Download presentation
Presentation is loading. Please wait.

1
What is the role of neighbourhoods in understanding spatial concentrations of health and ill health? Jamie Pearce Centre for Research on Environment, Society and Health (CRESH) Institute of Geography, School of GeoSciences University of Edinburgh jamie.pearce@ed.ac.uk www.cresh.org.uk
 Institute of Geography, School of GeoSciences University of Edinburgh")
2
Overview 1. Is poor health increasingly concentrated in socially disadvantaged neighbourhoods? 2. Do socially disadvantaged neighbourhoods also experience lower quality (health-related) physical environments? 3. The place of neighbourhood- level policy interventions to affect health
 physical environments. 3. The place of neighbourhood- level policy interventions to affect health.")
3
Health Inequalities: Mortality http://www.statistics.gov.uk/STAT BASE/Product.asp?vlnk=6638

4
Life expectancy in Glasgow Lenzie Life expectancy=82 Calton Life expectancy=54 14km apart: 28 year difference in life expectancy

5
Age standardised mortality for area deprivation category in Scotland. Rates per 100,000 men and women aged 0–64, 1980–82, 1991–92 and 2000–02 Data taken from Leyland et al. (2007) BMC Public Health Low High
 BMC Public Health Low High.")
6
Source: Pearce & Dorling. International Journal of Epidemiology 2006;35:597–603

7
Health selective migration Do ‘healthy’ or ‘unhealthy’ people have a greater or lesser propensity to move? Implications - geographical inequalities in health If sorting occurs in which: –people in better health are more likely to move to (or remain in) less deprived areas –people in poorer health are more likely move to (or remain in) more deprived areas Geographical inequalities in health will be exacerbated
 less deprived areas –people in poorer health are more likely move to (or remain in) more deprived areas Geographical inequalities in health will be exacerbated.")
8
Smoking Data Censuses: 1981, 1996 & 2006: cigarette smoking status age >15. Smoking data obtained (each respondent) classified: smoker ex-smoker never smoked District Health Boards (DHBs): n=21 av. pop. size of 194,000 range 31,000 to 489,000 Source: Pearce J, Dorling D, 2010. Annals of the Association of American Geographers 100(2), 393–408.
 classified: smoker ex-smoker never smoked District Health Boards (DHBs): n=21 av. pop. size of 194,000 range 31,000 to 489,000 Source: Pearce J, Dorling D, Annals of the Association of American Geographers 100(2), 393–408..")
9
Migration effects Demographic accounting - to ascertain the net movement of smokers into each area due to 1. 1.i) internal migration 2. 2.ii) immigration from overseas
 internal migration 2. 2.ii) immigration from overseas.")
10
Smoking migration balance Widening geographical gap in smoking behaviour (1981-2006) - only partly attributable to unequal smoking cessation rates Important component: – –differential migration patterns between regions according to their smoking status Eg net migration balance – all DHBs (1976-1981) ranged from – –2.2 % gain in never smokers in Capital and Coast (low deprivation) – –1.5 % gain in smokers in Wairarapa and in Whanganui (high poverty)
 - only partly attributable to unequal smoking cessation rates Important component: – –differential migration patterns between regions according to their smoking status Eg net migration balance – all DHBs ( ) ranged from – –2.2 % gain in never smokers in Capital and Coast (low deprivation) – –1.5 % gain in smokers in Wairarapa and in Whanganui (high poverty)")
11
Effects of International Migration Excluding immigrants had a significant effect E.g. 1/3 of Auckland’s ‘advantage’ due to selective migration of immigrants.

12
The smoking migration balance of men and women combined by DBH 1976-1981, 1991- 1996 and 2001-2006, and standard deviation Excluding immigrantsIncluding immigrants

13
Smoking migration balance and life expectancy What are effects of the selective migration patterns of smokers and non-smokers on the spatial pattern of health inequalities ? – –Clear relationship: DHB smoking migration balance and life expectancy for males in 2001 More smokers that tend to leave each area compared to the net number of non-smokers that arrive, the higher the DHB-level life expectancy. Correlation - life expectancy in 2001 & net smoking migration balance (1976- 1981) – –stronger for males (-0.67) than for females (-0.50), – –maybe because lower proportion of females smoked (particularly 1981).
 – –stronger for males (-0.67) than for females (-0.50), – –maybe because lower proportion of females smoked (particularly 1981)..")
14
Concepts of Environmental Justice Distribution Environmental Justice Recognition Participation Capabilities after Schlosberg (2007)
")
15
Pearce, Witten, Hiscock & Blakely. International Journal of Epidemiology 2007;36:348–355

16
Source: Pearce, Day & Witten. Urban Policy & Research 26: 2008; 213–27

17
Source: Pearce, Blakely, Witten & Bartie. American Journal of Preventive Medicine 2007;32:375–382 Fast food outlets

18
Source: Day & Pearce. American Journal of Preventive Medicine 2011;40(2):113–121 K Function Clustering High degree clustering around schools Up to 5.5 times more than expected Particularly socially deprived schools
:113–121 K Function Clustering High degree clustering around schools Up to 5.5 times more than expected Particularly socially deprived schools.")
19
Source: Pearce et al. Journal of Epidemiology and Community Health 2009; 63, 69-77. Tobacco outlets and smoking

20
But….

21
Source: Witten, Pearce & Day. Environment & Planning A 43: 2011; 205-23 Neighbourhood Destination Accessibility Index (NDAI): infrastructure support for neighbourhood physical activity
: infrastructure support for neighbourhood physical activity.")
22
Median travel time to 16 sub-domains of community resources in deprivation quintiles across New Zealand Source: Pearce et al. International Journal of Epidemiology 2007;36:348–355

23
Health/ behaviour effects Associations between community resource access and health in NZ neighbourhoods: Access to fast food outlets No association with BMI No association with diet (Pearce et al. Health and Place 2009; 15, 193-197) Access to supermarkets & convenience stores No association with fruit consumption No association with vegetable consumption (Pearce et al. Journal of Epidemiology and Community Health 2008; 62, 198-200) Access to green space No association with CVD (Richardson, Pearce et al. BMC Public Health 2010; 10(1):240.)
 Access to supermarkets & convenience stores No association with fruit consumption No association with vegetable consumption (Pearce et al. Journal of Epidemiology and Community Health 2008; 62, ) Access to green space No association with CVD (Richardson, Pearce et al. BMC Public Health 2010; 10(1):240.).")
24
Measure of Multiple Physical Environmental Deprivation? Multiple Environmental Deprivation Consider the social dimensions of multiple environmental risk factors: 1.Assess socio-spatial distribution of multiple dimensions of the physical environment (related to health) 2.Test the tool to assess implications for health and health inequalities
 2.Test the tool to assess implications for health and health inequalities.")
25
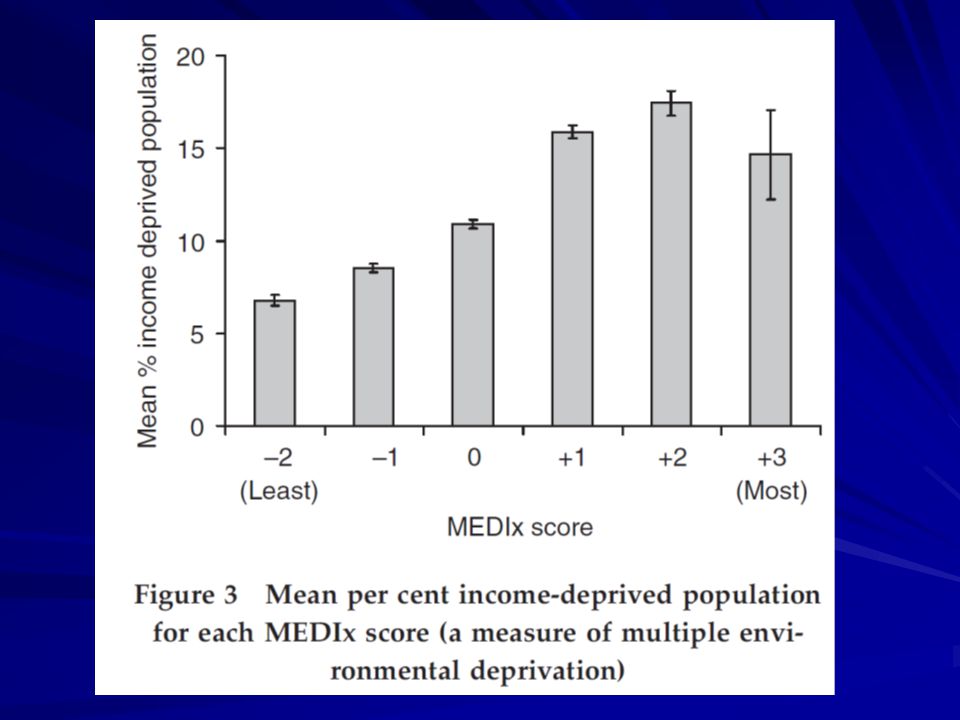
Multiple Environmental Deprivation Index (MEDIx) MEDIx score -2 = Least environmentally deprived wards (‘healthiest’ places, theoretically) MEDIx score +3 = Most environmentally deprived wards (‘unhealthiest’ places)
 MEDIx score -2 = Least environmentally deprived wards (‘healthiest’ places, theoretically) MEDIx score +3 = Most environmentally deprived wards (‘unhealthiest’ places)")
28
Standardised Mortality Ratios and confidence intervals across quintiles of socio-economic deprivation, unadjusted and adjusted for physical environmental deprivation

29
Localism in the UK May 2010 – Coalition Government (Conservative/Liberal Democrats) Implementing radical agenda –Budget cuts –Central government spend –Local government spend –Greatest cuts – most disadvantaged groups/ places Implications include: –Increase Value Added Tax (VAT) –Removing ‘Education Maintenance Allowance’ –Tripling student fees –Welfare –National Health Service restructuring Wholesale redefinition of the relationship between the individual and the state…?
 Implementing radical agenda –Budget cuts –Central government spend –Local government spend –Greatest cuts – most disadvantaged groups/ places Implications include: –Increase Value Added Tax (VAT) –Removing ‘Education Maintenance Allowance’ –Tripling student fees –Welfare –National Health Service restructuring Wholesale redefinition of the relationship between the individual and the state…")
30
Localism Agenda ‘Big Society’: –transfer of power & rights from centre to local –Increase role for community groups and third sector organisations – delivery of services –do things for yourself rather than the state Localism Bill: –Placing power at the heart of local communities? –Reinforce local democracy? –Devolving responsibility? Implications include: –return funds from business rates to councils that earn them rather than distribute according to need –removal of national housing targets Localism the shield for a sizeable redistribution from poor to rich?

31
Deficit reduction & localism Socio-ecological perspective: –Social distribution in health - underlain by unequal distribution of resources fundamental to a healthful life –Wealth, education, employment, access to health care, environment (physical, social, built etc) in which people live…. Fundamental implications for SDOH? –rise in social & economic inequalities –welfare support –food security –housing –migration –etc Local environment (neighbourhoods) –increasingly pertinent – public health/ health inequalities?
 –increasingly pertinent – public health/ health inequalities .")
32
Conclusion Increasing concentration of poor health in more disadvantaged neighbourhoods –Selective migration/mobility part of the story Socially disadvantaged neighbourhoods also experience lower quality (health-related) physical environments? –Triple jeopardy? –UK evidence supportive Mixed evidence from neighbourhoods in NZ –Questions some aspects of the neo-material understanding of health inequalities Public health perspective on ‘Big Society’ –Localism agenda – –Building community resilience and devolving local services? – –Or putting a sticking plaster over the wound caused by macro- structural inequalities in power and resources? –Challenge to efforts to reduce health inequalities?

33
Acknowledgements New Zealand work funded by the NZ Health Research Council –Tony Blakely (University of Otago) –Karen Witten (Massey University) MEDIx work funded by the NERC-led Environment & Human Health Program –Richard Mitchell (University of Glasgow) –Niamh Shortt (University of Edinburgh) –Elizabeth Richardson (University of Edinburgh)
 –Karen Witten (Massey University) MEDIx work funded by the NERC-led Environment & Human Health Program –Richard Mitchell (University of Glasgow) –Niamh Shortt (University of Edinburgh) –Elizabeth Richardson (University of Edinburgh)")
Similar presentations












>")
>")
 workshop, Harrogate, UK, 28-29 September 2012 Exploring equity issues in transport and communication networks Paulo Rui Anciaes.>")





