Download presentation
Presentation is loading. Please wait.

1
Physiology of the Newborn
Respiratory Changes

2
Circulatory Changes Anatomic changes:
Umbilical arteries and vein contract and close. Ductus arteriosus close within 24 hours. Ductus arteriosus and ductus venosus are converted to fibrous tissue (ligaments ) within months. When the pressure in the left atrium exceeds than that of right atrium Formen Ovale closes.
 within months. When the pressure in the left atrium exceeds than that of right atrium Formen Ovale closes.")
5
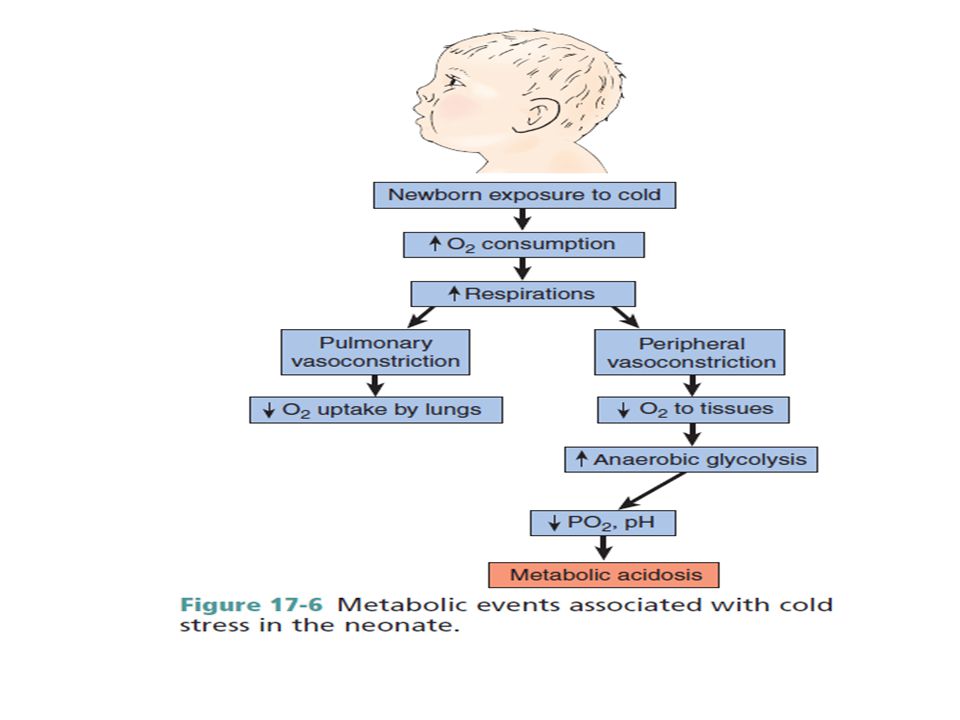
Basal Metabolism Surface area of the infant is large in comparison with body surface. Basal metabolism per kg of body is higher than that of adult. Caloric requirements are high (117 calories \kg day).
.")
6
Renal function At birth the kidney’s function 30 % - 50% of the adult’s capacity and cannt concentrate urine. Term newborns are unable to adequately concentrate urine (reabsorb water back into the blood). This alteration may lead to an inappropriate loss of substances such as amino acids and glucose. Neonate usually voids immediately after birth or within few hours, but it may take up to 24 hours. Anuria should be reported. Increase uric acid will stain in the diaper. Not functioning well yet in maintaining acid-base balance. GFR rapidly increases during the first 4 months, but reaches adult’s function after 2 years.
. This alteration may lead to an inappropriate loss of substances such as amino acids and glucose. Neonate usually voids immediately after birth or within few hours, but it may take up to 24 hours. Anuria should be reported. Increase uric acid will stain in the diaper. Not functioning well yet in maintaining acid-base balance. GFR rapidly increases during the first 4 months, but reaches adult’s function after 2 years.")
7
Hepatic Function Limited function
Decrease ability to conjugate bilirubin will lead to jaundice. Occurs in approximately 60% of full-term infants and in up to 80% of preterm infants (becomes visible when the total serum bilirubin level is greater than 5 mg to 7 mg/dL) Physiologic jaundice may start 1-2 days after birth, peak at 5-7 days, & decline after days. Elevated blood levels of unconjugated bilirubin can be toxic and result in kernicterus
 Physiologic jaundice may start 1-2 days after birth, peak at 5-7 days, & decline after days. Elevated blood levels of unconjugated bilirubin can be toxic and result in kernicterus.")
9
Decrease ability to regulate glucose will lead to hypoglycemia

10
Endocrine Function Disturbances are most often related to maternally provided hormones which can cause the following: Vaginal discharge \ bleeding in female infant. Enlargement of mammary glands in both sexes. Disturbance related to maternal endocrine pathology (D. M)
")
11
GI system Neonate’s stomach capacity increases from 6 ML/kg to 90 ML by end of first week. Low amylase, lipase and bile acids = difficulty in fat digestion. No salivation for the first 3 months. Cardiac sphincter is immature (leads to regurgitation) Small intestines are long First meconium stool within hours of life Absence of a bowel movement by 72 hours of age may be indicative of an obstructive bowel problem.
 Small intestines are long. First meconium stool within hours of life. Absence of a bowel movement by 72 hours of age may be indicative of an obstructive bowel problem.")
13
Immunological Adaptation
IgG is the only immunoglobulin able to pass through the placenta before birth. After birth, vaccination to tetanus, diphtheria, smallpox, measles, mumps, poliomyelitis. Preterm infants born before 34 weeks of gestation are at a greater risk for infection. Colostrum and breast milk are important sources of IgA

14
Posture

15
Milia enlarged sebaceous glands on face, decreased by 2 weeks. (small white papules or sebaceous cysts on the infant’s face that resemble pimples)
 .")
16
Mangolian spots are areas that appear gray, dark blue, or purple and are most commonly located on the back and buttocks, although they may also be found on the shoulders, wrists, forearms, and ankles

17
Head Caput succedaneum: swelling of soft tissue of the scalp.
Cephalhematoma: subperiosteal hemorrhage. Molding: overlapping of skull bones. Examine symmetry of facial movement. Head circumference: cm (2 cm larger than chest). Fontanels: (enlarged = increased intracranial pressure), (sunken = dehydration). Size of fontanels : (posterior 2 – 3 months) ( anterior months ).
. Fontanels: (enlarged = increased intracranial pressure), (sunken = dehydration). Size of fontanels : (posterior 2 – 3 months) ( anterior months ).")
18
Nursing Care of Newborn
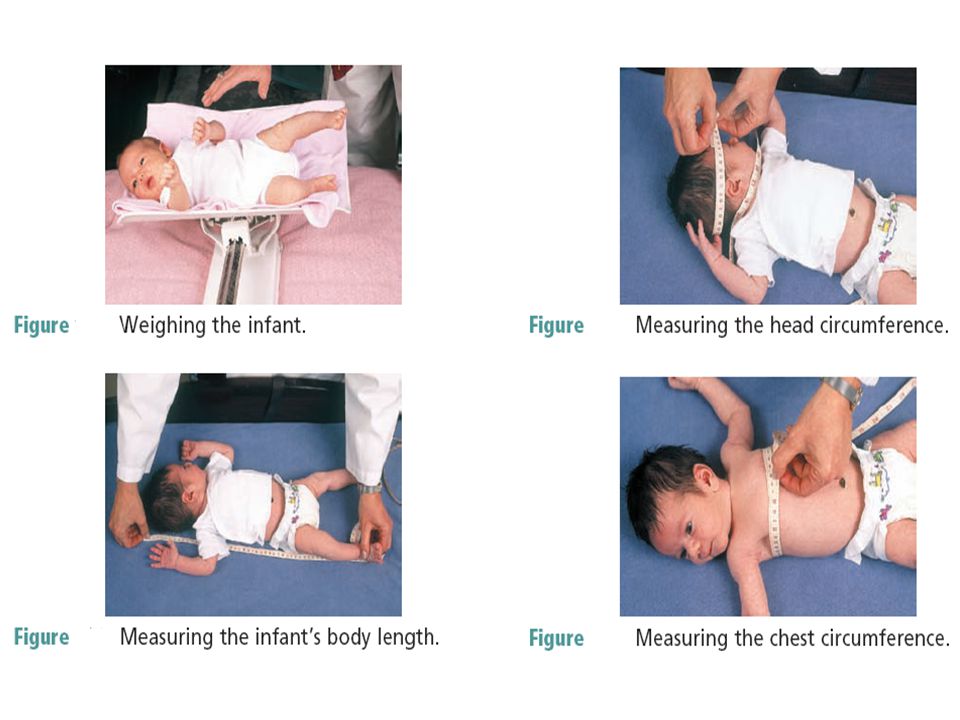
Cleansing and assessment: Weighing and measuring: Cord care: Clothing and cover: Positioning and environment: Recording and identifying Feeding and rest: Discharge planning

Similar presentations



















 eustachian tubes (wider and horizontal) increase amount of lymph tissue, especially in the pharynx.>")

