Download presentation
Presentation is loading. Please wait.

1
SMEAR NEGATIVE TUBERCULOSIS
FAIEZA SAHID DEPT. OF INFECTIOUS DISEASES

2
BACKGROUND STATISTICS DEFINITIONS WHO GUIDELINES MODALITIES TO DIAGNOSE SMEAR NEGATIVE TB

3
Anastasis D et al 1997; Behr MA et al 1999
BACKGROUND In South Africa tuberculosis (TB) has reached crisis proportions, being responsible for more than 80% of notifiable diseases. KwaZulu-Natal is considered the epicentre of HIV associated TB, where two thirds of all patients with TB are co-infected with HIV. HIV/AIDS modifies the clinical and radiological presentation as well as the diagnostic utility of sputum smears resulting in an increase in smear negative pulmonary TB. Of importance, it has been demonstrated that smear negative TB remains a public health risk with a transmission rate of 22 to 47% relative to smear positive cases. Anastasis D et al 1997; Behr MA et al 1999
 has reached crisis proportions, being responsible for more than 80% of notifiable diseases. KwaZulu-Natal is considered the epicentre of HIV associated TB, where two thirds of all patients with TB are co-infected with HIV. HIV/AIDS modifies the clinical and radiological presentation as well as the diagnostic utility of sputum smears resulting in an increase in smear negative pulmonary TB. Of importance, it has been demonstrated that smear negative TB remains a public health risk with a transmission rate of 22 to 47% relative to smear positive cases. Anastasis D et al 1997; Behr MA et al")
4
BACKGROUND Disproportionate increase in rates of smear negative pulmonary and extrapulmonary tuberculosis in HIV prevalent resource limited settings results in: Cultures frequently not available Delayed diagnosis May contribute to mortality Higher mortality in HIV infected, especially smear negative patients. In the absence of rapid, simple, and accurate diagnostic tools for smear-negative pulmonary and extrapulmonary tuberculosis, diagnostic algorithms have been recommended. In countries with a high prevalence of HIV infection, smear-negative tuberculosis has a poorer prognosis.12 In one study in sub-Saharan Africa, a third of patients with smear negative tuberculosis died within a year of their initial diagnosis.13 Roughly a third of the rest developed recurrent pulmonary tuberculosis.

5
WHO GLOBAL TB REPORT 2008 South Africa → highest TB incidence in the world 5 times the average incidence rate found in the 22 high-burden countries. 4th highest estimated total burden of TB for 2006, behind only India, China and Indonesia, countries with much larger populations. In 2006, South Africa with only 0.7% of the world’s population had an estimated 28% of HIV-positive adult TB cases reported globally. According to the W.H.O. Global Tuberculosis Report 2008, South Africa had the highest TB incidence in the world, at over 5 times the average incidence rate found in the 22 high-burden countries. It had the 4th highest estimated total burden of TB for 2006, behind only India, China and Indonesia, countries with much larger populations. In 2006, South Africa with only 0.7% of the world’s population had an estimated 28% of HIV-positive adult TB cases reported globally. National TB Control Programme data shows that over the last five years TB case notification has increased by a massive 81%, from 188,695 cases in 2001 to 341,165 in In 2006, Kwa-Zulu Natal had the highest total TB caseload accounting for 31% of all TB cases nationally.

6
STATISTICS (2006) Estimated 9.2 million new TB cases in 2006.
1.7 million deaths 200,000 in clients co-infected with HIV. Incidence highest in the African region at 363 cases per 100,000 population compared to a global figure of 139 per 100,000 population. Incidence in South Africa 940 per 100,000 population. Despite the decline in TB incidence, the total number of new TB cases is still rising and TB is still a major cause of morbidity and mortality. There were an estimated 9.2 million new TB cases in 2006 and 1.7 million deaths, including 200,000 in clients co-infected with HIV. Developing regions still bear the greatest brunt of TB with incidence highest in the African region at 363 cases per 100,000 population compared to a global figure of 139 per 100,000 population. Incidence in South Africa at 940 per 100,000 population. WHO SA TB STATS 2006 INCIDENCE OF TB (PER POPULATION PER YR) 940.0 PREVALENCE OF TB (PRE POPULATION PER YR) 998.0
 PREVALENCE OF TB (PRE POPULATION PER YR)")
7
Smear Negative PTB Cases
Table 1.1: TB Case Finding 2006 All TB Cases PTB Cases New Smear Positive PTB Cases Retreatment Smear Positive PTB Cases Smear Negative PTB Cases No Smear PTB Cases Children 0-7 years EPTB Cases Incidence All TB cases per 100,000 Incidence PTB cases per 100,000 EASTERN CAPE 48,512 41,558 19,527 8,473 3,615 9,943 2,805 6,954 687 589 FRRE STATE 23,374 19,058 9,553 2,840 2,479 4,186 2,295 4,316 789 643 GAUTENG 46,093 34,290 20,609 4,188 2,915 6,578 4,155 11,803 501 372 KZN 104,705 88,271 32,855 9,527 20,547 25,342 8,593 16,434 1076 907 LIMPOPO 17,301 14,118 7,574 1,323 1,305 3,916 1,069 3,183 305 249 MPUMALANGA 15,035 13,496 7,216 1,081 859 4,340 7,55 1,539 463 416 NORTH WEST 28,421 24,519 12,539 2,954 1,764 7,262 2,156 3,902 738 637 NORTHERN CAPE 8,631 7,951 3,583 1,482 901 1,986 1,018 680 950 875 WESTERN CAPE 49,093 43,296 17,644 8,563 8,366 8,723 6,955 5,797 1,033 911 SOUTH AFRICA 341,165 286,557 131,100 40,431 42,751 72,276 29,801 54,608 720 605

8
REVISED CASE DEFINITIONS (HIV ONLY)
Smear-positive pulmonary tuberculosis only requires one positive smear result. Smear-negative pulmonary TB: At least two sputum exams negative for AFB and X-ray consistent with active TB and Decision by clinician to treat with full course for TB OR AFB smear-negative sputum with cultures that are positive.

9
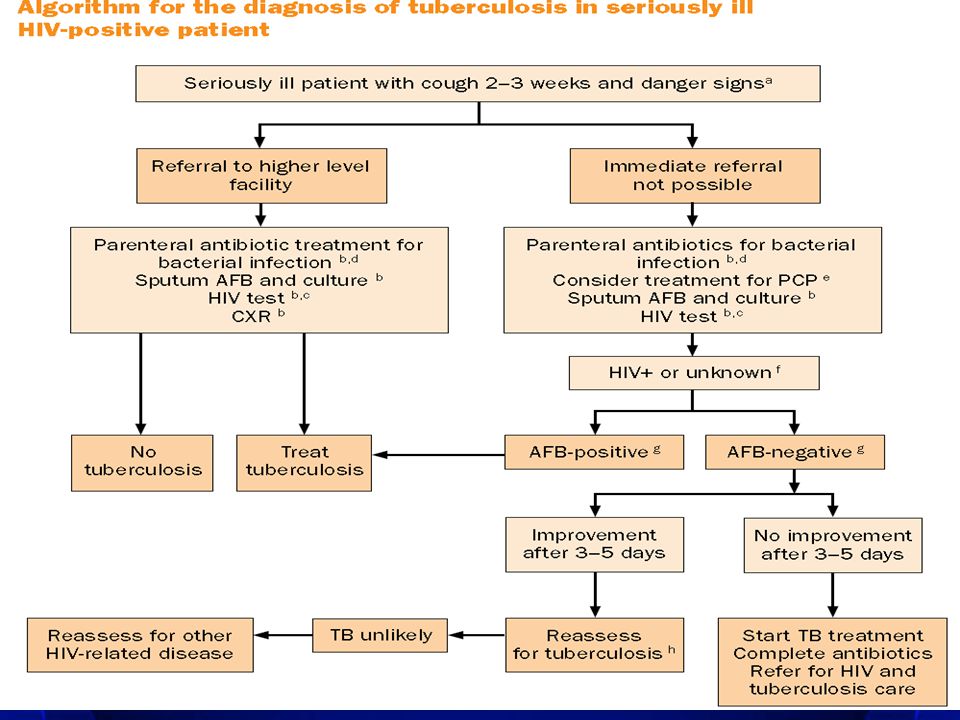
DANGER SIGNS RR > 30 TEMP > 39 PR > 120 UNABLE TO WALK UNAIDED In the absence of rapid and simple tools to diagnose tuberculosis, the main aim of these algorithms is to assist clinical decision-making in HIV-prevalent and resource-constrained settings, to expedite the diagnostic process and minimize incorrect diagnosis and mortality. First visit: HIV testing should be offered and AFB sputum examination should be performed. If AFB test is positive, treat for tuberculosis. • Second visit: If the AFB examination is negative, the patient should be provided with all available investigations during the second visit. The second visit should ideally take place on the second day following first presentation at the health facility. The investigations include: repeated sputum AFB, sputum culture and chest X-ray. Clinical assessment is also important for deciding whether to put the patient on antituberculosis treatment at this stage. HIV assessment should also be performed and co‑trimoxazole preventive therapy provided according to national guidelines. • Third visit: Results of the second-visit investigations (except culture) should be available during the patient’s third visit. Patients suspected of having tuberculosis after these investigations (e.g. compatible radiograph plus symptoms) should be treated for tuberculosis. Patients who are not treated for tuberculosis should receive either a broadbased antibiotic (not a fluoroquinolone) to treat bacterial infection or treatment for PCP. HIV assessment should also be performed and co‑trimoxazole preventive therapy provided according to national guidelines. • Fourth visit: The patient’s response is assessed and a clinical follow-up mechanism is established (in either the tuberculosis or the HIV services). For patients with immediate response to PCP or antibiotic treatment, continued vigilance is necessary to exclude superimposed tuberculosis. Those patients with an unsatisfactory response to treatment for PCP or bacterial pneumonia should be reassessed both clinically and bacteriologically for tuberculosis.
 should be available during the patient’s third visit. Patients suspected of having tuberculosis after these investigations (e.g. compatible radiograph plus symptoms) should be treated for tuberculosis. Patients who are not treated for tuberculosis should receive either a broadbased antibiotic (not a fluoroquinolone) to treat bacterial infection or treatment for PCP. HIV assessment should also be performed and co‑trimoxazole preventive therapy provided according to national guidelines. • Fourth visit: The patient’s response is assessed and a clinical follow-up mechanism is established (in either the tuberculosis or the HIV services). For patients with immediate. response to PCP or antibiotic treatment, continued vigilance is necessary to exclude superimposed tuberculosis. Those patients with an unsatisfactory response to treatment for PCP or bacterial pneumonia should be reassessed both clinically and bacteriologically for tuberculosis.")
12
EXTRAPULMONARY TUBERCULOSIS (EPTB)
CRITERIA: One specimen from an extrapulmonary site culture-positive OR Histological or strong clinical evidence consistent with active extrapulmonary tuberculosis and Decision by clinician to treat with full course for TB and Laboratory confirmation of HIV infection or Strong clinical evidence of HIV infection

13
EPTB – CLINICAL FEATURES

14
EPTB Maintain high clinical vigilance for EPTB.
Assess clinical response to TB treatment after one month and seek alternative diagnosis if no improvement. One in five registered tuberculosis patients has extrapulmonary tuberculosis (8, 9, 10). The commonest forms include lymph node (especially in the neck or under the arms), pleural (usually one-sided pleural effusion) and disseminated tuberculosis (disease that is not limited to one site in the body). Pericardial and meningeal tuberculosis are less frequent forms of extrapulmonary tuberculosis that are also covered in these guidelines. About one-third of deaths in HIV-positive Africans are due to disseminated tuberculosis (11, 12, 13) but only about half of HIV-positive patients who die from disseminated tuberculosis are diagnosed before death (12, 13, 14). With the exception of lymph node tuberculosis, which can usually be confirmed through aspiration of affected lymph nodes, most patients with extrapulmonary tuberculosis are managed without bacteriological or histological confirmation (15).
. The commonest forms include lymph node (especially in the neck or under the arms), pleural. (usually one-sided pleural effusion) and disseminated tuberculosis (disease that is not limited to one site in the body). Pericardial and meningeal tuberculosis are less frequent forms of extrapulmonary tuberculosis that are also covered in these guidelines. About one-third of deaths in HIV-positive Africans are due to disseminated tuberculosis (11, 12, 13) but only about half of HIV-positive patients who die from disseminated tuberculosis are diagnosed before death (12, 13, 14). With the exception of lymph node tuberculosis, which can usually be confirmed. through aspiration of affected lymph nodes, most patients with extrapulmonary tuberculosis are managed without bacteriological or histological confirmation (15).")
15
EPTB HIV testing offered to all patients suspected of EPTB..
This is because HIV-related EPTB is an indication for early commencement of antiretroviral treatment (clinical stage 4 of HIV disease). For HIV-related EPTB, the following interventions should be carried out: refer for HIV care or start antiretroviral treatment according to national guidelines. start co‑trimoxazole preventive therapy. remain vigilant for clinical deterioration of EPTB after the start of antiretroviral treatment (immune reconstitution inflammatory syndrome – IRIS) and take appropriate measures.
. For HIV-related EPTB, the following interventions should be carried out: refer for HIV care or start antiretroviral treatment according to national guidelines. start co‑trimoxazole preventive therapy. remain vigilant for clinical deterioration of EPTB after the start of antiretroviral treatment (immune reconstitution inflammatory syndrome – IRIS) and take appropriate measures.")
16
LATENT VS ACTIVE TB Maintained = TB remains dormant or latent
Cleared = No infection Adequacy of Innate defences Maintenance of Acquired Defences Contained = Latent Infection (LTBI) TB exposure Development of Acquired defences Not cleared = Primary Infection Not maintained = Late reactivation or Post primary TB In total, 13 studies were included. Assays based on RD1-specific antigens, ESAT-6 or CFP-10, correlate better with intensity of exposure, and therefore are more likely than TST/purified protein derivative (PPD)-based assays to detect LTBI accurately. An additional advantage is that they are more likely to be independent of BCG vaccination status and HIV status. Not contained = Progressive Primary Disease
 TB exposure. Development of. Acquired. defences. Not cleared = Primary Infection. Not maintained = Late reactivation or. Post primary TB. In total, 13 studies were included. Assays based on RD1-specific antigens, ESAT-6 or CFP-10, correlate better with intensity of exposure, and therefore are more likely than TST/purified. protein derivative (PPD)-based assays to detect LTBI accurately. An additional advantage is that they are more likely to be independent of BCG vaccination status and HIV status. Not contained = Progressive Primary. Disease.")
17
TESTS FOR LATENT TB TST Standardised screening test for detecting LTBI in high risk groups A negative skin test never excludes TB Interferon gamma release assays Quantiferon (based on PPD) Quantiferon Gold (based on ESAT 6 and CFP 10) False positives due to other mycobacteria or BCG vaccination False negatives due to anergy or overwhelming TB early secretory antigen target 6 (ESAT-6) and culture filtrate protein 10 (CFP-10). Various commercial and in-house tests based on PPD, ESAT-6 and/or CFP-10 have been evaluated using either an enzyme-linked immunospot assay (ELISPOT) or an enzyme-linked immunosorbent assay (ELISA). The two commercial tests using ELISA are Quantiferon® (based on PPD) and Quantiferon Gold®150 (based on ESAT-6 and CFP-10). The T SPOT-TB® assay151,152 is an ELISPOT assay and is also based on RD1-specific antigens.
 Quantiferon Gold (based on ESAT 6 and CFP 10) False positives due to other mycobacteria or BCG vaccination. False negatives due to anergy or overwhelming TB. early secretory antigen target 6 (ESAT-6) and culture filtrate protein 10 (CFP-10). Various commercial and in-house tests based on PPD, ESAT-6 and/or CFP-10 have been evaluated using either an enzyme-linked immunospot assay (ELISPOT) or an enzyme-linked immunosorbent assay (ELISA). The two commercial tests using ELISA are Quantiferon® (based on PPD) and Quantiferon Gold®150 (based on ESAT-6 and CFP-10). The T SPOT-TB® assay151,152 is an ELISPOT assay and. is also based on RD1-specific antigens.")
18
DIAGNOSIS OF SNTB CULTURE MOLECULAR TECHNIQUES CLINICAL FEATURES SMEAR

19
CLINICAL FEATURES Clinical features not sensitive or specific to distinguish TB from non-TB. Studies aimed to identify frequently occurring clinical features in smear negative TB in areas with high prevalence of HIV and TB: Hospital based study in Ethiopia, loss of appetite, weight loss, fever, night sweats, chest pain, haemoptysis and breathlessness were more common in patients with PTB (smear pos and smear neg) than in those without PTB. Pts with smear negative TB had night sweats for a longer period of time. Smear pos pts were more likely to have fever and weight loss than the smear negative group. Clinical features not sensitive or specific to distinguish TB from non-TB. Often results of pulmonary examinations are normal. Physical examination is, however, important in extrapulmonary forms of tuberculosis, namely cardiovascular examination to detect signs of pericarditis and neurological examination to detect meningitis.22 studies aimed to identify frequently occurring clinical features in smear-negative tuberculosis in areas with high prevalence of HIV infection and tuberculosis. In a hospital-based study in Ethiopia, loss of appetite, weight loss, fever, night sweats, chest pain, haemoptysis, and breathlessness were more common in patients with pulmonary tuberculosis (both smear positive and smear negative) than in those without pulmonary tuberculosis.24 However, patients with smear-negative tuberculosis had night sweats for a longer time. Smear-positive patients were more likely to have fever and weight loss than the smear negative group.
 than in those without PTB. Pts with smear negative TB had night sweats for a longer period of time. Smear pos pts were more likely to have fever and weight loss than the smear negative group. Clinical features not sensitive or specific to distinguish TB from non-TB. Often results of pulmonary examinations are normal. Physical examination is, however, important in extrapulmonary forms of tuberculosis, namely cardiovascular examination to detect signs of pericarditis and neurological examination to detect meningitis.22. studies aimed to identify frequently occurring clinical features in smear-negative tuberculosis in areas with high prevalence of HIV infection and tuberculosis. In a hospital-based study in Ethiopia, loss of appetite, weight loss, fever, night sweats, chest pain, haemoptysis, and breathlessness were more common in patients with pulmonary tuberculosis (both smear positive and smear. negative) than in those without pulmonary tuberculosis.24. However, patients with smear-negative tuberculosis had night sweats for a longer time. Smear-positive patients were more likely to have fever and weight loss than the smear negative group.")
20
CLINICAL FEATURES Tanzania and Burundi identified 4 clinical criteria for diagnosis of SNTB presence of cough for longer than 21 days (odds ratio 5·43[1·95–15·1]); presence of chest pain for longer than 15 days (1·98 [0·77–5·12]); absence of expectoration (odds ratio for expectoration 0·42 [0·15–1·18]); absence of shortness of breath (odds ratio for breathlessness 0·26 [0·01–0·66]). Diagnosis of smear negative tuberculosis by any two of these criteria had a sensitivity of 85% but a low specificity of 67% (positive predictive value 43%, negative predictive value 94%).
; presence of chest pain for longer than 15 days (1·98 [0·77–5·12]); absence of expectoration (odds ratio for expectoration 0·42 [0·15–1·18]); absence of shortness of breath (odds ratio for breathlessness 0·26 [0·01–0·66]). Diagnosis of smear negative tuberculosis by any two of these criteria had a sensitivity of 85% but a low specificity of 67% (positive predictive value 43%, negative predictive value 94%).")
21
Perkins M 2000, Best et al 1990, Steingart K 2006
SMEAR Despite its limitations, smear microscopy remains the primary diagnostic tool because it is inexpensive, specific in endemic regions and identifies patients that pose the greatest public health risk. Processing methods: NALC method – improves sensitivity by 66 to 83% compared to direct microscopy. Bleach method – favoured in resource limited settings because bleach kills mycobacteria, eliminating the need for biosafety cabinets. It was shown that bleach and centrifugation increased sensitivity by 18%. Perkins M 2000, Best et al 1990, Steingart K 2006

22
CULTURE Most sensitive of currently available tests (sensitivity of 98% have been reported), and also permits identification and drug sensitivity tests to be made. Specificity is higher → each live bacillus forms colonies on culture. Requires up to 6–8 weeks for the isolation of M. TB from a clinical specimen and in 10–20% of cases the bacillus is not successfully cultured. Estimated that 10% of smear-negative patients are also culture negative. Not all patients with clinical TB will have positive cultures.
, and also permits identification and drug sensitivity tests to be made. Specificity is higher → each live bacillus forms colonies on culture. Requires up to 6–8 weeks for the isolation of M. TB from a clinical specimen and in 10–20% of cases the bacillus is not successfully cultured. Estimated that 10% of smear-negative patients are also culture negative. Not all patients with clinical TB will have positive cultures.")
23
CULTURE Solid medium : Lowenstein Jensen Medium – egg based.
Middle Brook 7H10/7H11 – agar based. Simple and cost effective to use. Slow bacterial growth therefore detection of bacilli occurs within 3 – 4 weeks. Liquid medium : Semi – automated Radiometric System BACTEC 460 – uses radiation technology. Automated Non-Radiometric Systems (MGIT) – uses fluorometric technology Detection of bacilli occurs within 7 – 14 days. NB!! Liquid medium is used in conjunction with solid medium as back up. The detection of bacilli occurs within 7 to 14 days in liquid medium. The major limitation to the use of these methods is the high cost involved.
 – uses fluorometric technology. Detection of bacilli occurs within 7 – 14 days. NB!! Liquid medium is used in conjunction with solid medium as back up. The detection of bacilli occurs within 7 to 14 days in liquid medium. The major limitation to the use of these methods is the high cost involved.")
24
MOLECULAR TECHNIQUES The NAAT tests provide a reliable way of increasing the specificity of diagnosis (ruling in disease) but sensitivity is too poor to rule out disease, especially in smear-negative (paucibacillary) disease where clinical diagnosis is equivocal and where the clinical need is greatest. Nucleic acid amplification tests: Gen -Probe Amplified M.TB direct test (sensitivity of 70.2% and specificity of 94.6% in smear negative patients) Roche Amplicor M.TB test (sensitivity of 57.5% and specificity of 95.5%) HAIN’s PCR Mycobacteriophage based method Alternative to PCR Detect only viable mycobacteria and can yield antibiotic sensitivities within 2-3 days Not clear whether these tests have sufficiently high sensitivity in smear negative samples to recommend their routine use in practice A systematic review of rapid diagnostic tests for the detection of tuberculosis infection J Dinnes, J Deeks, H Kunst, A Gibson, E Cummins, N Waugh, F Drobniewski and A Lalvani Health Technology Assessment 2007; Vol. 11: No. 3 Dinnes et al 2007
 but sensitivity is too poor to rule out disease, especially in smear-negative (paucibacillary) disease where clinical diagnosis is equivocal and where the clinical need is greatest. Nucleic acid amplification tests: Gen -Probe Amplified M.TB direct test (sensitivity of 70.2% and specificity of 94.6% in smear negative patients) Roche Amplicor M.TB test (sensitivity of 57.5% and specificity of 95.5%) HAIN’s PCR. Mycobacteriophage based method. Alternative to PCR. Detect only viable mycobacteria and can yield antibiotic sensitivities within 2-3 days. Not clear whether these tests have sufficiently high sensitivity in smear negative samples to recommend their routine use in practice. A systematic review of rapid diagnostic tests for the detection of tuberculosis infection. J Dinnes, J Deeks, H Kunst, A Gibson, E Cummins, N Waugh, F Drobniewski and A Lalvani. Health Technology Assessment 2007; Vol. 11: No. 3. Dinnes et al")
25
CONCLUSIONS New diagnostic techniques are required in addition to AFB microscopy for the identification of smear-negative tuberculosis. These need to be appropriate for use in low income countries. However, until such tests are widely available, algorithms must be developed and validated to assist clinicians working in resource-poor settings.

Similar presentations

















 Gram (+) rod (bacilli). Acid-fast Pulmonary.>")

: Relevance for neurological infections Lucie Jean-Gilles.>")
