Download presentation
Presentation is loading. Please wait.

1
CRT-D Effectiveness by QRS Duration and Morphology in the MADIT-CRT Patients
Wojciech Zareba, MD, PhD, Helmut Klein, MD, Iwona Cygankiewicz, MD, PhD, W. Jackson Hall, PhD, Jeffrey Goldberger, MD, James P. Daubert, MD, Michael R. Gold, MD, Mayer Rashtian, MD, Sami Viskin, MD, Wlodzimierz Kargul, MD, Heinz Pitschner, MD, Scott McNitt, MS and Arthur J. Moss, MD. University of Rochester, Rochester, NY, Northestern University, Chicago, IL, Duke University, Durham, NC, Medical University of South Carolina, Charlston, SC, Foothill Cardiology/California Heart Medical Group, Pasadena, CA, Tel Aviv Sourasky Medical Center, Tela Aviv, Israel, Silesian Medical University, Katowice, Poland, Kerckhoff Medical University, Ban Neuheim, Germany

2
Author Disclosure Information:
W. Zareba - Boston Scientific Corp., S,I; H. Klein - LIFECOR, M,A; Boston Scientific Corp., S,I; I. Cygankiewicz - None; W. Hall - None; J. Goldberger - None; J.P. Daubert - Boston Scientific Corp., M,A; Medtronic, Corp., M,A; CV Therapeutics, Inc., M,A; Biosense Webster, Inc., M,A; S,I; St. Jude Medical, S,I; Biotronik, S,J; M.R. Gold - None; M. Rashtian - None; S. Viskin - None; W. Kargul - None; H. Pitschner - None; S. McNitt - None; A.J. Moss - Boston Scientific Corp., S,I.

3
Multicenter Automatic Defibrillator Implantation Trial – Cardiac Resynchronization Therapy (MADIT-CRT) Moss et al. N Engl J Med 2009;361:

4
ICM NYHA I/II and NICM NYHA II EF < 0.30; QRS >0.13sec
MADIT-CRT Entry Criteria: Ischemic NYHA I-II or non-ischemic NYHA class II EF<0.30 QRS >0.13sec Sinus Rhythm Optimal pharmacologic therapy: B-b (>3 mo.); ACE/ARB (>1 mo.); statins in IHD Exclusions: NYHA III-IV <90 days PTE Acute MI, CABG, PCI <3 months Existing ICD or CRT device AF; PR>250ms; 2nd or 3rd degree HB BUN >70mg/dl or creatinine >3.0mg/dl ICM NYHA I/II and NICM NYHA II EF < 0.30; QRS >0.13sec Randomization N=1,820 ICD only N=731 CRT-D N=1,089
; ACE/ARB (>1 mo.); statins in IHD. Exclusions: NYHA III-IV <90 days PTE. Acute MI, CABG, PCI <3 months. Existing ICD or CRT device. AF; PR>250ms; 2nd or 3rd degree HB. BUN >70mg/dl or creatinine >3.0mg/dl. ICM NYHA I/II and NICM NYHA II EF < 0.30; QRS >0.13sec. Randomization N=1,820. ICD only. N=731. CRT-D. N=1,089.")
5
MADIT-CRT: Baseline Clinical Characteristics
Variable ICD CRT-ICD (N = 731) (N = 1089) Age (yrs) Males (76%) (75%) Ischemic heart disease NYHA class I (16%) (14%) NYHA class II (39%) (41%) Nonischemic heart disease NYHA class II (45%) (45%) EF Table 1. Baseline Demographic and Clinical Characteristics of the Patients. Moss AJ et al. N Engl J Med 2009;361:
 (N = 1089) Age (yrs) Males 553 (76%) 814 (75%) Ischemic heart disease. NYHA class I 113 (16%) 152 (14%) NYHA class II 288 (39%) 446 (41%) Nonischemic heart disease. NYHA class II 330 (45%) 491 (45%) EF Table 1. Baseline Demographic and Clinical Characteristics of the Patients. Moss AJ et al. N Engl J Med 2009;361:")
6
Kaplan-Meier Estimates of the Probability of Survival Free of Heart Failure
Figure 2. Kaplan-Meier Estimates of the Probability of Survival Free of Heart Failure. There was a significant difference in the estimate of survival free of heart failure between the group that received cardiac-resynchronization therapy plus an implantable cardioverter-defibrillator (CRT-ICD) and the group that received an ICD only (unadjusted P<0.001 by the log-rank test). Moss AJ et al. N Engl J Med 2009;361:
 and the group that received an ICD only (unadjusted P<0.001 by the log-rank test). Moss AJ et al. N Engl J Med 2009;361:")
7
Hazard Ratio for CRT-D vs. ICD only in MADIT-CRT
HR (95% CI) P Value Heart failure or Death (0.52–0.84) Heart failure only (0.47–0.74) <0.001 Death at any time (0.69–1.44)
 P Value. Heart failure or Death 0.66 (0.52–0.84) Heart failure only 0.59 (0.47–0.74) < Death at any time 1.00 (0.69–1.44)")
8
Changes in Mean Echocardiographic Left Ventricular Volumes and Ejection Fraction between Baseline and 1-Year Follow-up Figure 4. Changes in Mean Echocardiographic Left Ventricular Volumes and Ejection Fraction between Baseline and 1-Year Follow-up. Paired-sample analyses involved 746 patients who received cardiac-resynchronization therapy plus an implantable cardioverter-defibrillator (CRT-ICD) and 620 patients who received an ICD only. LVEDV denotes left ventricular end-diastolic volume, LVEF left ventricular ejection fraction, and LVESV left ventricular end-systolic volume. The height of each bar indicates the average change in the measure from baseline to 1 year, the vertical lines represent 95% confidence intervals, and P values reflect the significances of the difference in average changes between the two groups. Moss AJ et al. N Engl J Med 2009;361:
 and 620 patients who received an ICD only. LVEDV denotes left ventricular end-diastolic volume, LVEF left ventricular ejection fraction, and LVESV left ventricular end-systolic volume. The height of each bar indicates the average change in the measure from baseline to 1 year, the vertical lines represent 95% confidence intervals, and P values reflect the significances of the difference in average changes between the two groups. Moss AJ et al. N Engl J Med 2009;361:")
9
Effects of CRT-D by QRS Morphology in MADIT-CRT
Non-LBBB 534, 30%

10
Baseline Clinical Characteristics of MADIT-CRT Patients by QRS Morphology
LBBB n=1,281 Non-LBBB n=536 RBBB n=228 IVCD n=308 Age (yrs) 64±11 65±10 66±10* 64±10 Females 394 (31%) 59 (11%)† 18 (8%)† 41 (13%)† Ischemic NYHA class I 143 (11%) 120 (22%)† 47 (21%)† 73 (24%)† Ischemic NYHA class II 420 (33%) 314 (58%)† 150 (66%)† 164 (53%)† Nonischemic NYHA class II 718 (56%) 102 (19%)† 31 (14%)† 71 (23%)† Prior hospitalization 563 (45%) 274 (52%) 112 (50%) 162 (53%) EF (%) 23.5±5.3 24.5±5.0† 25.2±5.0† 23.9±5.2† QRS (ms) 163±19 146±15† 153±15† 142±14† BUN (mg/dl) 21±9 22±9 Creatinine (mg/dl) 1.14±0.32 1.23±0.46† 1.28±0.53 1.18±0.40† * P<0.05; † P<0.01 when comparing with LBBB patients
 64±11. 65±10. 66±10* 64±10. Females. 394 (31%) 59 (11%)† 18 (8%)† 41 (13%)† Ischemic NYHA class I. 143 (11%) 120 (22%)† 47 (21%)† 73 (24%)† Ischemic NYHA class II. 420 (33%) 314 (58%)† 150 (66%)† 164 (53%)† Nonischemic NYHA class II. 718 (56%) 102 (19%)† 31 (14%)† 71 (23%)† Prior hospitalization. 563 (45%) 274 (52%) 112 (50%) 162 (53%) EF (%) 23.5± ±5.0† 25.2±5.0† 23.9±5.2† QRS (ms) 163± ±15† 153±15† 142±14† BUN (mg/dl) 21±9. 22±9. Creatinine (mg/dl) 1.14± ±0.46† 1.28± ±0.40† * P<0.05; † P<0.01 when comparing with LBBB patients.")
11
Baseline Clinical Characteristics of MADIT-CRT Patients by QRS Morphology
LBBB n=1,281 Non-LBBB n=536 RBBB n=228 IVCD n=308 Echo Parameters LVEDV (ml) 251±66 242±52* 231±45† 250±54* LVESV (ml) 180±53 171±41† 162±35† 177±43† LAV (ml) 94±22 93±21 92±22 94±20 Medication: ACE Inhibitors 982 (77%) 418 (78%) 177 (78%) 241 (78%) Ang. Rec. Blockers 278 (22%) 98 (18%) 42 (18%) 56 (18%) Beta-blockers 1204 (94%) 490 (91%)* 202 (89%)† 288 (94%) Diuretics 873 (68%) 353 (66%) 147 (64%) 206 (67%) * P<0.05; † P<0.01 when comparing with LBBB patients
 251± ±52* 231±45† 250±54* LVESV (ml) 180± ±41† 162±35† 177±43† LAV (ml) 94±22. 93±21. 92±22. 94±20. Medication: ACE Inhibitors. 982 (77%) 418 (78%) 177 (78%) 241 (78%) Ang. Rec. Blockers. 278 (22%) 98 (18%) 42 (18%) 56 (18%) Beta-blockers (94%) 490 (91%)* 202 (89%)† 288 (94%) Diuretics. 873 (68%) 353 (66%) 147 (64%) 206 (67%) * P<0.05; † P<0.01 when comparing with LBBB patients.")
12
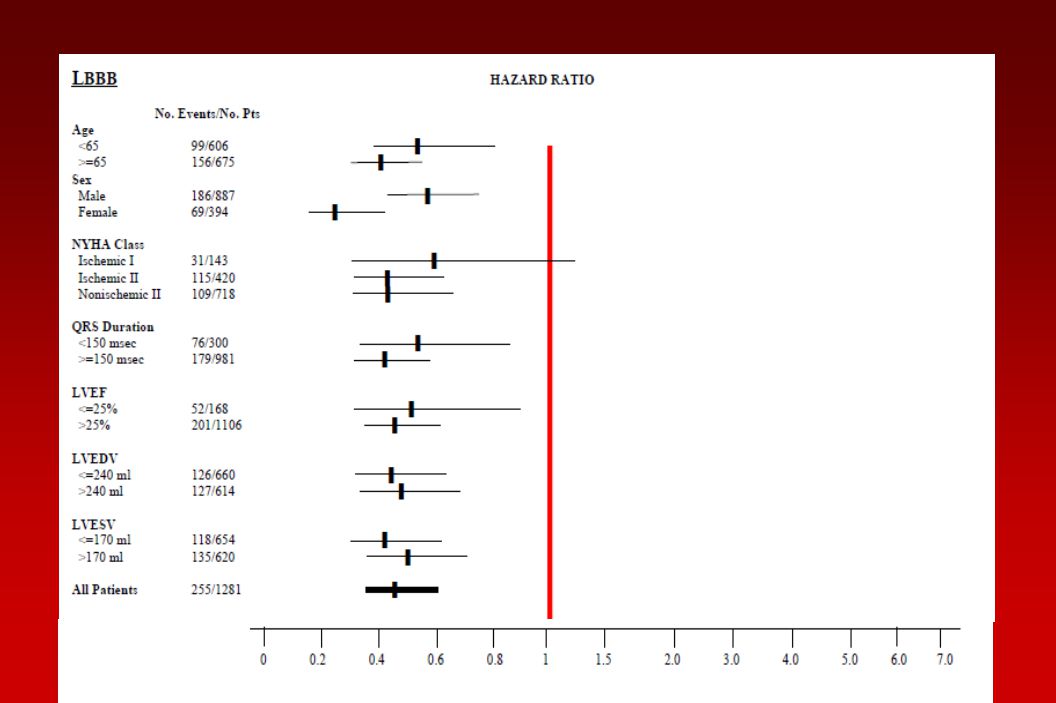
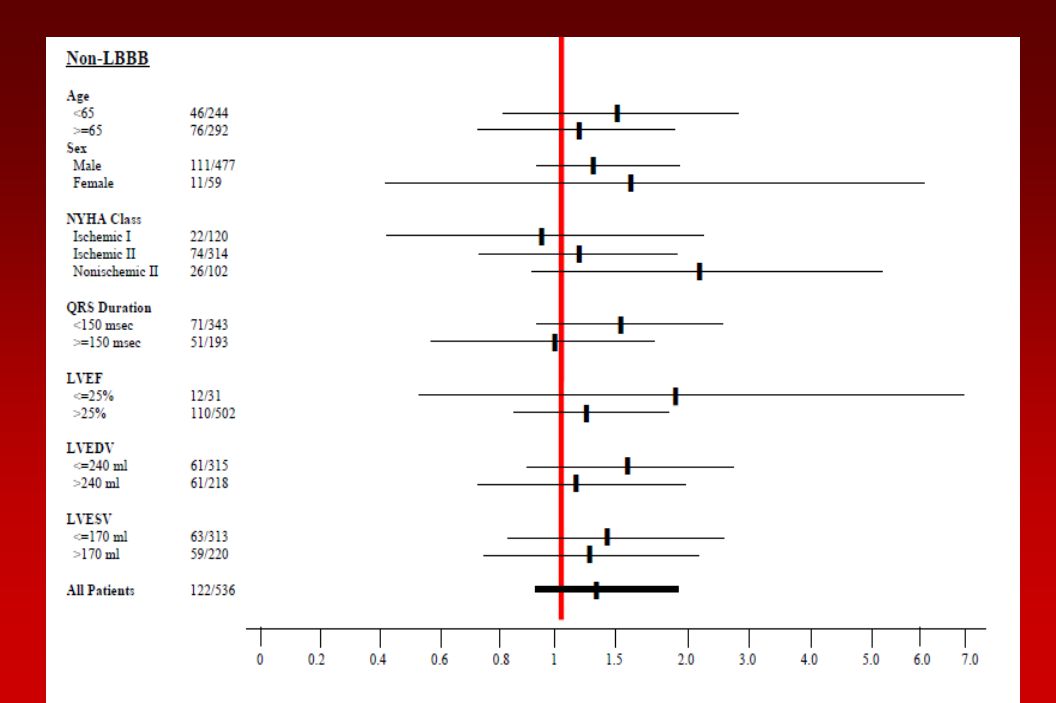
Cumulative Probability of Heart Failure (HF) Event or Death by Treatment (CRT-D vs. ICD only) in patients with LBBB and Non-LBBB QRS Pattern in MADIT-CRT Patients LBBB Non-LBBB

13
Cumulative Probability of Heart Failure (HF) Event or Death by Treatment (CRT-D vs. ICD only) in patients with RBBB and IVCD QRS Pattern in MADIT-CRT Patients RBBB IVCD

14
Cumulative Probability of VT/VF or Death by Treatment (CRT-D vs
Cumulative Probability of VT/VF or Death by Treatment (CRT-D vs. ICD only) in patients with LBBB and Non-LBBB QRS Pattern in MADIT-CRT Patients LBBB Non-LBBB
 in patients with LBBB and Non-LBBB QRS Pattern in MADIT-CRT Patients. LBBB. Non-LBBB.")
15
Cumulative Probability of Death by Treatment (CRT-D vs
Cumulative Probability of Death by Treatment (CRT-D vs. ICD only) in patients with LBBB and Non-LBBB QRS Pattern in MADIT-CRT Patients LBBB Non-LBBB
 in patients with LBBB and Non-LBBB QRS Pattern in MADIT-CRT Patients. LBBB. Non-LBBB.")
16
Hazard Ratios for Clinical Endpoints by QRS Morphology
LBBB n=1,281 Non-LBBB n=536 P value for Inter- action Heart Failure Event HR 0.47 1.24 or Death 95% CI 0.37,0.61 0.85,1.81 P value <0.001 0.257 0.41 1.23 0.31,0.54 0.76,1.68 0.559 Death 0.75 1.79 0.49,1.16 0.90,3.57 0.196 0.097 0.037 * The model adjusted for sex, ischemic or nonischemic cardiomyopathy, prior hospitalizations for heart failure, ejection fraction, QRS>150, left ventricular ejection fraction, left ventricular end-systolic volume.

17
Hazard Ratios for Clinical Endpoints by QRS Morphology
LBBB n=1,281 Non-LBBB n=536 P value for Inter- action VT/VF HR 0.67 1.11 95% CI 0.52,0.87 0.77,1.60 P value 0.002 0.574 0.028 VF 0.54 1.24 0.33,0.87 0.58,2.66 0.011 0.585 0.070 VT/VF/Death 0.69 1.21 0.55,0.87 0.87,1.69 0.254 0.006 * The model adjusted for sex, ischemic or nonischemic cardiomyopathy, prior hospitalizations for heart failure, ejection fraction, QRS>150, left ventricular ejection fraction, left ventricular end-systolic volume.

18
Hazard Ratios for Primary and Secondary Endpoints by QRS Morphology in MADIT-CRT
* * * * *p<0.05

19
Hazard Ratios for Primary Endpoint by QRS Morphology and Duration by Gender
Males Females n HR P value n HR P value QRS Duration <140 ms ms ms ≥180 ms QRS Morphology LBBB* < <0.001 Non-LBBB RBBB NA IVCD * p=0.006 for interaction comparing HR = 0.56 in males vs. HR = 0.25 in females

22
Mean Change in Echocardiographic Parameters from Enrollment to 12 months in CRT-D Patients
* * p<0.001 when comparing LBBB and Non-LBBB patients (all changes within subgroups were significant) * *
 * *")
23
Conclusions Heart failure patients with NYHA class I or II and ejection fraction ≤30% who present with LBBB derive substantial benefit from CRT-D: reduction in heart failure progression and reduction in the risk of ventricular tachyarrhythmias. No evidence of CRT-D benefit was observed in patients with Non-LBBB QRS pattern: RBBB or IVCD regardless of their QRS duration. Beneficial effect of CRT-D in LBBB patients was observed in all studied subjects: males and females, ischemic and non-ischemic, QRS>150 and QRS<150 ms.

Similar presentations




 Arthur J. Moss, MD for the MADIT-RIT Executive Committee AHA Late Breaking Trials November.>")










 Implantation indications and outcomes Guy Amit, MD; Mahmoud Suleiman, MD; Mark Kazatsker,>")



