Download presentation
Presentation is loading. Please wait.

1
Living Donor Kidney Transplantation in Hereditary Nephropathy Patients
Reference: Niaudet P. Nat. Rev. Living donor kidney transplantation in patients with hereditary nephropathies. Nephrol. 2010;6:736–743.

2
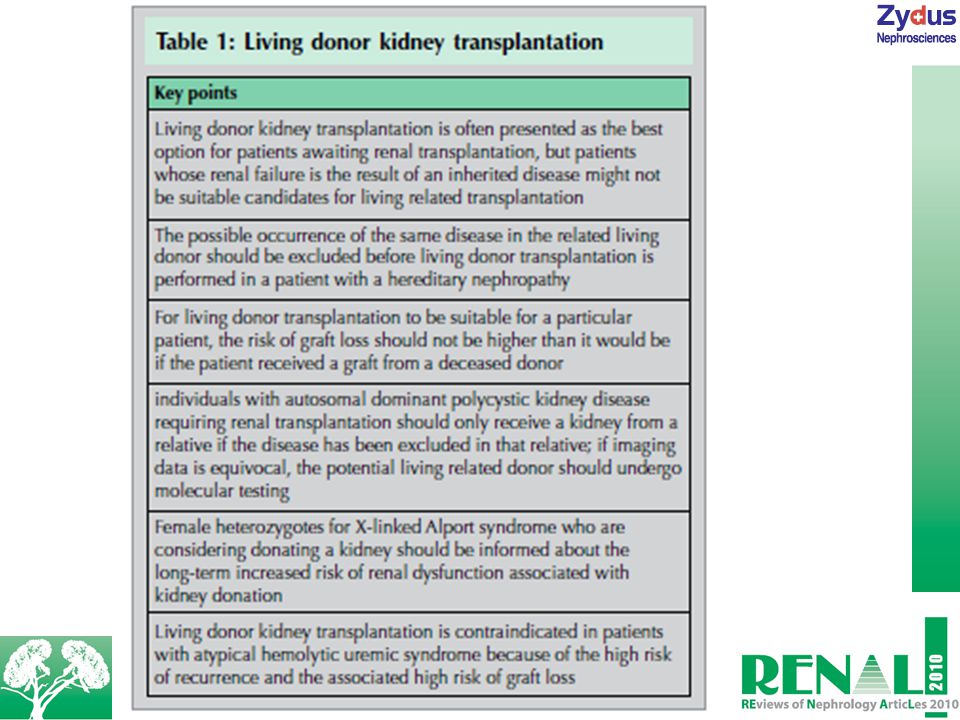
Kidney transplantation (KT) from living donors is regarded as the best option for renal transplantation recipients. Those recipients who receive kidney grafts from the living donor generally have shorter waiting times compared to those who receive from deceased donors. However, grafts from living donors are not suitable for recipients who had renal failure due to genetic causes. In recipients with a genetic disorder, the probable incidence of the same disease in the associated potential donor should be debarred. In some cases, the disease can get elicited due to the graft donated. The living donor KT is generally thought to be suitable in patients with nephronophthisis, autosomal recessive polycystic kidney disease, congenital nephrotic syndrome of the Finnish type and cystinosis. Table 1 depicts some of the key points related to living donor KT.

4
Autosomal Dominant Polycystic Kidney Disease
Autosomal dominant polycystic kidney disease (ADPKD), a very common genetic renal disease, accounts for more than 5% of cases of end-stage renal disease (ESRD) in Europe and North America. The KT recipients should be examined using direct sequence analysis for ADPKD-related mutation and in case of positive results the potential donor should also be tested for the same. In at-risk recipients <30 years old, CT scanning or heavily T2-weighted MRI can help detect small cysts; but however, in case of negative results, indirect and/or direct molecular genetic testing of the polycystic kidney disease (PKD1) and PKD2 genes should be considered. Living donation is contraindicated in potential donors aged <30 years old for whom imaging techniques do not show cysts but for whom genetic tests show positive results for mutated PKD genes, although no data exist on the risk of ESRD in such individuals.
, a very common genetic renal disease, accounts for more than 5% of cases of end-stage renal disease (ESRD) in Europe and North America. The KT recipients should be examined using direct sequence analysis for ADPKD-related mutation and in case of positive results the potential donor should also be tested for the same. In at-risk recipients <30 years old, CT scanning or heavily T2-weighted MRI can help detect small cysts; but however, in case of negative results, indirect and/or direct molecular genetic testing of the polycystic kidney disease (PKD1) and PKD2 genes should be considered. Living donation is contraindicated in potential donors aged <30 years old for whom imaging techniques do not show cysts but for whom genetic tests show positive results for mutated PKD genes, although no data exist on the risk of ESRD in such individuals.")
5
Alport Syndrome Alport syndrome, an inherited glomerular disease, is characterized by the familial occurrence of a progressive hematuric nephropathy related with sensorineural deafness and ultrastructural changes in the glomerular basement membrane (GbM). In the X-linked form of Alport syndrome, renal disease is seen to be more acute in males as compared to females, with the affected males progressing to ESRD at a mean age of 21 years. For transplant candidates with Alport syndrome, screening tests for potential living kidney donors include urinalysis, glomerular filtration rate estimation, and sight and hearing test.
. In the X-linked form of Alport syndrome, renal disease is seen to be more acute in males as compared to females, with the affected males progressing to ESRD at a mean age of 21 years. For transplant candidates with Alport syndrome, screening tests for potential living kidney donors include urinalysis, glomerular filtration rate estimation, and sight and hearing test.")
6
Male siblings aged >20 years without hematuria are suitable donors for a recipient with Alport syndrome. Sisters of affected male recipients with Xlinked disease are at a 50% risk of being carriers; however, in the affected brother associated with a neomutation there is no potential risk. Female carriers of the abnormal gene that leads to Xlinked Alport syndrome will develop renal failure. For a patient with Xlinked Alport syndrome, a female relative without hematuria could be an appropriate donor. The female heterozygous potential donors with no proteinuria, microhematuria, and a normal glomerular filtration rate should only be permitted to donate a kidney, after a detailed consultation with a nephrologist and a geneticist. Individuals with isolated microhematuria are eligible donors; however, they should be counseled about the ambiguity of long-term renal function. In addition, both the potential kidney donor and the recipient with Alport syndrome should also be educated about the possible occurrence of an anti-GbM antibody disease that occurs in about 3% of renal transplant recipients with Alport syndrome, with the male transplant recipients with Xlinked disease being at the highest risk.

7
Fabry Disease Fabry disease, an Xlinked recessive metabolic disease is caused by the deficient activity of the lysosomal enzyme α-galactosidase A. Most of the affected males require renal replacement therapy by the time they reach 35–45 years of age. Heterozygote females have a different clinical course with variable clinical manifestations owing to random X‑chromosome inactivation. Renal transplantation from the heterozygote female donor is unsafe as the accumulation of globotriaosylceramide might be already present in the donor, even in the absence of any clinical symptoms. It has been observed that the renal function of a heterozygous female reduced 5 years after the kidney was transplanted to a male relative with Fabry disease.

8
Hemolytic Uremic Syndrome
Hemolytic uremic syndrome (HuS) can persist after renal transplantation. In patients with Shiga-like toxinassociated HuS, who advance into ESRD and undergo renal transplantation, reappearance of HuS in the transplanted kidney is very rare. However, recurrence is a major concern in patients with non-Shiga toxin-associated (atypical) HuS. Patients with an inherited form of HuS are at a higher risk of recurrence following renal transplantation, with the risk being even greater in patients who have complement factor I (CFI) mutations. Living-related donation should be prevented in patients with complement factor H or CFI mutations due to the high risk of HuS recurrence. Living related donors, carrying the mutation, are at a risk of developing de novo disease after donating a kidney to a family member with atypical HuS. The risk of HuS recurrence is low in patients with CD46 mutations. It is advised that genotyping for complement protein genes should be carried out in patients who have atypical HuS and ESRD and are being considered for renal transplantation.
 can persist after renal transplantation. In patients with Shiga-like toxinassociated HuS, who advance into ESRD and undergo renal transplantation, reappearance of HuS in the transplanted kidney is very rare. However, recurrence is a major concern in patients with non-Shiga toxin-associated (atypical) HuS. Patients with an inherited form of HuS are at a higher risk of recurrence following renal transplantation, with the risk being even greater in patients who have complement factor I (CFI) mutations. Living-related donation should be prevented in patients with complement factor H or CFI mutations due to the high risk of HuS recurrence. Living related donors, carrying the mutation, are at a risk of developing de novo disease after donating a kidney to a family member with atypical HuS. The risk of HuS recurrence is low in patients with CD46 mutations. It is advised that genotyping for complement protein genes should be carried out in patients who have atypical HuS and ESRD and are being considered for renal transplantation.")
9
Primary Hyperoxaluria
Primary hyperoxaluria, a rare metabolic disease with an autosomal recessive form of inheritance, is caused by a deficiency of alanine–glyoxylate aminotransferase (AGT). In patients with primary hyperoxaluria, living donor KT is controversial due to the associated risk of recurrence. However, according to some groups, early living donor transplantation could be carried out, particularly in adults who have late onset and slowly progressive disease that is responsive to pyridoxine. Heterozygote family members of patients with primary hyperoxaluria have vaguely lower AGT enzyme activity as compared to controls, but they do not develop renal stones. A living related donor for an isolated renal transplantation for a patient with primary hyperoxaluria should be examined for normal oxalate and glycolate urine excretion levels.
. In patients with primary hyperoxaluria, living donor KT is controversial due to the associated risk of recurrence. However, according to some groups, early living donor transplantation could be carried out, particularly in adults who have late onset and slowly progressive disease that is responsive to pyridoxine. Heterozygote family members of patients with primary hyperoxaluria have vaguely lower AGT enzyme activity as compared to controls, but they do not develop renal stones. A living related donor for an isolated renal transplantation for a patient with primary hyperoxaluria should be examined for normal oxalate and glycolate urine excretion levels.")
10
Familial FSGS In patients with idiopathic nephrotic syndrome and focal segmental glomerulosclerosis (FSGS), who progress to ESRD, are at risk of recurrence of the nephrotic syndrome following renal transplantation. The overall risk of recurrence being projected to be 20–30%. Genetic analysis of patients with steroid-resistant nephrotic syndrome is useful. It is advisable that a parent of a child carrying two pathogenic mutations in NPHS2, undergoes test for the Arg229Gln (p.R229Q) variant prior to living donor transplantation, as they could be at adult-onset steroid-resistant nephrotic syndrome risk.
, who progress to ESRD, are at risk of recurrence of the nephrotic syndrome following renal transplantation. The overall risk of recurrence being projected to be 20–30%. Genetic analysis of patients with steroid-resistant nephrotic syndrome is useful. It is advisable that a parent of a child carrying two pathogenic mutations in NPHS2, undergoes test for the Arg229Gln (p.R229Q) variant prior to living donor transplantation, as they could be at adult-onset steroid-resistant nephrotic syndrome risk.")
11
Conclusion Prior to considering a living donor as a suitable choice for a patient with a hereditary nephropathy, a careful evaluation involving both a nephrologist and a geneticist is required to investigate the risks involved for the recipient and donor. The transplantation outcomes are also affected by the age at onset, the mode of inheritance and the clinical features of the original disease. Genetic testing is suggested in case if the potential living donor is a relative of the renal transplant recipient with a hereditary disease. Living donor transplantation should be prevented in patients who have diseases with a high risk of posttransplantation recurrence, like atypical primary hyperoxaluria or HuS.

Similar presentations