivity=80~90% ,Specificity=70% Serum lipase Tends to be elevated several days longer than amylase levels Sensitivity=87% Specificity=90% Serum amylase & lipase: Sensitivity=95% Specificity=90% 17 17

18
Diagnostic Testing: Imaging Studies
CXR/Plain abdominal films – dilated bowel loops CT scan – diagnosis, predict outcome/prognosis Abdominal Ultrasound – detects stone ( in gallbladder & bile duct) May be difficult to evaluate pancreas in up to 30% of cases due to overlying bowel gas 18 18
 May be difficult to evaluate pancreas in up to 30% of cases due to overlying bowel gas")
19
Imaging Studies ERCP (Endoscopic Retrograde Cholangio- Pancreatography) Diagnosis - Confirm presence of common duct stones Therapy - Removal of common bile duct stone in severe pancreatitis patients 19 19

20
Acute Pancreatitis-Outcome
Peritonitis Pseudocysts Abscesses Chronic pancreatitis Diabetes mellitus(rare) 20 20
")
21
Prognostic Indicators
Ranson’s Criteria: Original Criteria for classification of pancreatitis 21 21

22
Ranson’s Criteria Assessment of Severity in Acute Pancreatitis 22 22

23
Ranson’s Criteria < 3 signs = excellent prognosis
3~5 signs = 10 – 20% mortality 6 signs = > 50% mortality General rule: 3 signs Severe Pancreatitis 23 23

24
Pancreatic Pseudocysts
Collection of enzyme-rich pancreatic fluid and tissue debris arising within areas of necrosis or an obstructed smaller duct. It is not surrounded by a true capsule. Death is caused by secondary infection, hemorrhage, or rupture. 24 24

25
25

26
Chronic Pancreatitis 26 26

27
Definition A persistent inflammatory disease of the pancreas
Irreversible morphologic changes Typically causing pain and/or loss of digestive function 27 27

28
Etiologies of Chronic Pancreatitis
Alcohol (~70% of CP) Hereditary-Genetic mutation. => PRSSI =>Spink1 Obstruction Trauma Pancreas divisum Tropical Hyperparathyroidism Idiopathic-40% truly idiopathic. Most are due to hereditary causes. -CFTR mutations(cystic Fibrosis) is cause of Idiopathic chronic pancreatitis. 28 28
 Hereditary-Genetic mutation. => PRSSI. =>Spink1. Obstruction. Trauma. Pancreas divisum. Tropical. Hyperparathyroidism. Idiopathic-40% truly idiopathic. Most are due to hereditary causes. -CFTR mutations(cystic Fibrosis) is cause of Idiopathic chronic pancreatitis")
29
Chronic Pancreatitis Gross Fibrotic & firm Pancreatic duct
Dilated Stones Constriction Common bile duct Duodenum Pyloris 29 29

30
Chronic Pancreatitis Histology Fibrosis
Scattered foci of chronic inflammation Ducts & islets of Langerhans persist Calcifications 30 30

31
31 Downloaded from: StudentConsult (on 6 October 2011 01:04 PM)
© 2005 Elsevier 31

32
Clinical Presentation
Abdominal pain - primary feature Weight loss 15 – 25% CP may be painless Malabsorption/steatorrhea – usually occurs when enzyme secretion < 10% of normal Diabetes (usually a late finding) 32 32
")
33
Diagnosis Frequently made by history alone
e.g. an alcoholic with recurrent attacks Plain abdominal X-ray - calcification in ~30% diagnostic in clinically suspected patients Serum amylase & lipase usually elevated - can be normal 33 33

34
Chronic pancreatitis 34 34

35
Imaging abdominal ultrasound or CT (shows abnormalities in size and consistency of the pancreas, pancreatic pseudocyst, or dilated pancreatic ducts. ERCP shows abnormalities of the main pancreatic duct and secondary branches 35 35

36
Complications of Chronic Pancreatitis
Pseudocyst Pancreatic ascites Pancreatic fistula Weight loss/ malabsorption Pancreatic carcinoma -40%lifetime risk of pancreatic CA in those with hereditary pancreatitis Role of chronic pancreatitis in pancreatic CA is otherwise inconclusive. Common bile duct obstruction Splenic /portal vein thrombosis 36 36

37
Cystic neoplasm 5-15% of pancreatic cysts are neoplastic
Most cysts in the pancreas are pseudodocysts Three common types of neoplastic cysts. Serous - Benign, more in females Mucinous (always in females) Intraductal papillary mucinous neoplasms (IPMN)..more in males Both Mucinous and IPMN could present as:benign,borderline or malignant tumors 37 37
 Intraductal papillary mucinous neoplasms. (IPMN)..more in males. Both Mucinous and IPMN could present as:benign,borderline or malignant tumors")
38
Pancreatic Cancer 31,800 new cases, 31,200 deaths in 2004 U.S.
5-yr Survival Rate: <4% ~10-20% resectable at diagnosis Difficult to treat by ChemoXRT due to its highly resistant nature 4th cause of cancer related death 38 38

39
PANCREATIC CANCER ETIOLOGY. I. poorly characterized
60-80 yrs,Blacks>whites, Increased risk in Jews cigarette smoking (2-3 times)- Smoking is the most significant environmental risk factor Association with: chronic pancreatitis; causal relationship established with hereditary forms only. long-standing D/M.(not clear whether cause or consequences since ca pancreas could cause D/M) No correlation with: Alcohol and coffee abuse Cholelithiasis 39 39
- Smoking is the most significant environmental risk factor. Association with: chronic pancreatitis; causal relationship established with hereditary forms only. long-standing D/M.(not clear whether cause or consequences since ca pancreas could cause D/M) No correlation with: Alcohol and coffee abuse. Cholelithiasis")
40
Pancreatic Cancer Etiology II.
Familial syndromes: Peutz-Jeghers Hereditary Pancreatitis(PRSSI mutation) Familial atypical multiple mole melanoma syndrome,FAMMM(p16) Hereditary breast and ovarian cancer (BRCA2) Hereditary non polyposis colorectal cancer Lynch II,(hMSH2)
 Familial atypical multiple mole melanoma syndrome,FAMMM(p16) Hereditary breast and ovarian cancer (BRCA2) Hereditary non polyposis colorectal cancer Lynch II,(hMSH2)")
41
Molecular Carcinogenesis
Pancreatic intraepithelial neoplasm ,PanIN,is the putative precursor lesion Telomere shortening in PanINs leads to accumulation of progressive chromosomal abnormalities. K-RAS oncogene is activated,while the tumor suppressor genes ( P53, P16,SMAD4).are inactivated. SMAD4 appears to be the more specific tumor suppressor gene involved
.are inactivated. SMAD4 appears to be the more specific tumor suppressor gene involved.")
42
Figure 17-8 Model for the development of pancreatic cancer
Figure 17-8 Model for the development of pancreatic cancer. It is postulated that telomere shortening, and mutations of the oncogene K-RAS occur at early stages, inactivation of the p16 tumor suppressor gene occurs at intermediate stages, and the inactivation of the p53, SMAD4, and BRCA2 tumor suppressor genes occurs at late stages. Note that while there is a general temporal sequence of changes, the accumulation of multiple mutations is more important than their occurrence in a specific order. (Adapted from Wilentz RE, et al.: Loss of expression of Dpc4 in pancreatic intraepithelial neoplasia: evidence that DPC4 inactivation occurs late in neoplastic progression. Cancer Res 60:2002, 2000.) Downloaded from: StudentConsult (on 7 October :16 PM) © 2005 Elsevier
 Downloaded from: StudentConsult (on 7 October :16 PM) © 2005 Elsevier.")
43
Anatomical Prevalence
Head of Pancreas: ~70% of the cases, presenting as jaundice or pancreatic insufficiency CBD PD 43 43

44
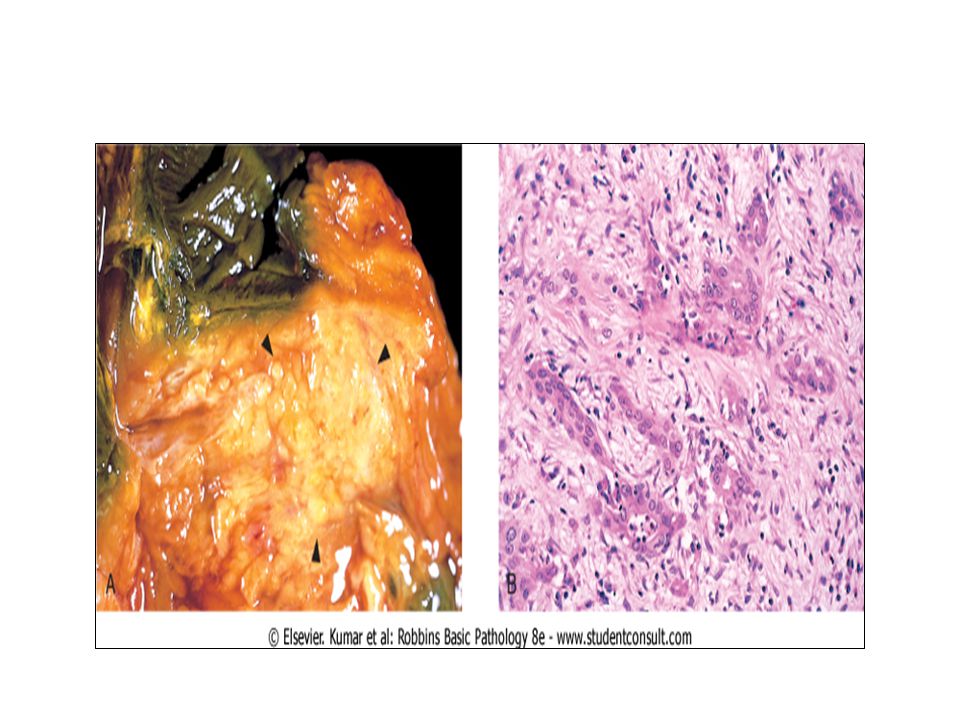
Morphology and Histology
Ductal adenocarcinomas Often poorly differentiated Highly invasive Desmoplasia Poorly formed glands in a densely fibrotic stroma on histology.

46
PRESENTING SIGNS AND SYMPTOMS OF PANCREATIC CARCINOMA
FREQUENT abdominal pain; anorexia and weight loss; jaundice (lesions of pancreatic head only); INFREQUENT glucose intolerance; palpable gallbladder with painless jaundice (Courvoisier's sign); migratory thrombophlebitis (Trousseau’ sign); gastrointestinal hemorrhage; *splenomegaly
; INFREQUENT. glucose intolerance; palpable gallbladder with painless jaundice (Courvoisier s sign); migratory thrombophlebitis (Trousseau’ sign); gastrointestinal hemorrhage; *splenomegaly.")
47
Diagnosis No effective screening
Imaging studies,CT are good for diagnosis and prognosis CA 19-9, carcinoembryonic antigen, are tumor markers but unreliable;lack specificity Poor prognosis

48
Progression Adenocarcinomas appear at the mean age of 55 yr and occur 1.5 to 2 times more often in men. locally invasive Direct invasion of retroperitoneal structures, spread to regional lymph nodes, Distant Metastasis

Similar presentations




 EXOCRINE PANCREASE Lecture Dr. Gamal Hamra Wednesday 01/12/1430 (18/11/2009)>")














