Download presentation
Presentation is loading. Please wait.

1
Treat Everyone to an LDL-C of 70mg/dl? Daniel Edmundowicz, MS, MD, FACC Associate Professor Of Medicine Director, Preventive Cardiology UPMC Cardiovascular Institute

2
4.50 2.85 1.80 1.15 0.75 91 LDL-C (mg/dL) ARIC Study (Men) Relative risk of CHD Adjusted for age and race 10-year follow-up N=5432 LDL = low-density lipoprotein; LDL-C = LDL cholesterol; ARIC = Atherosclerosis Risk in Communities. Adapted from Sharrett et al. Circulation. 2001;104:1108. 110130149168188 Dyslipidemia and CHD: LDL-C

3
UPMC Cardiovascular Institute LaRosa JC et al. NEJM. 2005;352:1425-1435 LDL-C=Low density lipoprotein cholesterol; TNT=Treating to New Targets; HPS=Heart Protection Study; CARE=Cholesterol and Recurrent Events Trial; LIPID=Long-term Intervention with Pravastatin in Ischaemic Disease; 4S=Scandinavian Simvastatin Survival Study. 30 25 20 15 10 5 0 07090110130150170190210 LDL-C (mg/dL) TNT (atorvastatin 80 mg/d) TNT (atorvastatin 10 mg/d) HPS CARE LIPID CARE HPS Event (%) 4S Statin Placebo Relationship between LDL Levels and Event Rates in Secondary Prevention Trials of Patients with Stable CHD HMG-CoA Reductase Inhibitor: Secondary Prevention
 TNT (atorvastatin 80 mg/d) TNT (atorvastatin 10 mg/d) HPS CARE LIPID CARE HPS Event (%) 4S Statin Placebo Relationship between LDL Levels and Event Rates in Secondary Prevention Trials of Patients with Stable CHD HMG-CoA Reductase Inhibitor: Secondary Prevention.")
4
UPMC Cardiovascular Institute LDL approx. 130 mg/dl LDL approx. 50 - 70 mg/dl O’Keefe JH, et al. JACC 2004;43:2142

5
UPMC Cardiovascular Institute

6
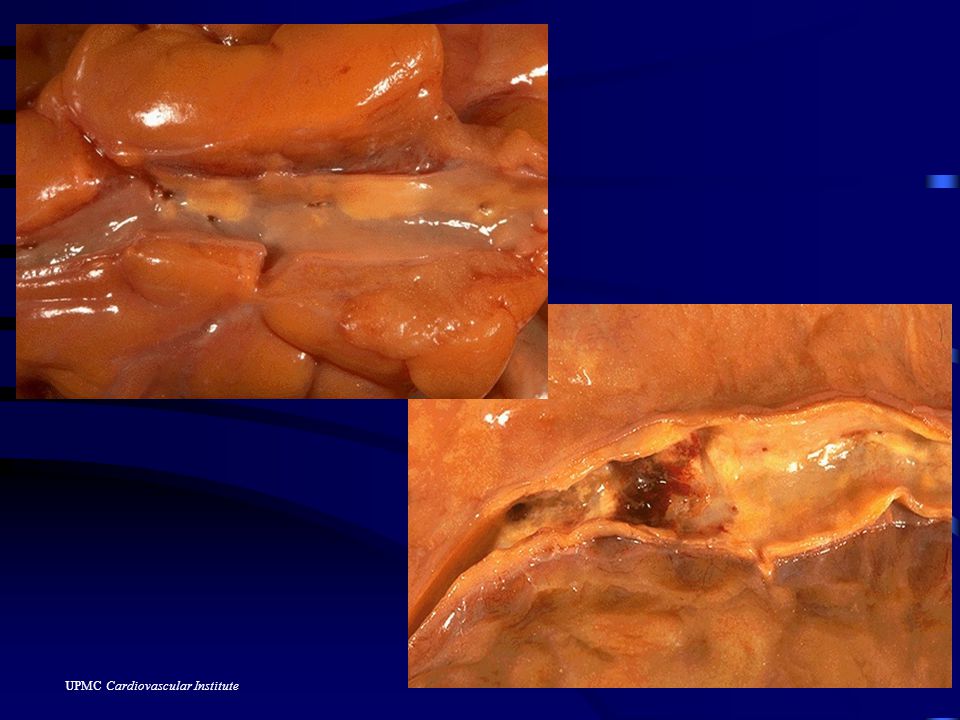
Vascular endothelium modification in atherosclerosis

7
UPMC Cardiovascular Institute

12
Although the LDLC mantra “lower is better” has been popularized in advertising and continuing medical education ……the precise target level for LDLC for optimal treatment has not been rigorously defined. William Isley, MD Mayo Clinic

13
UPMC Cardiovascular Institute “Intention to treat” LDL-C levels and CHD risk: Cholesterol Treatment Trialists’ Collaborators 90,056 participants in 14 randomized trials of Statins Am J Cardiol 2006;98:1405–1408

14
UPMC Cardiovascular Institute Estimates of risk and NNT to prevent one event with additional 30mg/dl LDL lowering Am J Cardiol 2006;98:1405–1408

15
UPMC Cardiovascular Institute “Intention to treat” LDL-C levels and CHD risk by presence of risk factors: “risk curve approach” to LDL therapy Am J Cardiol 2006;98:1405–1408 LDL Therapy Alternative Risk Factor Therapy

16
…Many advocates of “lower is better” seem oblivious to the potential downsides of more aggressive lipid- lowering therapy.

17
UPMC Cardiovascular Institute PROVE-IT and A to Z No significant reduction in non-fatal MI/CHD death 30% drop-out rates Prove-It: Prior statin use or those with baseline LDL <125 had similar outcomes regardless of treatment NNT to cause significant LFT abnl similar to NNT to prevent CV event

18
UPMC Cardiovascular Institute TNT and IDEAL Adverse events and treatment related drug discontinuation 40% more common in high dose atorvastatin Over twice as many subjects in the atorva 80mg group stopped therapy related to side effects compared to simva 20/40.

19
UPMC Cardiovascular Institute LDL goal attainment among Kaiser Permanente Northwest patients over the age of 65 Am Heart J 2007;154:554

20
UPMC Cardiovascular Institute Aggressive vs. Conventional Lipid lowering in 235 patient with CHD Cardiovasc Drugs Ther (2007) 21:91 Simvastatin 40 mg daily Atorvastatin 40 mg daily
 21:91 Simvastatin 40 mg daily Atorvastatin 40 mg daily.")
21
UPMC Cardiovascular Institute Cardiovasc Drugs Ther (2007) 21:91 While LDL was lower, no change in levels of oxidative stress or inflammatory markers with more intensive statin therapy
 21:91 While LDL was lower, no change in levels of oxidative stress or inflammatory markers with more intensive statin therapy")
22
UPMC Cardiovascular Institute Law MR et al. BMJ. 2003;326:1423-1427. Absolute reductions* (mg/dL) and (percentage reductions † ) Statin 10 mg/d20 mg/d40 mg/d80 mg/d Atorvastatin69 (37)80 (43)91 (49)102 (55) Fluvastatin29 (15)39 (21)50 (27) 61 (33) Lovastatin ‡ 39 (21)54 (29)68 (37) 83 (45) Pravastatin37 (20)45 (24)53 (29) 62 (33) Rosuvastatin § 80 (43)90 (48)99 (53)108 (58) Simvastatin51 (27)60 (32)69 (37) 78 (42) *Standardized to LDL-C 186 mg/dL (mean concentration in trials) before treatment. † Independent of pretreatment LDL-C. ‡ Maximum dose of 80 mg/d administered as two 40-mg tablets. § Not FDA approved at 80 mg/d. LDL-C Lowering According to Statin and Dose: A Meta-analysis of 164 Trials
 and (percentage reductions † ) Statin 10 mg/d20 mg/d40 mg/d80 mg/d Atorvastatin69 (37)80 (43)91 (49)102 (55) Fluvastatin29 (15)39 (21)50 (27) 61 (33) Lovastatin ‡ 39 (21)54 (29)68 (37) 83 (45) Pravastatin37 (20)45 (24)53 (29) 62 (33) Rosuvastatin § 80 (43)90 (48)99 (53)108 (58) Simvastatin51 (27)60 (32)69 (37) 78 (42) *Standardized to LDL-C 186 mg/dL (mean concentration in trials) before treatment. † Independent of pretreatment LDL-C. ‡ Maximum dose of 80 mg/d administered as two 40-mg tablets. § Not FDA approved at 80 mg/d. LDL-C Lowering According to Statin and Dose: A Meta-analysis of 164 Trials.")
23
UPMC Cardiovascular Institute Statin Titration Yields Minimal Incremental LDL-C Reduction Jones et al. Am J Cardiol. 2003;92:152. 20%-46% 3%-7% Starting dose of statin % LDL-C reduction 1st doubling of statin dose 2nd doubling 3rd doubling

24
UPMC Cardiovascular Institute Mechanism of Intestinal-Acting Agents

25
UPMC Cardiovascular Institute 47

26
UPMC Cardiovascular Institute 53

27
UPMC Cardiovascular Institute Cost Effectiveness First three available statins available generically Difference in drug acquisition costs is marked (plus monitoring of high dose Rx) Doubtful that the incremental cost would be worth the benefit of more aggressive LDLC lowering in the majority of patients
 Doubtful that the incremental cost would be worth the benefit of more aggressive LDLC lowering in the majority of patients")
28
UPMC Cardiovascular Institute Cost of CVD in the United States Hospital/nursing home Physicians/other professionals Drugs Home health/ other medical durables Lost productivity/ morbidity Lost productivity/ mortality American Heart Association. 1999 Heart and Stroke Statistical Update. 1998. Total direct and indirect costs: $286.5 billion

29
UPMC Cardiovascular Institute Ideal Lipid Lowering Drug Drive LDLC below 70 Live Longer Aphrodisiac Tax Deductible Ozone Friendlier

30
UPMC Cardiovascular Institute

31
Conclusion LDL-C of 70mg/dl or less is a reasonable goal for the highest risk patients (i.e. CHD and diabetes). An individualized clinical management strategy that takes into account the patient’s absolute benefit from further LDL-C reduction as well as from shifting the risk curve downward through non lipid interventions.
. An individualized clinical management strategy that takes into account the patient’s absolute benefit from further LDL-C reduction as well as from shifting the risk curve downward through non lipid interventions..")
32
UPMC Cardiovascular Institute Conclusion (cont.) Moderate dose statin therapy can lower CHD risk in primary and secondary prevention with minimal side effects and, with the availability of several generic statins, with great cost- effectiveness.
 Moderate dose statin therapy can lower CHD risk in primary and secondary prevention with minimal side effects and, with the availability of several generic statins, with great cost- effectiveness.")
Similar presentations



>")















 vs. placebo FU 5 years total cholesterol 25%; LDL.>")
>")

