Download presentation
Presentation is loading. Please wait.

1
CONGENITAL AND ACQUIRED RESPIRATORY DISORDERS IN INFANTS

2
OBJECTIVES n Review of Cardio-Pulmonary Development. n Define changes that occur during transition to extra-uterine life with emphasis on breathing mechanics. n Identify infants at risk for and who have respiratory distress n Review of common neonatal disease states.

3
STAGES OF NORMAL LUNG GROWTH Embryonic - first 5 weeks; formation of proximal airways Pseudoglandular - 5-16 weeks; formation of conducting airways Canalicular - 16-24 weeks; formation of acini Saccular - 24 - 36 weeks; development of gas- exchange units Alveolar - 36 weeks and up; expansion of surface area

4
Pseudoglandular 6-16 weeks

5
Canalicular Phase 16-24 weeks

6
Saccular Phase 24-34 weeks

7
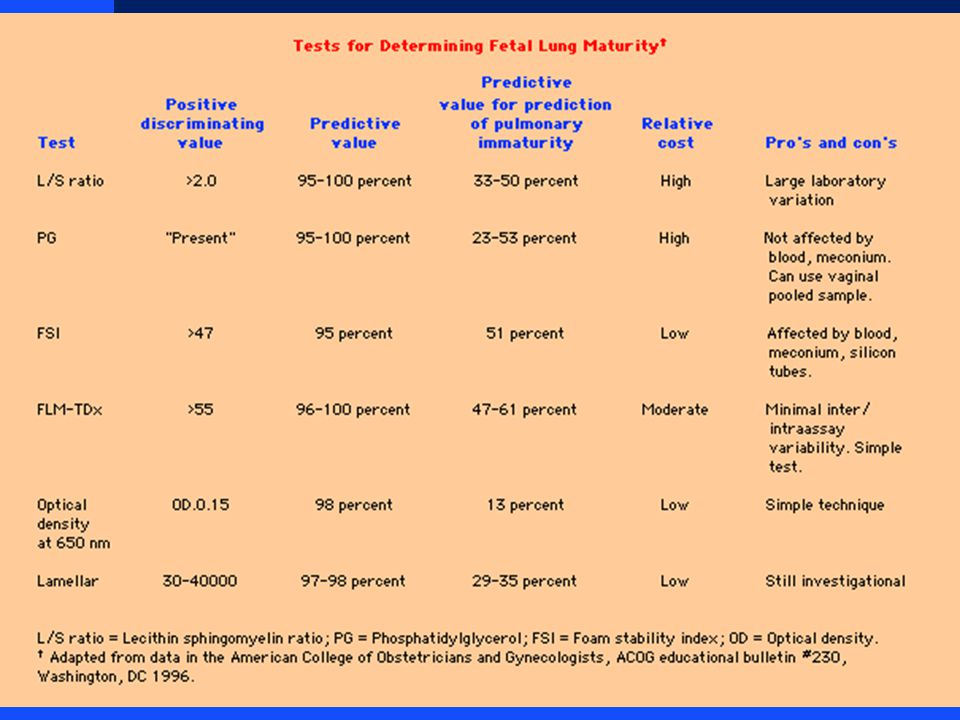
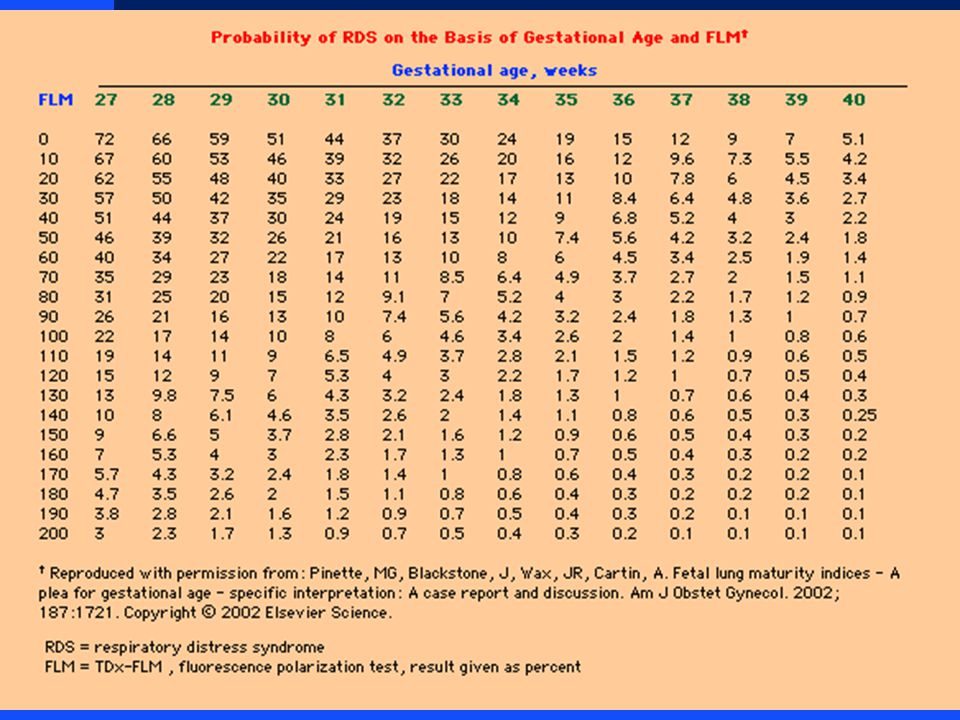
PHYSIOLOGIC MATURATION (Surfactant Production) n Type 2 pneumocytes appear at 24-26 weeks n Responsible for reduction of alveolar surface tension. u LaPlace’s Law n Lipid profile as indicator of lung maturity u L/S Ratio u Flourescence Polarization - FLM n Many other factors influence lung maturation

10
Maturational Factors n Stimulation u Glucorticoids, ACTH u Thyroid Hormones, TRF u EGF u Heroin u Aminophyline,cAMP u Interferon u Estrogens n Inhibition u Diabetes (insulin, hyperglycemia, butyric acid) u Testosterone u TGF-B u Barbiturates u Prolactin
 u Testosterone u TGF-B u Barbiturates u Prolactin")
11
FETAL CIRCULATION

12
TRANSITION TO EXTRA-UTERINE LIFE n Fetal Breathing n Instantaneous; liquid filled to air filled lungs n Maintenance of FRC n Placental blood flow termination n Decreased PVR n Closure of fetal shunts

13
MECHANICS OF BREATHING n Respiratory Control Center...CNS u Metabolic Needs n Negative pressure breathing n Compliance and Resistance u Inspiratory Muscles u Rib Cage F “Compliability becomes a liability”

14
Signs of Respiratory Distress n Tachypnea n Intercostal retractions n Nasal Flaring n Grunting n Cyanosis

15
When is it abnormal to show signs of respiratory distress? n When tachypnea, retractions, flaring, or grunting persist beyond one hour after birth. n When there is worsening tachypnea, retractions, flaring or grunting at any time. n Any time there is cyanosis

16
Causes of Neonatal Respiratory Distress n Obstructive/restrictive - mucous, choanal atresia, pneumothorax, diaphragmatic hernia. n Primary lung problem - Respiratory Distress Syndrome (RDS), meconium aspiration, bacterial pneumonia, transient (TTN). n Non -pulmonary - hypovolemia/hypotension, congenital heart disease, hypoxia, acidosis, cold stress, anemia, polycythemia
, meconium aspiration, bacterial pneumonia, transient (TTN). n Non -pulmonary - hypovolemia/hypotension, congenital heart disease, hypoxia, acidosis, cold stress, anemia, polycythemia.")
17
Infants at Risk for Developing Respiratory Distress n Preterm Infants n Infants with birth asphyxia n Infants of Diabetic Mothers n Infants born by Cesarean Section n Infants born to mothers with fever, Prolonged ROM, foul-smelling amniotic fluid. n Meconium in amniotic fluid. n Other problems

18
Evaluation of Respiratory Distress n Administer Oxygen and other necessary emergency treatment n Vital sign assessment n Determine cause-- physical exam, Chest x-ray, ABG, Screening tests: Hematocrit, blood glucose, CBC n Sepsis work-up

19
Principles of Therapy n Improve oxygen delivery to lungs-- supplemental oxygen, CPAP, assisted ventilation, surfactant n Improve blood flow to lungs-- volume expanders, blood transfusion, partial exchange transfusion for high hematocrit, correct acidosis (metabolic/respiratory) n Minimize oxygen consumption-- neutral thermal environment, warming/humidifying oxygen, withhold oral feedings, minimal handling
 n Minimize oxygen consumption-- neutral thermal environment, warming/humidifying oxygen, withhold oral feedings, minimal handling")
20
DISEASE STATES n Respiratory Distress Syndrome n Transient Tachypnea of the Newborn n Meconium Aspiration Syndrome n Persistent Hypertension of the Newborn n Congenital Pneumonia n Congenital Malformations n Acquired Processes

21
RESPIRATORY DISTRESS SYNDROME Surfactant Deficiency Tidal Volume Ventilation Pulmonary Injury Sequence

22
CLINICAL FEATURES OF RDS n Tachypnea/Apnea n Dyspnea n Grunting/Flaring n Hypoxemia n Radiographic Features n Pulmonary Function Abnormalities

23
Early RDS

24
Progressive RDS

25
Late RDS

26
Hyaline Membrane Disease

27
THERAPY FOR RDS n Oxygen - maintain PaO2 > 50 torr n Nasal CPAP n Intermittent Mandatory Ventilation n Surfactant Replacement n High Frequency Ventilation n Intercurrent Therapies

28
PIE

29
PIE Pathology

30
PIE Histology

31
Pneumothorax/PIE

32
Pneumothorax

33
Pneumopericardium

34
TRANSIENT TACHYPNEA OF THE NEWBORN n Delayed Fluid Resorption n Hard to differentiate early on from RDS both clinicaly and radiographicaly especially in the premature infant n Initial therapy similar to RDS, but hospital course is quite different

35
Wet Lung

36
MECONIUM ASPIRATION SYNDROME n Chemical Pneumonitis n Surfactant Inactivation n Potential for Infection n Potential for Pulmonary Hypertension n Management varies on severity

37
Meconium Aspiration

38
PERSISTENT PULMONARY HYPERTENSION n Usually secondary to primary pulmonary disease state n Pulmonary Vascular Lability n Treat the underlying problem n Maintain normo-oxygenation n Selective Pulmonary Vasodilators n Pray for good luck

39
PPHN

40
CONGENITAL PNEUMONIA n Infectious; primarily GBS n Amniotic Fluid aspiration n Viral etiology n Surfactant inactivation

41
GBS Pneumonia

42
CONGENITAL MALFORMATIONS n Choanal Atresia n Tracheal Atresia/stenosis n Chest Mass u Diaphragmatic hernia u CCAM u Sequestration u Lobar emphysema

43
CCAM

44
Lobar Emphysema

45
Diaphragmatic Hernia

46
Chylothorax

47
Phrenic Nerve Paralysis

48
ACQUIRED DISEASES n Infections n Bronchopulmonary Dysplasia n Sub-glottic stenosis n Apnea of Prematurity

49
Early BPD

50
Progressive BPD

51
Late BPD

52
APNEA Definition: cessation of breathing for longer than a 15 second period or for a shorter time if there is bradycardia or cyanosis

53
Babies at Risk for Apnea n Preterm n Respiratory Distress n Metabolic Disorders n Infections n Cold-stressed babies who are being warmed n CNS disorders n Low Blood volume or low Hematocrit n Perinatal Compromise n Maternal drugs in labor

54
Anticipation and Detection n Place at-risk infants on cardio- respiratory monitor n Low heart rate limit (80-100) n Respiratory alarm (15-20 seconds)
 n Respiratory alarm (15-20 seconds)")
55
Treatment n Determine cause: n x-ray n blood sugar n body and environmental temperature n hematocrit n sepsis work up n electrolytes n cardiac work up n r/o seizure

56
Treatment n CPAP n Theophylline/Caffeine therapy n Mechanical ventilation n Apnea monitor

Similar presentations

>")













 LECTURE Dr. Essam H. Jiffri.>")
 Respiratory Distress Syndrome.>")



