Download presentation
Presentation is loading. Please wait.

1
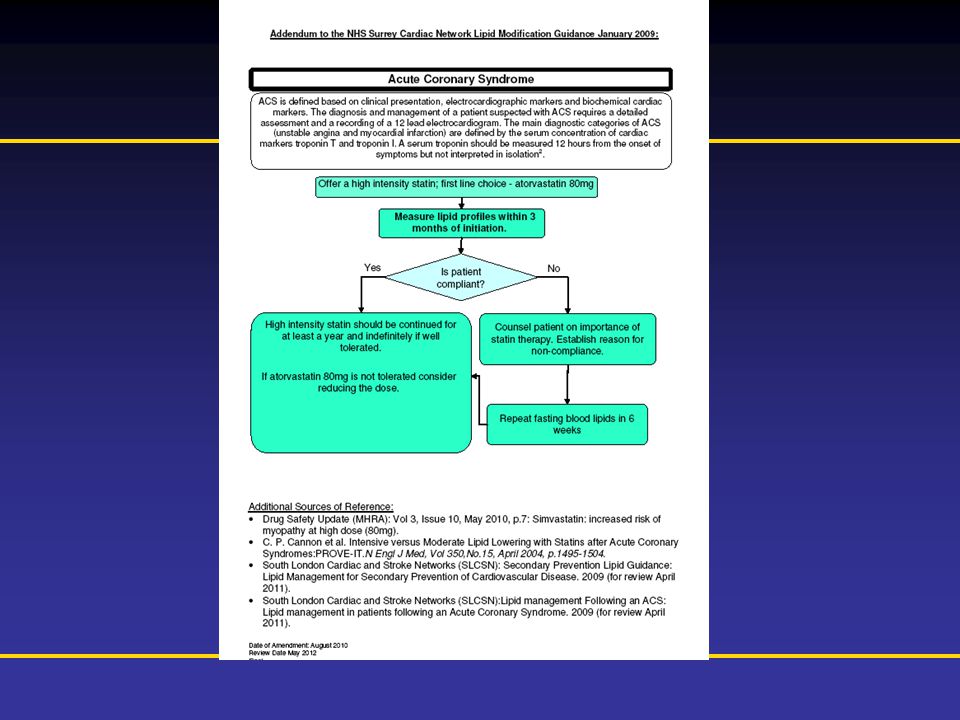
Prescribing Information is available at the end of this presentation NHS Surrey Lipid Guidelines Dr Adam Jacques adamjacques@doctors.org.uk Ashford & St Peter’s Hospital NHS Foundation Trust

2
Prescribing Information is available at the end of this presentation

5
The Evidence for Intensive Statin Therapy

6
Prescribing Information is available at the end of this presentation Myocardial Ischaemia Reduction with Aggressive Cholesterol Lowering ( MIRACL) Schwartz GG et al. JAMA 2001; 285 (13): 1711-1718
:")
7
Prescribing Information is available at the end of this presentation MIRACL Effects of early-initiated atorvastatin 80 mg after an acute coronary syndrome on death and recurrent ischaemic events Multicentre, randomised, double-blind, placebo- controlled trial Patients were assigned to atorvastatin 80 mg or placebo 24–96 hours after hospital admission for ACS Schwartz GG et al. JAMA 2001; 285 (13): 1711-1718
:")
8
Prescribing Information is available at the end of this presentation Atorvastatin 14.8% 16% RRR HR 0.84 (0.70-0.99) P=0.048 Placebo 17.4% 0 5 10 15 0481216 Time since randomisation (weeks) Cumulative incidence (%) Primary endpoint* * Primary endpoint=death, non-fatal acute MI, cardiac arrest with resuscitation, or recurrent symptomatic myocardial ischaemia with objective evidence and requiring emergency rehospitalisation Adapted from Schwartz GG et al. JAMA 2001; 285 (13): 1711-1718 16% Relative Risk Reduction
: % Relative Risk Reduction.")
9
Prescribing Information is available at the end of this presentation Safety Placebo (n=1,548) Atorvastatin (n=1,538) P value Any serious adverse event < 1% - Elevated liver transaminases (>3 x ULN) 0.6%2.5%P< 0.001 Myositis0% - Adapted from Schwartz GG et al. JAMA 2001; 285 (13): 1711-1718
:")
10
Prescribing Information is available at the end of this presentation Conclusions In stable CHD patients with ACS, early lipid-lowering therapy with atorvastatin (80 mg/day) reduces the risk of: –Early recurrent ischaemic events, primarily recurrent symptomatic ischaemia requiring rehospitalisation –Non-fatal or fatal stroke Schwartz GG et al. JAMA 2001; 285 (13): 1711-1718
:")
11
Prescribing Information is available at the end of this presentation The PRavastatin Or AtorVastatin Evaluation and Infection Therapy– Thrombolysis In Myocardial Infarction 22 (PROVE IT: TIMI 22) Cannon CP et al. NEJM 2004; 350 (15): 1495-1504
:")
12
Prescribing Information is available at the end of this presentation PROVE IT: TIMI 22 Intensive versus moderate lipid-lowering with statins after ACS Atorvastatin 80 mg vs pravastatin 40 mg (lowering LDL-C to <1.60 mmol/L vs <2.46 mmol/L, respectively) Randomised, double-blind, double-dummy non-inferiority trial Follow-up: mean 24 months Cannon CP et al. NEJM 2004; 350:1495-1504

13
Prescribing Information is available at the end of this presentation Endpoints Primary Endpoint: Composite of death from any cause, MI, documented unstable angina requiring hospitalisation, revascularisation* and stroke Secondary Endpoints: Risk of death from CHD, non-fatal MI, or revascularisation*, risk of death from CHD or non-fatal MI, and the risk of the individual components of the primary endpoint * If performed at least 30 days after randomisation Cannon CP et al. NEJM 2004; 350:1495-1504

14
Prescribing Information is available at the end of this presentation Median LDL-C levels during the study Pravastatin 40 mg Atorvastatin 80 mg 49% 21% Median LDL-C achieved Pravastatin: 2.5 mmol/L Atorvastatin: 1.6 mmol/L (P<0.001) LDL-C (mmol/L) Time of visit Adapted from Cannon CP et al. NEJM 2004; 350:1495-1504

15
Prescribing Information is available at the end of this presentation Primary endpoint: Incidence of all- cause mortality or major CV event* Adapted from Cannon CP et al. NEJM 2004; 350:1495-1504 * Major CV events included: MI, documented unstable angina requiring hospitalisation, revascularisation with either PCI or CABG (if performed at least 30 days after randomisation), and stroke 0 318212427 30 691215 % with event Months of follow-up Pravastatin 40 mg (event rate 26.3%) Atorvastatin 80mg (event rate 22.4%) 16% RRR HR 0.84 (0.74-0.95) P=0.005 30 25 20 15 10 5 0 16% Relative Risk Reduction
, and stroke % with event Months of follow-up Pravastatin 40 mg (event rate 26.3%) Atorvastatin 80mg (event rate 22.4%) 16% RRR HR 0.84 ( ) P= % Relative Risk Reduction.")
16
Prescribing Information is available at the end of this presentation Early benefits* Adapted from Ray KK et al. J Am Coll Cardiol 2005; 46:1405-1410 051015202530 0 1 2 3 4 5 Pravastatin 40 mg 4.2 % Atorvastatin 80 mg 3.0 % 28% RRR HR 0.72 (0.52-0.99) P=0.046 Days following randomisation % of patients with death, MI or rehospitalisation for ACS *Early phase = first 30 days 28% Relative Risk Reduction Different endpoint used - Triple composite of: Death, MI, or rehospitalisation for recurrent ACS
 P=0.046 Days following randomisation % of patients with death, MI or rehospitalisation for ACS *Early phase = first 30 days 28% Relative Risk Reduction Different endpoint used - Triple composite of: Death, MI, or rehospitalisation for recurrent ACS.")
17
Prescribing Information is available at the end of this presentation Late benefits* % of patients with death, MI or rehospitalisation for ACS **Analysis excluding patients with events in the first 6 months 0 2 4 6 8 10 12 Pravastatin 40 mg 13.1% Atorvastatin 80 mg 9.6% 28% RRR HR 0.72 (0.58-0.89) P=0.003 Months following randomisation 2461218 *Late Phase = 6 months–2 years** Adapted from Ray KK et al. J Am Coll Cardiol 2005; 46:1405-1410 28% Relative Risk Reduction Different endpoint used - Triple composite of: Death, MI, or rehospitalisation for recurrent ACS

18
Prescribing Information is available at the end of this presentation Safety Atorvastatin 80mg (n=2,099) Pravastatin 40mg (n=2,063) P value Discontinuation for AE, patient preference or other reasons 30.4%33.0%0.11 Discontinuation for myalgia/CK elevation 3.3%2.7%0.23 Rhabdomyolysis 0% N/A ALT ≥3 ULN 3.3%1.1%<0.001 Dose halving due to side effects or raised LFTs 1.9%1.4%0.20 Adapted from Cannon CP et al. NEJM 2004; 350:1495-1504

19
Prescribing Information is available at the end of this presentation Summary In patients hospitalised within 10 days of an acute coronary event: –‘Intensive’ lipid-lowering with 80 mg atorvastatin to a median LDL-C of 1.6 mmol/L was associated with a significant reduction in the risk of combined all-cause mortality and major CV events by 16% compared to ‘moderate’ lipid- lowering therapy with 40 mg pravastatin which achieved a median LDL-C of 2.5 mmol/L (P=0.005) –Benefits emerged within 30 days of randomisation with continued divergence of the event curves over time Cannon CP et al. NEJM 2004; 350:1495-1504

20
Prescribing Information is available at the end of this presentation The Treating to New Targets Study (TNT) LaRosa JC et al. N Engl J Med 2005; 352 (14): 1425-1435
:")
21
Prescribing Information is available at the end of this presentation TNT Intensive lipid-lowering with atorvastatin in patients with stable coronary disease Mean LDL-C of 2 mmol/L with atorvastatin 80 mg vs mean LDL-C of 2.6 mmol/L with atorvastatin 10 mg Multicentre, randomised, double-blind trial Follow-up: median 4.9 years LaRosa JC et al. N Eng J Med 2005; 352: 1425-1435

22
Prescribing Information is available at the end of this presentation Endpoints Primary endpoints Major CV event –CHD death –Non-fatal, non-procedure-related MI –Resuscitated cardiac arrest –Fatal or non-fatal stroke LaRosa JC et al. N Eng J Med 2005; 352: 1425-1435

23
Prescribing Information is available at the end of this presentation Lipid results Adapted from LaRosa JC et al. N Eng J Med 2005; 352: 1425-1435 Study visit (months) 0 20 40 60 80 100 120 140 160 Mean LDL-C (mg/dL) Atorvastatin 80 mg (n=4995) Atorvastatin 10 mg (n=5006) FinalScreen031212 2424 3636 4848 6060 P<0.001 Baseline Mean LDL-C level = 101 mg/dL (2.6 mmol/L) Mean LDL-C level = 77 mg/dL (2.0 mmol/L) 4.0 3.5 3.0 2.5 2.0 1.5 1.0 0.5 0 Mean LDL-C (mmol/L)
 Mean LDL-C (mg/dL) Atorvastatin 80 mg (n=4995) Atorvastatin 10 mg (n=5006) FinalScreen P<0.001 Baseline Mean LDL-C level = 101 mg/dL (2.6 mmol/L) Mean LDL-C level = 77 mg/dL (2.0 mmol/L) Mean LDL-C (mmol/L).")
24
Prescribing Information is available at the end of this presentation Primary endpoint: Major cardiovascular events* *CHD death, non-fatal non–procedure-related MI, resuscitated cardiac arrest, fatal or non-fatal stroke Adapted from LaRosa JC et al. N Eng J Med 2005; 352: 1425-1435 22% RRR HR = 0.78 (95% CI 0.69, 0.89) P< 0.001 Proportion of patients experiencing major cardiovascular event (%) 0 0.05 0.10 0.15 Atorvastatin 10 mg Atorvastatin 80 mg 0123456 Time (years) 22% Relative Risk Reduction
 P< Proportion of patients experiencing major cardiovascular event (%) Atorvastatin 10 mg Atorvastatin 80 mg Time (years) 22% Relative Risk Reduction.")
25
Prescribing Information is available at the end of this presentation CHD death or non-fatal, non-procedure-related MI 0123456 Time (years) Proportion of patients experiencing CHD death or non-fatal non-PR MI (%) 0.05 0.10 22% RRR HR = 0.78 (95% CI 0.68, 0.91) P<0.001 0 Atorvastatin 10 mg Atorvastatin 80 mg Adapted from LaRosa JC et al. N Eng J Med 2005; 352: 1425-1435 22% Relative Risk Reduction

26
Prescribing Information is available at the end of this presentation Fatal or non-fatal stroke Proportion of patients experiencing fatal or non-fatal stroke (%) 0123456 Time (years) 0 0.01 0.02 0.04 0.03 25% RRR HR = 0.75 (95%CI 0.59, 0.96) P=0.02 Adapted from LaRosa JC et al. N Eng J Med 2005; 352: 1425-1435 Atorvastatin 10 mg Atorvastatin 80 mg 25% Relative Risk Reduction

27
Prescribing Information is available at the end of this presentation Safety No. of patients (%) Atorvastatin 10 mg (n=5,006) Atorvastatin 80 mg (n=4,995) Treatment-related AEs 1 Treatment-related myalgia 2 289 (5.8) 234 (4.7) 406 (8.1) 241 (4.8) Rhabdomyolysis*3 (0.06)2 (0.04) AST/ALT elevation >3 ULN 3 9 (0.2)60 (1.2) *No cases were considered by the investigator with direct responsibility for the patient to be causally related to atorvastatin, and none met ACC/AHA/NHLBI criteria 4 for rhabdomyolysis 1 P<0.001, 2 P=0.72, 3 P<0.001, 4 Pasternak RC et al. Circulation 2002; 106: 1024-1028 Adapted from LaRosa JC et al. N Eng J Med 2005; 352: 1425-1435 Note: n=197 patients were excluded at baseline due to AEs after 8 weeks open-label 10 mg treatment and n=96 were also excluded at baseline due to ALT/AST > 1.5 x ULN
 Atorvastatin 10 mg (n=5,006) Atorvastatin 80 mg (n=4,995) Treatment-related AEs 1 Treatment-related myalgia (5.8) 234 (4.7) 406 (8.1) 241 (4.8) Rhabdomyolysis*3 (0.06)2 (0.04) AST/ALT elevation >3 ULN 3 9 (0.2)60 (1.2) *No cases were considered by the investigator with direct responsibility for the patient to be causally related to atorvastatin, and none met ACC/AHA/NHLBI criteria 4 for rhabdomyolysis 1 P<0.001, 2 P=0.72, 3 P<0.001, 4 Pasternak RC et al. Circulation 2002; 106: Adapted from LaRosa JC et al. N Eng J Med 2005; 352: Note: n=197 patients were excluded at baseline due to AEs after 8 weeks open-label 10 mg treatment and n=96 were also excluded at baseline due to ALT/AST > 1.5 x ULN.")
28
Prescribing Information is available at the end of this presentation Summary The TNT study is the first randomised trial designed to demonstrate the benefits of lowering LDL-C below 2.6 mmol/L in stable CHD patients Significant (>20%) reductions in CV events including stroke were achieved with atorvastatin 80 mg vs atorvastatin 10 mg Even at high atorvastatin dose, there was a very low incidence of adverse events and no treatment-related rhabdomyolysis The findings add to other data showing the efficacy and safety of high-dose (80 mg) atorvastatin LaRosa JC et al. N Eng J Med 2005; 352: 1425-1435

29
Prescribing Information is available at the end of this presentation Effect of Statin Therapy on Lipid Lowering, Ischaemic Heart Disease & Stroke: Meta-Analyses Law MR et al. BMJ 2003; 326: 1423-1429

30
Prescribing Information is available at the end of this presentation Meta-analysis 1: Percentage reduction in serum LDL-C concentration by statin & daily dose Adapted from Law MR et al. BMJ 2003; 326: 1423-1429 Adapted from a meta-analysis of 164 randomised, placebo controlled trials involving over 24,000 patients treated with statins and 14,000 treated with placebo. Percentage reductions are independent of pre-treatment LDL-C concentration. Data not shown for fluvastatin and lovastatin. P-values not available. atorvastatin pravastatin simvastatin rosuvastatin 0 -10 -20 -30 -40 -50 -60 10mg20mg10mg40mg20mg40mg10mg80mg10mg20mg 40mg 80mg -20 -24 -27 -29 -32 -37 -42 -43 -48 -49 -53 -55 Mean percentage change LDL-C from baseline

31
Prescribing Information is available at the end of this presentation Safety Muscle-related adverse effects In the meta-analysis of 35,000 people treated with statins and placebo rhabdomyolosis was diagnosed (variable criteria) in eight treated and five placebo patients, none with serious illness or death Raised serum creatine kinase activity ( ≥ 10 times the ‘upper limit of normal’) was reported in 55 treated patients (0.17%) and 43 placebo patients (0.13%); muscle symptoms were present in 13 and 4 respectively Liver-related adverse effects There were no cases of liver failure in the trials Raised ALT ( ≥ 3 x ULN) was reported in 449 treated (1.3%) and 383 placebo patients (1.1%) Law MR et al. BMJ 2003; 326: 1423-1429

32
Prescribing Information is available at the end of this presentation

Similar presentations






 event rates in secondary prevention and acute coronary syndrome trials A. Kumar, C.P. Cannon. Arch Med Sci 2007;3:S115-S125.>")


: Design Cannon CP.>")




 The LIPID Study Group N Engl J Med 1998;339:1349-57.>")



 Simvastatin in Patients With Prior Cerebrovascular Disease: HPS *29% RRR, p=0.001 Heart Protection Study Collaborative Group. Lancet. 2004;363:757-767.>")

1071-1080 REVERSAL 657 CHD Patients Atorvastatin 80mg Pravastatin 40mg Randomised, double blind multicentre trial performed.>")

 vs. placebo FU 5 years total cholesterol 25%; LDL.>")
>")