Download presentation
Presentation is loading. Please wait.

1
Aortic root surgery Decision making
Kriengchai Prasongsukarn, MD, MSc

2
Case 1 Case ผู้หญิงไทย อายุ 25 ปี underlying Marfan’s syndrome, married, want to pregnant CXR:Dilatation of ascending aorta Echo/TEE: severe AR ,EF 70%,no RWMA, dilated aortic root at sinus part of aorta 5.05 cm, LVOT 2.4 cm, Ascending aortic dilate 5.6 cm indiameter

3
Operation ? Tissue Valve/ Homograft Replacement
Mechanical Valve Replacement Composite valve graft (Bentall operation) Ross Operation Aortic valve sparing
 Ross Operation. Aortic valve sparing.")
4
Case 2 Case ผู้หญิงไทย อายุ 22 ปี
DX severe AS (อายุ 19 ปี ) s/p AV commissurotomy หลังทำ3 months มีเหนื่อย ประมาณ 1-2 เดือน หลังจากคลอดบุตรคนแรกผู้ป่วยเหนื่อยมากขึ้น ตรวจพบว่ามี severe AR, ผู้ป่วยมาปรึกษาแพทย์ว่าถ้าหลังจากการผ่าตัดแล้ว ผู้ป่วยยังอยากที่จะมีบุตรต่อ
 s/p AV commissurotomy หลังทำ3 months มีเหนื่อย. ประมาณ 1-2 เดือน หลังจากคลอดบุตรคนแรกผู้ป่วยเหนื่อยมากขึ้น ตรวจพบว่ามี severe AR, ผู้ป่วยมาปรึกษาแพทย์ว่าถ้าหลังจากการผ่าตัดแล้ว ผู้ป่วยยังอยากที่จะมีบุตรต่อ.")
5
Case 2 Echo: EF 62%, Severe AR (regurgitation flow 1114 ms., PHT 323 ms.), tricuspid and torn leaflet, no calcification
, tricuspid and torn leaflet, no calcification.")
6
Operation ? Tissue Valve/ Homograft Replacement
Mechanical Valve Replacement Composite valve graft (Bentall operation) Ross Operation Aortic valve sparing
 Ross Operation. Aortic valve sparing.")
7
Case 3 Case ผู้ชายไทยอายุ 21 ปี severe AR ผู้ป่วยมาปรึกษาแพทย์ เรื่องการผ่าตัดว่า หลังการผ่าตัดผู้ป่วยไม่ขอ on anticoagulant Echo: EF 61%, severe AR (PHT ms.), LVEDD 65 mm, LV enlargement, Aortic annulus 2.75 cm., Pulmonic valve cm., Aortic Valve are trileaflets, retracted and rolling.
, LVEDD 65 mm, LV enlargement, Aortic annulus 2.75 cm., Pulmonic valve cm., Aortic Valve are trileaflets, retracted and rolling.")
8
Operation ? Tissue Valve/ Homograft Replacement
Mechanical Valve Replacement Composite valve graft (Bentall operation) Ross Operation Aortic valve sparing
 Ross Operation. Aortic valve sparing.")
9
Case 4 Case ผู้ชายไทย อายุ 24 ปี มาด้วย ไข้ เหนื่อย
Dx:BE with severe AR, รักษาได้ ATB ครบ 6 wk คลำได้ก้อนที่บริเวณก้นด้านซ้าย(AVM at left buttock) Echo:Severe AR, EF 60%, Aortic root 28.8 mm, sinotubular junction 28 mm, aortic root 24.8 mm, tricuspid AV, vegetation size 24x9.9 mm attached to left cusp and down to septum, pulmonic valve 24. mm
 Echo:Severe AR, EF 60%, Aortic root 28.8 mm, sinotubular junction 28 mm, aortic root 24.8 mm, tricuspid AV, vegetation size 24x9.9 mm attached to left cusp and down to septum, pulmonic valve 24. mm.")
10
Operation ? Tissue Valve/ Homograft Replacement
Mechanical Valve Replacement Composite valve graft (Bentall operation) Ross Operation Aortic valve sparing
 Ross Operation. Aortic valve sparing.")
11
Case 5 Case ผู้ชายไทย อายุ 40 ปี มาด้วยเหนื่อยมากขึ้นขณะสอนหนังสือ
CXR: Dilatation of of ascending aorta CTA: Aortic aneurysm at ascending aorta size 6.2 cm in diameter. Echo: moderate AR, EF 48%, ascending aortic aneurysm 6 cm in diameter, no evidence of ascending aortic dissection, LVOT 4.2 cm, STJ 5.2 cm, tubular diameter 4.2 cm, AV 3 leaflets, no MR/MS

12
Operation ? Tissue Valve/ Homograft Replacement
Mechanical Valve Replacement Composite valve graft (Bentall operation) Ross Operation Aortic valve sparing
 Ross Operation. Aortic valve sparing.")
13
Case 6 female 59 years old, chest pain, FC III
CXR: Dilatation of of ascending aorta Echo: moderate AR, EF 39%, ascending aortic aneurysm 5 cm in diameter, no evidence of ascending aortic dissection, sinus valsava 6 cm, AV 3 leaflets rolling and retracted of leaflets, mild MR

14
Operation ? Tissue Valve/ Homograft Replacement
Mechanical Valve Replacement Composite valve graft (Bentall operation) Ross Operation Aortic valve sparing
 Ross Operation. Aortic valve sparing.")
15
Tissue valve

16
AVR - Hancock II Bioprosthesis from TGH
670 patients Mean age: 65+/-12 years (range 18 to 87) Sex: male % female - 25% ECG: sinus - 92% AF % Previous AVR - 10%
 Sex: male - 75% female - 25% ECG: sinus - 92% AF - 8% Previous AVR - 10%")
17
AVR - Hancock II Bioprosthesis
NYHA functional class I % II - 23% III - 43% IV - 31% AV lesion: AS - 46% AI % Mixed %

18
AVR - Hancock II Bioprosthesis
Infective endocarditis: Active - 24 pts Healed - 11 pts Coronary artery disease: pts (44%) Ascending aortic aneurysm: 73 pts (11%) Left ventricular EF: >40% pts (64%) <40% pts (21%) N.A pts (15%)
 Ascending aortic aneurysm: 73 pts (11%) Left ventricular EF: >40% pts (64%) <40% pts (21%) N.A pts (15%)")
19
AVR - Hancock II Bioprosthesis
Operative Data: Valve size: #21 = 48 pts (7%) #23 = 198 pts (30%) #25 = 208 pts (31%) #27 = 174 pts (26%) #29 = 42 pts (6%) Aortic annulus enlargement: 125 pts (19%) #21=24 pts; #23=53 pts; #25=58 pts
 #23 = 198 pts (30%) #25 = 208 pts (31%) #27 = 174 pts (26%) #29 = 42 pts (6%) Aortic annulus enlargement: 125 pts (19%) #21=24 pts; #23=53 pts; #25=58 pts.")
20
AVR - Hancock II Bioprosthesis
Operative mortality - 32 pts (5%) Operative morbidity: Bleeding/tamponade - 33 (5%) Myocardial infarction - 9 (1.3%) Stroke/TIA (3.2%) Sternal infection - 4 (0.6%) Early endocarditis - 2 (0.3%)
 Operative morbidity: Bleeding/tamponade - 33 (5%) Myocardial infarction - 9 (1.3%) Stroke/TIA - 22 (3.2%) Sternal infection - 4 (0.6%) Early endocarditis - 2 (0.3%)")
21
AVR - Hancock II Bioprosthesis
Follow-up: 86+/-45 mo. (range ) 99% complete Deaths: Total (35.3%) Operative - 32 (13.5%) Valve-related (12%) Cardiac-related (34%) Other causes (40.5%)
 99% complete. Deaths: Total (35.3%) Operative - 32 (13.5%) Valve-related - 28 (12%) Cardiac-related - 81 (34%) Other causes - 96 (40.5%)")
22
Hancock II: AVR Survival

23
Hancock II: AVR Free From Structural Valve Dysfunction

24
Hancock II: AVR Free From Structural Valve Dysfunction

25
Hancock II: AVR Free From Reoperation

26
AVR: Hancock II Bioprosthesis Summary of Events
5yr 10yr 15yr Freedom from: Death 79% 61% 47% Thromboembolism 95% 87% 83% Endocarditis 98% 97% 96% Tissue failure 100% 97% 81% Reoperation 98% 94% 77%

27
AVR: CE Perimount CE Perimount No. Patients 310
Mean Age +/-S.D /-12 NYHA class IV % Coronary artery disease % Banbury et al - Ann Thorac Surg – 2001;72:753

28
AVR with CE Perimount Freedom from Failure
15 yr = 77% Banbury et al - Ann Thorac Surg – 2001;72:753

29
The Journal of Thoracic and Cardiovascular Surgery
October 2005 Carpentier-Edwards supra-annular aortic porcine bioprosthesis: Clinical performance over 20 years W.R.Eric Jamieson and colleagues

30
AV Bioprostheses: Freedom from Tissue Failure
Pt’s age years Hancock II David et al ± % Rizolli et al ± % CE Perimount Banbury et al ± % Neville et al ± % (12yr) Frater et al ± % (14yr) SJM Biocor % CE porcine %
 Frater et al 65±12 85% (14yr) SJM Biocor 69 76% CE porcine 69 75%")
31
AV Bioprostheses Freedom from Failure
Jamieson’s discussion “There is no apparent difference in failure rates of second generation porcine valves and CE Perimount…”

32
Homograft

33
AVR with Aortic Valve Homograft
Versatile: Sub-coronary implantation Aortic root inclusion Aortic root replacement Excellent flow characteristics, particularly when used as an aortic root replacement device Drawbacks: Limited availability Limited durability

34
Durability of Aortic Valve Homograft

35
AVR with Aortic Valve Homograft Freedom from Reoperation
10 year = 87% 15 year = 76% Pts’ mean age = 47 yrs Pts at risk O’Brien et al. J Heart Valve Dis 2001;10:334

36
AVR with Aortic Valve Homograft
Freedom from reoperation Freedom from failure

37
AVR with Aortic Valve Homograft Freedom from Reoperation & Failure
10-year % % 20-year % % Lund et al. J Thorac Cardiovasc Surg 1999;117:77

38
AVR with Aortic Valve Homograft
Drawbacks: Limited availability Limited durability Complicated reoperation: high op mortality Better than xenografts?

39
Stentless valve

40
AVR with Medtronic Freestyle Freedom from Reoperation
10 yr = 92% Pts at risk Bach et al. – Ann Thorac Surg 2005;80:480

41
AVR with Medtronic Freestyle Freedom from Moderate/Severe AI
10-year: Sub-coronary = 87% Root replaced = 98% Pts’ mean age = 72 years Bach et al. – Ann Thorac Surg 2005;80:480

42
AV Homograft vs. Medtronic Freestyle
Medina et al. Three-dimensional in vivo characterization of calcification in native valves and in Freestyle versus homograft aortic valves J Thorac Cardiovasc Surg 2005;130:41 Quantitative evaluation of calcium deposits in the aortic valve by electron beam tomography data fusion technique: Freestyle had lower amounts of calcium than aortic valve homograft 2 years after implantation

44
Choice of Valve in Active Infective Endocarditis of the Aortic Valve
Conventional wisdom Aortic valve homograft is the best valve to treat patients with active infective endocarditis, particularly if an abscess is present

45
Aortic Root Replacement with Aortic Valve Homograft
213 patients Mean age: 51 years Indication for surgery: 73 – Native AV endocarditis 52 – Prosthetic AV endocarditis All 213 patients had aortic root replacement Operative mortality 16/213 (7.5%) 58% Kaya et al. – Ann Thorac Surg 2005;79:1491
 58% Kaya et al. – Ann Thorac Surg 2005;79:1491.")
46
Aortic Root Replacement with Aortic Valve Homograft
Freedom from adverse events (survivors only): 5-year year Freedom from death % % Freedom from reoperation % % Kaya et al. – Ann Thorac Surg 2005;79:1491
: 5-year 10-year. Freedom from death 87% 71% Freedom from reoperation 94% 76% Kaya et al. – Ann Thorac Surg 2005;79:1491.")
47
Aortic Root Replacement with Aortic Valve Homograft
Reasons for reoperation: 20/194 12 – Homograft failure 3 – False aneurysm 3 – Endocarditis in the homograft 3 – Other reasons Reoperation mortality: 25% Endocarditis in the homograft: 4 cases Kaya et al. – Ann Thorac Surg 2005;79:1491

48
Aortic Valve Homograft for Aortic Root Abscess
: 161 patients 78 sub-coronary implantation 83 aortic root replacement 83 aorto-ventricular discontinuity 81 prosthetic valve endocarditis Operative mortality: 9.3% urgent; 14.3% emergent 11 early reoperations for dehiscence/infection 73% free from reoperation at 10 years Yankah et al - Eur J Cardio-Thorac Surg 2005;28:69

49
Aortic Valve Surgery for Active Infective Endocarditis
Infection limited to valve cusps = simple AVR Infection extended into paravalvular tissues = radical resection of all seemingly infected tissues and reconstruction with appropriate patches

50
Surgery for Active Infective Endocarditis Experience at Toronto General Hospital
418 patients Mean age: 52±16 years Sex: 65% male Native valve: 287 (68%) Prosthetic valve: 131 (32%) Paravalvular abscess: 150 (36%)
 Prosthetic valve: 131 (32%) Paravalvular abscess: 150 (36%)")
51
Surgery for Active Infective Endocarditis Experience at Toronto General Hospital
Operations performed 268 replacement/repair of one (212 patients) or two or more valves (56 patients) NO aortic homograft used 150 reconstruction of annulus + valve replacement of one (88 patients) or two or more valves (62 patients) 18 aortic homograft used Mechanical valves in 42%; tissue valves in 55%; valve repair alone in 3%
 or two or more valves (56 patients) NO aortic homograft used. 150 reconstruction of annulus + valve replacement of one (88 patients) or two or more valves (62 patients) 18 aortic homograft used. Mechanical valves in 42%; tissue valves in 55%; valve repair alone in 3%")
52
Surgery for Active Infective Endocarditis Experience at Toronto General Hospital
Operative mortality: 11.5% Predictors: Odds ratio Shock 5.2 Prosthetic valve 3.2 Preop renal failure 2.3 (Surgeon was a predictor of operative mortality in patients with prosthetic valve and/or abscess)
")
53
Surgery for Active Infective Endocarditis Survival
5 year = 74% 10 year = 63% 15 year = 45% Pts at risk

54
Surgery for Active Infective Endocarditis Survival: Valve vs. Abscess
1 year year Valve % % Abscess 81% %

55
Surgery for Active Infective Endocarditis Freedom from Recurrent Endocarditis
5 year = 93% 10 year = 88% 15 year = 86% Pts at risk

56
Surgery for Active Infective Endocarditis Freedom from Reoperation
5 year = 97% 10 year = 91% 15 year = 71% Pts at risk

57
Surgery for Active Infective Endocarditis Conclusions
Continues to be associated with high operative mortality and morbidity, particularly in patients with aortic root abscess Radical resection of all infected tissues is probably more important than the valve implanted as far as the chances of curing the endocarditis

58
Conclusions Homograft
AV homograft offers no advantage over xenograft valves in patients with aortic stenosis AV homograft may be ideal for patients with infective endocarditis with paravalvular abscess but it is not a substitute for radical resection

59
Homograft aortic root replacement
More technically demanding (less rigid nature of tissue) Recommended in age years Study by McGiffin showed the unacceptably high incidence of valve failure over 15 years period McGiffin/ Grinda / Lytle found improved freedom from recurrent endocarditis compared with prosthetic material
 Recommended in age years. Study by McGiffin showed the unacceptably high incidence of valve failure over 15 years period. McGiffin/ Grinda / Lytle found improved freedom from recurrent endocarditis compared with prosthetic material.")
60
Pulmonary autograft

61
AVR with Pulmonary Autograft TGH Experience (1990-2003)
213 patients 66% men Mean age: 34 years (16 – 63 years) AV pathology: 82% - bicuspid/congenital 5% - prosthetic dysfunction 2% - rheumatic 10% - miscellaneous
 AV pathology: 82% - bicuspid/congenital. 5% - prosthetic dysfunction. 2% - rheumatic. 10% - miscellaneous.")
62
AVR with Pulmonary Autograft
AV lesion: AS % AI % AS+AI % Follow-up: 6.1±3.4 years; 100% complete Annual echocardiographic studies Annual visit to cardiologist and/or valve clinic

63
AVR with Pulmonary Autograft Operative Outcome
One operative death: AMI 2 late deaths: 1 accident, 1 suicide 11 patients had reoperations: (no death) 2 – false aneurysms (valve saved) 5 – aortic insufficiency (valve replaced) 2 – pulmonary homograft stenosis 2 – coronary artery bypass 17 patients developed moderate or severe AI 182 (85%) – free of any adverse event
 2 – false aneurysms (valve saved) 5 – aortic insufficiency (valve replaced) 2 – pulmonary homograft stenosis. 2 – coronary artery bypass. 17 patients developed moderate or severe AI. 182 (85%) – free of any adverse event.")
64
AVR with Pulmonary Autograft Survival and Freedom from Any Reoperation
12-year: Survival = 98% Reop Free = 87% Pts at risk

65
AVR with Pulmonary Autograft Freedom from Aortic Insufficiency
12 yr = 88±4% 3+ AI = 12 patients 4+ AI = 5 patients 13/17 due to dilation Pts at risk

66
AVR with Pulmonary Autograft Predictors of Moderate or Severe AI
Incompetent bicuspid aortic valve Odds ratio: 3.6 Mismatch between aortic and pulmonary annuli >4 mm Odds ratio: 2.9 Incompetent bicuspid aortic valve + mismatch Odds ratio: 8.5

67
AVR with Pulmonary Autograft Freedom from Moderate or Severe PI ± >40mmHg PS
12-yr = 86±4% Age 34 years = 72% Age > 34 years = 100% Pts at risk

68
AVR with Pulmonary Autograft Predictors of Pulmonary Valve Homograft Dysfunction
Patients’ age (by 5 years reductions) Odds ratio 1.6 10 year freedom from PV dysfunction: <20 yr-old = 62%±8% 20-30 yr-old = 85%±5% >30 yr-old = 95%±2%
 Odds ratio year freedom from PV dysfunction: <20 yr-old = 62%±8% yr-old = 85%±5% >30 yr-old = 95%±2%")
70
Result

71
Factor for late AI Male Aortic/ pulmonic annular mismatch
Aortic annulus >= 27mm Preoperative AI Female, Aortic stenosis, annulus <27 mm got best outcome Not recommended in bicuspid aortic valve, marfan syndrome, connective tissue disease

72
Ross Procedure Very demanding technically
80 % freedom from reoperation at 20 years Promise for IE David found dilatation of neoaortic valve in bicuspid aortic valve disease Reserve for young patients who are not predisposed to aortic or pulmonary artery dilatation

73
Conclusions Pulmonary Autograft
AVR with pulmonary autograft is probably the ideal valve for young adults who are physically active and have aortic stenosis Pulmonary autograft should be avoided in patients with mismatch between the aortic and pulmonary annuli by more than 4 mm and/or an incompetent bicuspid aortic valve

74
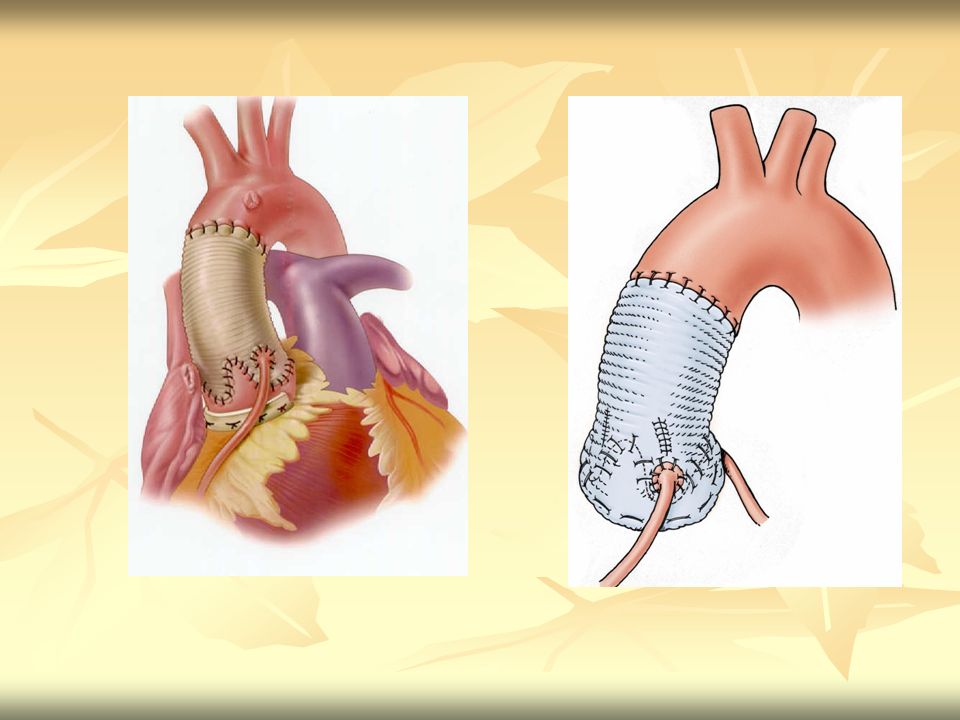
Composite valve graft Used in abnormal aortic cusp and dilated aortic root Results varied as the indication of surgery (aortic dissection less than aneurysm) Mortality 5-10% Freedom from TE93% Freedom from endocarditis 90% Freedom from reoperation 74%
 Mortality 5-10% Freedom from TE93% Freedom from endocarditis 90% Freedom from reoperation 74%")
75
CVG with tissue valve

77
Results of CVG Low operative MR (4-10%)
Excellent long term survival (10 year survival 60%) Freedom from TE, Endocarditis and Reoperation is good
 Freedom from TE, Endocarditis and Reoperation is good.")
78
Aortic valve sparing 30 % of Aortic root replacement has normal aortic valve Two technique: Remodeling (Yacoub) Reimplantation (David) (Less AI, good hemostasis, less reoperation, redo for AVR easier)
 (Less AI, good hemostasis, less reoperation, redo for AVR easier)")
79
Aortic valve sparing Indication are expanding to bicuspid aortic valve and type A dissection Result (freedom from reoperation) is excellent
 is excellent.")
80
Remodeling (Yacoub technique)
")
81
Reimplantation (David technique)
MR 0.6% 15 year survival 87.8% 15yrFreedom from AI 79.2%

83
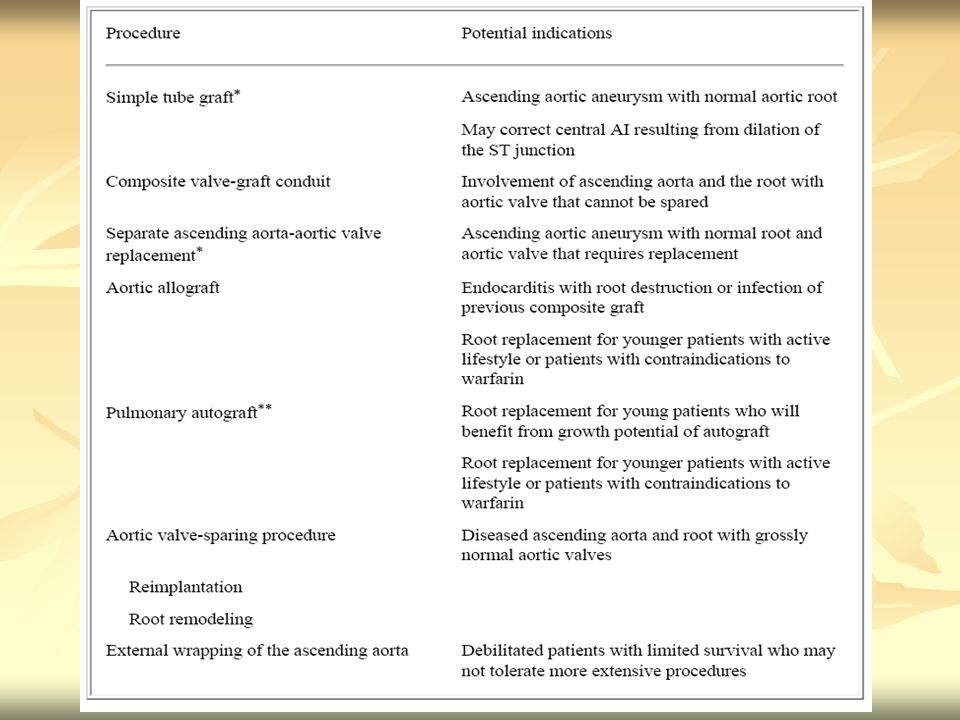
Aortic Root Replacement
Aortic Regurgitation Congestive Heart Failure Prominent Ascending Aortic Shadow History Physical Examination Chest x-ray Echocardiogram CT/MRI A B Aortic Root Pathology Mild-moderate AI Size<5.0 cm Severe AI Size > 5.0 cm Medical therapy And follow-up C Aortic Root Replacement D Age < 40 Age 40-60 F Age > 60 G Extensive or Prosthetic Valve Endocarditis Acute Type A Aortic Dissection E Aorta not dilated Aorta dilated Ross Procedure Aortic valve diseased Aortic valve not diseased Homograft Root H Aortic valve not diseased Aortic valve diseased Aortic valve not diseased Aortic valve diseased Mechanical or Tissue CVG Homograft Root Xenograft Root Valve-Sparing Root Replacement Aortic valve diseased Aortic valve not diseased I Mechanical CVG Xenograft Root Valve-Sparing Root Replacement Valve-Sparing Root Replacement Mechaical or Tissue CVG Separate Valve-Graft Valve-Sparing Root Replacement Tissue CVG Xenograft Root John S. Ikonomidis, Aortic root replacement, in cardiac surgery

85
Conclusion Type of surgery: depends on
Patient condition Age, comorbidity, condition of native aortic valve, pulmonic valve, limitation of anticoagulant usage postop Valve preference in each patient Surgeon (experience, skillful)
")
86
Case 1 Case ผู้หญิงไทย อายุ 25 ปี underlying Marfan’s syndrome, married, want to pregnant CXR:Dilatation of ascending aorta Echo/TEE: severe AR ,EF 70%,no RWMA, dilated aortic root at sinus part of aorta 5.05 cm, LVOT 2.4 cm, Ascending aortic dilate 5.6 cm indiameter

87
Operation ? Tissue Valve/ Homograft Replacement
Mechanical Valve Replacement Composite valve graft (Bentall operation) Ross Operation Aortic valve sparing
 Ross Operation. Aortic valve sparing.")
88
Case 2 Case ผู้หญิงไทย อายุ 22 ปี
DX severe AS (อายุ 19 ปี ) s/p AV commissurotomy หลังทำ3 months มีเหนื่อย ประมาณ 1-2 เดือน หลังจากคลอดบุตรคนแรกผู้ป่วยเหนื่อยมากขึ้น ตรวจพบว่ามี severe AR, ผู้ป่วยมาปรึกษาแพทย์ว่าถ้าหลังจากการผ่าตัดแล้ว ผู้ป่วยยังอยากที่จะมีบุตรต่อ
 s/p AV commissurotomy หลังทำ3 months มีเหนื่อย. ประมาณ 1-2 เดือน หลังจากคลอดบุตรคนแรกผู้ป่วยเหนื่อยมากขึ้น ตรวจพบว่ามี severe AR, ผู้ป่วยมาปรึกษาแพทย์ว่าถ้าหลังจากการผ่าตัดแล้ว ผู้ป่วยยังอยากที่จะมีบุตรต่อ.")
89
Case 2 Echo: EF 62%, Severe AR (regurgitation flow 1114 ms., PHT 323 ms.), tricuspid and torn leaflet, no calcification
, tricuspid and torn leaflet, no calcification.")
90
Operation ? Tissue Valve/ Homograft Replacement
Mechanical Valve Replacement Composite valve graft (Bentall operation) Ross Operation Aortic valve sparing
 Ross Operation. Aortic valve sparing.")
91
Case 3 Case ผู้ชายไทยอายุ 21 ปี severe AR ผู้ป่วยมาปรึกษาแพทย์ เรื่องการผ่าตัดว่า หลังการผ่าตัดผู้ป่วยไม่ขอ on anticoagulant Echo: EF 61%, severe AR (PHT ms.), LVEDD 65 mm, LV enlargement, Aortic annulus 2.75 cm., Pulmonic valve cm., Aortic Valve are trileaflets, retracted and rolling.
, LVEDD 65 mm, LV enlargement, Aortic annulus 2.75 cm., Pulmonic valve cm., Aortic Valve are trileaflets, retracted and rolling.")
92
Operation ? Tissue Valve/ Homograft Replacement
Mechanical Valve Replacement Composite valve graft (Bentall operation) Ross Operation Aortic valve sparing
 Ross Operation. Aortic valve sparing.")
93
Case 4 Case ผู้ชายไทย อายุ 24 ปี มาด้วย ไข้ เหนื่อย
Dx:BE with severe AR, รักษาได้ ATB ครบ 6 wk คลำได้ก้อนที่บริเวณก้นด้านซ้าย(AVM at left buttock) Echo:Severe AR, EF 60%, Aortic root 28.8 mm, sinotubular junction 28 mm, aortic root 24.8 mm, tricuspid AV, vegetation size 14x9.9 mm attached to left cusp involve to septum, pulmonic valve 24. mm
 Echo:Severe AR, EF 60%, Aortic root 28.8 mm, sinotubular junction 28 mm, aortic root 24.8 mm, tricuspid AV, vegetation size 14x9.9 mm attached to left cusp involve to septum, pulmonic valve 24. mm.")
94
Operation ? Tissue Valve/ Homograft Replacement
Mechanical Valve Replacement Composite valve graft (Bentall operation) Ross Operation Aortic valve sparing
 Ross Operation. Aortic valve sparing.")
95
Case 5 Case ผู้ชายไทย อายุ 40 ปี มาด้วยเหนื่อยมากขึ้นขณะสอนหนังสือ
CXR: Dilatation of of ascending aorta CTA: Aortic aneurysm at ascending aorta size 6.2 cm in diameter. Echo: moderate AR, EF 48%, ascending aortic aneurysm 6 cm in diameter, no evidence of ascending aortic dissection, LVOT 4.2 cm, STJ 5.2 cm, tubular diameter 4.2 cm, AV 3 leaflets, no MR/MS

96
Operation ? Tissue Valve/ Homograft Replacement
Mechanical Valve Replacement Composite valve graft (Bentall operation) Ross Operation Aortic valve sparing
 Ross Operation. Aortic valve sparing.")
97
Case 6 female 59 years old, chest pain FC III
CXR: Dilatation of of ascending aorta Echo: moderate AR, EF 39%, ascending aortic aneurysm 5 cm in diameter, no evidence of ascending aortic dissection, sinus valsava 6 cm, AV 3 leaflets rolling and retracted of leaflets, mild MR

98
Operation ? Tissue Valve/ Homograft Replacement
Mechanical Valve Replacement Composite valve graft with tissue valve (Bentall operation) Ross Operation Aortic valve sparing
 Ross Operation. Aortic valve sparing.")
Similar presentations

















 Ross operations in 62 consecutive pediatric patients Alejandra Bueno MD, David Zurakowski.>")


