Download presentation
Presentation is loading. Please wait.

1
ALLOGRAFT VALVE SURGERY P.Skillington CANBERRA April 2003

2
Aortic Valve Replacement Aetiology of Valvular Disease Pathology encountered Operations Available: focus on Allograft Operative Techniques Results

3
Aortic Valve - Aetiology Congenital: bicuspid, monocuspid age – 0-70 (peak 35-50) Degenerative: tricuspid age - >60 (peak 70-80) Rheumatic: Post rheumatic fever, uncommon in Australia age – all ages
 Degenerative: tricuspid age - >60 (peak 70-80) Rheumatic: Post rheumatic fever, uncommon in Australia age – all ages")
4
AVR: Choice of Prosthesis Durability of Prosthesis Necessity for Warfarin- temporary or permanent Risk of Thrombo-embolism & Bleeding Re-operation rate & difficulty

5
Patient Related Factors Haemodynamic Performance: flow dynamics functional state achieved Biocompatibility Effect of various disease states eg: Marfans,other connective tissue diseases Possible future pregnancy Valve noise

6
AVR : Mechanical vs. Tissue Valve Excellent Durability 95% at 10yrs. 90% at 20yrs Low rate of re-operation. Easy to insert Warfarin, blood tests Thrombo-embolism 1-2%/pt/yr Bleeding risk 2%/pt/yr Non Cardiac Surgery hazardous Do not need warfarin Low risk of thrombo- embolism and bleeding : 0-1% Noiseless Durability variable:ie higher rate of re-operation Insertion may be more difficult Other surgery safe

7
Tissue Valve Durability Porcine,Pericardial: 40yrs:– 8-10 yrs 70yrs:- 12-15yrs Aortic Allograft: 20yrs:- 10yrs 40-70yrs:- 15yrs Ross Procedure: On average,will last 40-50yrs (variable) Re-operation rate:- 1%/pt/yr
 Re-operation rate:- 1%/pt/yr")
8
Stentless Porcine Valve AVR in elderly Better Haemodynamic function Larger orifice area Better resolution of Left Ventricular Hypertrophy

9
Aortic Allograft Insertion Human cadaveric Ao. v Cryopreserved AVR Root Replacement vs Subcoronary

10
Aortic Homograft (Allograft) Durability Better than Xenografts eg 50yr old: expect 15yr lifespan (vs 10 yrs ) Other Advantages Endocarditis with aortic root abcess Warfarin not required Disadvantages Not on shelf Re-operation difficult
 Durability Better than Xenografts eg 50yr old: expect 15yr lifespan (vs 10 yrs ) Other Advantages Endocarditis with aortic root abcess Warfarin not required Disadvantages Not on shelf Re-operation difficult")
11
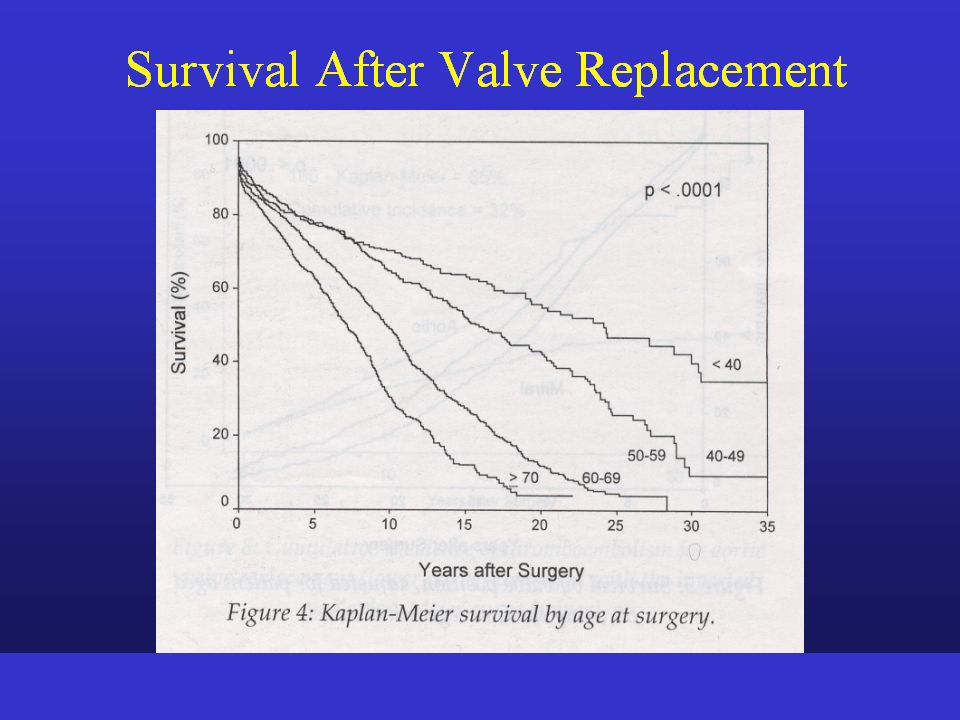
M.O’Brien et al “The Homograft Aortic Valve:29 yrs” J. Heart V. Dis 2001;10:334-345 1,022 patients mean age 47yrs: Actuarial Survival

12
O’Brien et al,2001 Aortic Homograft Durability vs Age: Freedom from Re-op

13
Summary – Allograft AVR Best age range: 30 – 65 yrs Durability in that age range: 15yrs avge Indications: Endocarditis Not suitable for Ross Proc. Results: 78 pts over 12 yrs (1990-2002) Early Mortality: 0 Late re-operation: 3
 Early Mortality: 0 Late re-operation: 3.")
14
Ross Procedure Advantages Viable aortic valve Improved Durability cf other tissue valves No Warfarin absence T/E, ARH Disadvantages Longer operation Follow up of pulmonary valve

15
Ross Procedure Indications Age 20-60yrs, requiring AVR Contra-indications Bicuspid pulmonary valve(echo) Marfans Syndrome Other connective tissue disease R.arthritis/ SLE Active rheumatic heart disease Triple vessel CAD/ Mitral v. dis.

16
Patient Demographics (Ross P.) Time Frame : October 1992 to February 2003 No. of Patients: 172 1. Age:Range 16-62 (Mean 39.3) 2. :GenderM = 122 (70.9%)F = 50 (29.1%) 3. Valve Lesion: Aortic Stenosis: 68 (40%) AS/AR(Mixed): 51 (29%) Aortic Regurg: 53 (31%) 4. Aortic Valve Aetiology: Congenital: 158 (92%) Other:14 (8%) 5. Re-operation:19 (11%)
 2. :GenderM = 122 (70.9%)F = 50 (29.1%) 3. Valve Lesion: Aortic Stenosis: 68 (40%) AS/AR(Mixed): 51 (29%) Aortic Regurg: 53 (31%) 4. Aortic Valve Aetiology: Congenital: 158 (92%) Other:14 (8%) 5. Re-operation:19 (11%).")
17
Microsoft Excel Spreadsheet – May 2002

18
MORTALITY & MORBIDITY 1. Early Mortality(in hosp. Or within 30 days)1 (0.6%) Myocardial Infarct 2. Early Morbidity - Re-Exploration9 (a) Bleeding7 (4.1%) (b) Graft RCA.1 ( c ) Low C.O. 1 - Retinal Embolus1 - CHB >>> Pacemaker1 - Renal Impairment4 - AMI2 - Inotropes3 - IABP1 - Respiratory Failure (Re-Intubation)1 - Pericardial Effusion1 - Arrhythmia Ventricular2 Atrial (AF) 20 -Sternal Infection 1 N=172
1 (0.6%) Myocardial Infarct 2. Early Morbidity - Re-Exploration9 (a) Bleeding7 (4.1%) (b) Graft RCA.1 ( c ) Low C.O. 1 - Retinal Embolus1 - CHB >>> Pacemaker1 - Renal Impairment4 - AMI2 - Inotropes3 - IABP1 - Respiratory Failure (Re-Intubation)1 - Pericardial Effusion1 - Arrhythmia Ventricular2 Atrial (AF) 20 -Sternal Infection 1 N=172.")
19
Late Results (n = 172) Late Death (non-cardiac) 2 1.2% Follow up 98.6% complete 735 patient years Thrombo-embolism 1 Cumulative Inc. 0.1% Bleeding(ARH) 0 0.0% Endocarditis 0 0.0% Re-operation 6 0.8% Late AR>mild 0 0.0% * 5yr freedom from re-operation = 96.2%
 0 0.0% Endocarditis 0 0.0% Re-operation 6 0.8% Late AR>mild 0 0.0% * 5yr freedom from re-operation = 96.2%.")
20
Ross (inclusion cylinder) Actuarial Survival: 155 patients 5yrs = 98% 7yrs = 95% 155 127 101 83 54 37 19 7 4
 Actuarial Survival: 155 patients 5yrs = 98% 7yrs = 95%")
21
(n=155) 5yrs = 99% 7yrs = 99% 155 127 101 83 54 37 19 7
 5yrs = 99% 7yrs = 99%")
22
Zellner et al “Long term experience With the St.Jude Medical Valve Prosthesis” South Carolina,USA AVR 418 pts, mean age 54.8yrs Re-operation inc. 1.0%/pt/y *10yr survival 58%

23
Pregnancy after the Ross Procedure Seven women have under gone 11 successful pregnancies No maternal cardiac complications No problems with the passengers Favourable in contrast with mechanical valves

24
Durability Aortic Valve Prostheses

26
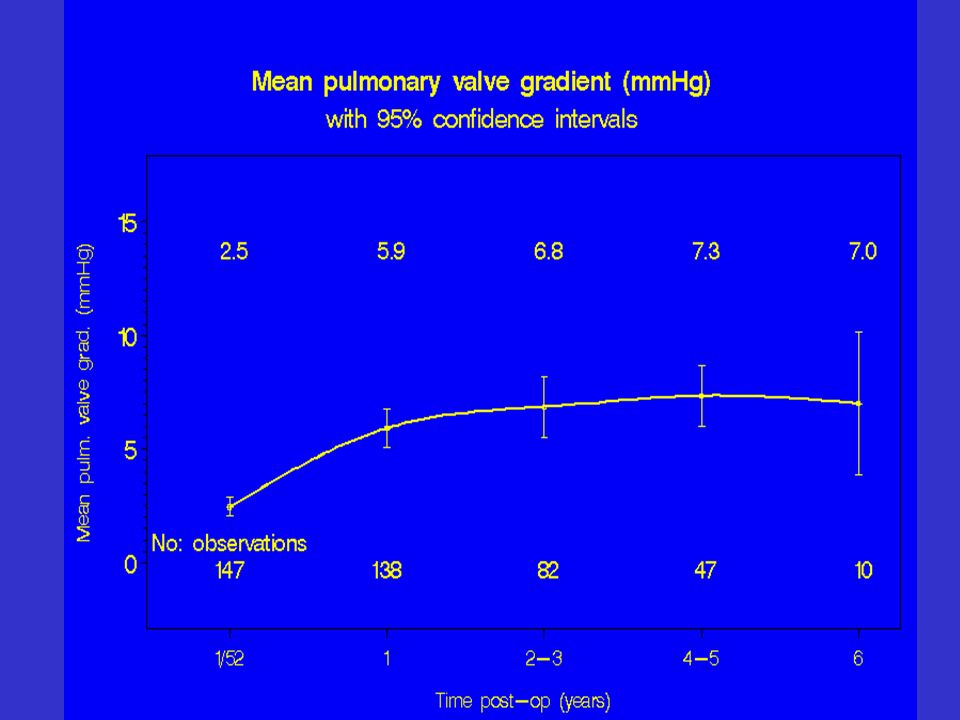
Pulmonary Regurgitation

28
AVR - Choice Prosthesis-Effect of Age 15-60 yrs Ross, Mechanical, Allograft 60-70 yrs Mechanical, Allograft, Porcine/Pericardial >70 yrs Stentless Porcine,Stented Pericardial, Mechanical

29
Results Pulmonary Allograft Insertion for Tetralogy, other Congenital Cardiac 45 patients over 12 year period zero mortality, minimal complications Beating heart surgery Do not require warfarin Quality of life very good

30
Conclusion 300 patients have had cardiac allograft valve replacement: Ross Procedure 177 Aortic Allograft 78 Pulmonary Allograft 45 Safe surgery: one(1) early death Excellent quality of life without anti- coagulants : young people
 early death Excellent quality of life without anti- coagulants : young people")
31
Standard Post-op Management Early BP(sys, mean) ; filling pressures (R+L) C. Output – depends on temperature Low CO (>37 C) Pericardial Tamponade signs of tamponade : low bp,high cvp,low urine output (usually prior bleeding) Improve CO optimal filling (+ve balance 1-2 l) vasodilators (GTN, prop., nipride) inotropes (milrinone, NOT adr,dop) noradrenaline IABP rate(80-90),rhythm
 Pericardial Tamponade signs of tamponade : low bp,high cvp,low urine output (usually prior bleeding) Improve CO optimal filling (+ve balance 1-2 l) vasodilators (GTN, prop., nipride) inotropes (milrinone, NOT adr,dop) noradrenaline IABP rate(80-90),rhythm.")
32
ANTICOAGULATION AVR mechanical : INR, Time to reach 2.0 pacing wire removal day 3-4 if not required porcine / pericardial : warfarin 6 weeks Ross / Allograft : aspirin 3months MVR mechanical INR 3.0,if chr.AF, clexane after 3-4 days porcine / pericardial Warfarin at least 3 months, often permanent MV Repair Warfarin 3 months

33
Special Situations Mitral valve surgery /PHT : pul vaso-dil,extub, sw ganz, LA line,b. gases, pht crisis AVR for AS and severe LVH AVR thin walled aorta – sys BP Ross : Sw Ganz removal Patients with poor LV sys function :early IABP TVR : pacing, cvp only for Repl. PVR : Usually no PA catheter

34
Stentless Tissue Valves Examples include: stentless porcine valve Aortic Allograft (homograft) Ross Proc. (pul.autograft) Features: Better haemodynamic funct. Improved resolution of left ventricular hypertrophy
 Features: Better haemodynamic funct. Improved resolution of left ventricular hypertrophy.")
35
Haemodynamic Function Ross (pulmonary autograft) 2-4 Stentless Porcine 5 Aortic Allograft 6 Mechanical 10-20 Stented Porcine/Pericardial 12-25 Residual aortic valve gradient(mmHg) *gradients at rest
 2-4 Stentless Porcine 5 Aortic Allograft 6 Mechanical Stented Porcine/Pericardial Residual aortic valve gradient(mmHg) *gradients at rest")
37
MITRAL VALVE - Aetiology Myxoid Degeneration – 75% Repair Rheumatic – 95% Replacement Ischaemic – 50% Repair, 50% Replace Other – Endocarditis, SLE, Chordal Rupture

38
Actuarial Survival 132 107 86 65 41 22 No.Patients 5 yr. 5 5yr. 97.5% 5yr.Cardiac Related 98.7%

39
AVR - Mortality Depends on age,cor.dis.,LV function 80 3-5%

40
Conclusions Early Mortality for AVR very low – all ages Tissue Valves favoured where possible,especially in the elderly,to avoid warfarin related problems & T- embolism If Tissue Valve used, Stentless valve is better haemodynamically In the elderly, patient will usually outlive their valve In younger patients, Ross Proc. is safe, good quality of life, low risk re-operation

41
ALREADY SHOWN Low Operative Mortality and Morbidity Resolution LVH Normalization LV Size and Function AIMS Late Valve Related Events Aortic Valve Function and Need For Re-Operation

42
AORTIC VALVE FAILURE A.R. Re-operation Moderate Aortic Regurgitation or Greater Factors Analyzed Age Sex Aortic Valve Lesion : AS/AR/Mixed Aortic Annulus Diameter Aortic Annulus Reduction Method Implantation of Autograft

43
TORONTO SPV CLINICAL SERIES June 1994 – May 2001 90 Patients Mean Age 75.5 years (61-87) Sex:Male53.3% (48) Female46.7% (42)
 Sex:Male53.3% (48) Female46.7% (42)")
46
Results Stentless Valve Insertion Early Mortality Re-operation Hospital <30 days Total (%/pt/yr) Ross Proc. 143 0 1 1(0.7%) 0.9 TSPV 90 1 1 2(2.2%) 0 Aortic Allo. 35 0 0 0 1.5
 0.9 TSPV (2.2%) 0 Aortic Allo")
47
Aortic Allograft :- Indications Endocarditis : Lowest risk of recurrent infection Exclusion of abcess cavities Women of child bearing age <60 yrs:-Unsuitable for Ross Procedure 60-70yrs:-Unsuitable for Mechanical device

48
Cardiac Surgery Modern Surgical specialty 1953: Development of the heart/lung machine (cardiopulmonary bypass) allowed intracardiac procedures to be performed on the empty heart Later improvements (cardioplegia) led to Asystolic arrest– flaccid or still heart 1960: Cardiac Valve Replacement 1968: Coronary Artery Bypass Surgery
 allowed intracardiac procedures to be performed on the empty heart Later improvements (cardioplegia) led to Asystolic arrest– flaccid or still heart 1960: Cardiac Valve Replacement 1968: Coronary Artery Bypass Surgery")
Similar presentations