Download presentation
Presentation is loading. Please wait.

1
Preventing Surgical Site Infections in the OR
Kerri A. Thom, MD, MS Assistant Professor, UM School of Medicine

2
Nothing to Disclose

3
Key Point Up to 60% of surgical site infections may be preventable and there are multiple strategies aims at reducing infection

4
Key Points – SSI Prevention
Up to 60% of SSI are preventable Antibiotic prophylaxis is very important Be aware of your own bioburden Be aware of impact of traffic/door openings

5
Key Points Surgical antimicrobial prophylaxis is the most important intervention in the prevention of SSI Essential elements include: Selection of appropriate agent Timing (within 1 hour of incision) Dose (weight-based, re-dosing) Minimizing adverse events
 Dose (weight-based, re-dosing) Minimizing adverse events.")
6
Objectives Recognize modifiable risk factors for surgical site infection Provide safe care by applying key measures to preventing infections in the OR Optimize antibiotic prophylaxis by selecting the most appropriate agent and giving the optimal dose at the optimal time

7
Overview Background Antibiotic Prophylaxis, What Matters
Modifiable risks for SSI Antibiotic Prophylaxis, What Matters Agent, dose, time Other important measures Optimizing modifiable risk factors Use of the surgical checklist Hand hygiene Limiting traffic and door openings

8
Surgical Site Infections (SSI)
Most Common Healthcare infection1 21% of all HAIs 11%, BSI HAP 14% 20%, SSI 36%, UTI CLABSI 14% 22%, Other 11%, PNA Magill S et al. N Engl J Med, 2014

9
Surgical Site Infections (SSI)
Most Common Healthcare infection1 21% of all HAIs 11%, BSI 15 million inpatient surgeries per year HAP 14% 20%, SSI 36%, UTI CLABSI 14% 22%, Other 11%, PNA Magill S et al. N Engl J Med, 2014

10
Surgical Site Infections (SSI)
Most Common Healthcare infection1 21% of all HAIs 11%, BSI 15 million inpatient surgeries per year 2-5% ( K) develop SSI HAP 14% 20%, SSI 36%, UTI CLABSI 14% 22%, Other 11%, PNA Magill S et al. N Engl J Med, 2014
 develop SSI. HAP. 14% 20%, SSI. 36%, UTI. CLABSI. 14% 22%, Other. 11%, PNA. Magill S et al. N Engl J Med,")
11
Surgical Site Infections (SSI)
Most Common Healthcare infection1 21% of all HAIs Up to 55% of SSIs are preventable! 11%, BSI HAP 14% 20%, SSI 36%, UTI CLABSI 14% 22%, Other 11%, PNA 1Magill S et al. N Engl J Med, Umscheid et al. Infect Control Hosp Epidemiol, 2011

12
Surgical Site Infections (SSI)
Prolong hospital stay (7-10 days) Increased Mortality Risk of death, 2-11 times greater 77% of deaths are attributable to SSI More expensive than other complications (e.g., sternal wound infections most expensive complication of CABG) 1/3 of these are deep/organ space Kirckland et al, Infect Control Hosp Epi, 1999 Managram et al, Infect Control Hosp Epi, 1999 Hollenbeak et al, Chest, 2000 Wenzel et al, Clin Infect Dis, 2007
 Increased Mortality. Risk of death, 2-11 times greater. 77% of deaths are attributable to SSI. More expensive than other complications (e.g., sternal wound infections most expensive complication of CABG) 1/3 of these are deep/organ space. Kirckland et al, Infect Control Hosp Epi, 1999 Managram et al, Infect Control Hosp Epi, 1999 Hollenbeak et al, Chest, 2000 Wenzel et al, Clin Infect Dis,")
13
Pathogenesis SSI Microbial Characteristics Host Characteristics
e.g. Virulence, Dose SSI Complex relationship between microbial contamination and patient/surgical characteristics Host Characteristics Surgical Characteristics e.g. Duration, Implant e.g. Host Defense, Immunity Anderson. Infect Dis Clinics North Am 2011

14
Microbial Characteristics
Pathogenesis Microbial Characteristics e.g. Virulence, Dose SSI Microbial contamination of the wound is a necessary step! The risk is greatest when the wound is open (e.g. commonly at the time of surgery) Host Characteristics Surgical Characteristics e.g. Duration, Implant e.g. Host Defense, Immunity Anderson. Infect Dis Clinics North Am 2011
 Host Characteristics. Surgical Characteristics. e.g. Duration, Implant. e.g. Host Defense, Immunity. Anderson. Infect Dis Clinics North Am")
15
Sources of Microbial Contamination
Endogenous Exogenous ADD PICTURES HERE ENDOGENOUS – PATIENT EXOGENOUS – SURIGCAL HAND HOLDING INTRUMENT Altemeier, Surg Clin North Am 1968 Berkelman, JAMA 1982 Bassett, Lancet 1970 Clegg, J Infect Dis 1983 Gartenberg, N Engl J Med 1978 Most Common Gram-positive (Skin Flora) Air, Instruments, etc… Post-operative Dressing
 Air, Instruments, etc… Post-operative Dressing.")
16
Organisms Causing SSI Staphylococcus aureus 30.0% Coag-negative Staphylococci 13.7% Enterococcus spp. 11.2% Escherichia coli 9.6% Pseudomonas aeruginosa 5.6% Rest: Other gram negative bacteria, Candida Point out that the most important thing to remember is that they causative organisms typically reflect the normal flora and common colonizing organisms of the surgical site Hidron, Infect Control Hosp Epidemiol 2008

17
SSI Patient Post-Operative Surgery Patient Age Undernutrition
Infection at Remote Site Prolonged Pre-op Stay Prior Operations Immunesuppression Cancer Diabetes Obesity Smoking Surgical Wound Class Prophylactic Antibiotics Pre-op Cleansing Pre-op Screening Pre-op Hair Removal Surgical Technique Surgical Duration OR environment Hypothermia SSI Post-Op Glucose Control Wound Care

18
Prophylactic Antibiotics
Use for surgeries that require: entering a hollow viscus, insertion of prosthesis, or if development of SSI would pose catastrophic risk Point out that the most important thing to remember is that they causative organisms typically reflect the normal flora and common colonizing organisms of the surgical site One of the most important interventions to prevent SSI

19
The Ideal Agent?

20
No impact on Microbiome
The Ideal Agent? Safe Effective No impact on Microbiome

21
Antibiotic Selection Activity against expected pathogens
Favorable safety profile (toxicities, allergies) Favorable cost profile Point out that the most important thing to remember is that they causative organisms typically reflect the normal flora and common colonizing organisms of the surgical site
 Favorable cost profile. Point out that the most important thing to remember is that they causative organisms typically reflect the normal flora and common colonizing organisms of the surgical site.")
22
Dose Weight-based Cefazolin 2 gm for all RCT of 1 versus 2 gm
1 gm decreased serum/tissue concentrations, below necessary MICs Point out that the most important thing to remember is that they causative organisms typically reflect the normal flora and common colonizing organisms of the surgical site Forse, Surg, 1989

23
Timing Successful prophylaxis relies on drug availability
at the operative site during time of contamination Begin administration within 1 hour of cut time 2 hr for Vanc/FQ Complete administration by incision Re-dose at 3 hour intervals (and/or blood loss) Stop antibiotics after procedure Point out that the most important thing to remember is that they causative organisms typically reflect the normal flora and common colonizing organisms of the surgical site
 Stop antibiotics after procedure. Point out that the most important thing to remember is that they causative organisms typically reflect the normal flora and common colonizing organisms of the surgical site.")
24
Timing SSI rates corresponding to the temporal association between administration of antibiotics and the start of surgery 2847 pts elective clean or clean/contaminated surgeries Classen NEJM, 1992

25
Timing Association between the timing of prophylaxis and incidence of SSI following Cardiac Surgery, THA/TKA, Hysterectomy 4472 patients Steinberg JP, Ann Surg, 2009

26
Timing Successful prophylaxis relies on drug availability
at the operative site during time of contamination Begin administration within 1 hour of cut time 2 hr for Vanc/FQ Complete administration by incision Re-dose at 3 hour intervals (and/or blood loss) Stop antibiotics after procedure Point out that the most important thing to remember is that they causative organisms typically reflect the normal flora and common colonizing organisms of the surgical site
 Stop antibiotics after procedure. Point out that the most important thing to remember is that they causative organisms typically reflect the normal flora and common colonizing organisms of the surgical site.")
27
National QI Initiatives
SCIP (Surgical Care Improvement Project) Appropriate selection Within 1 hour Stopped within 24 hours CMS Reporting SSI after CABG, THA, TKA Soon…SSI after Colorectal and Hysterectomy
 Appropriate selection. Within 1 hour. Stopped within 24 hours. CMS Reporting. SSI after CABG, THA, TKA. Soon…SSI after Colorectal and Hysterectomy.")
29
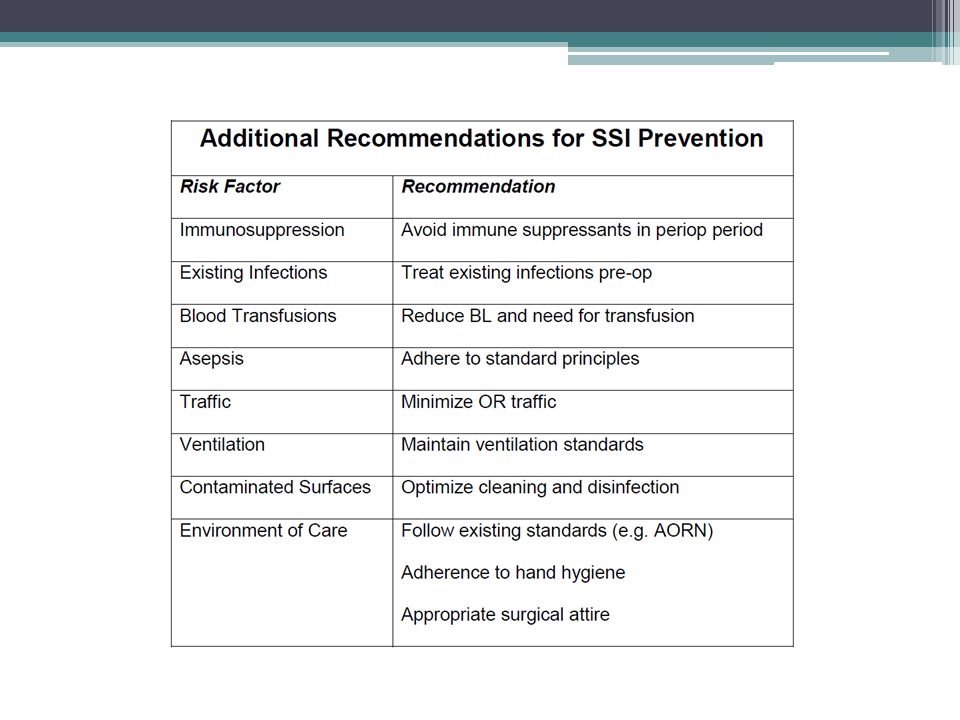
Other Infection Prevention Measures

30
(based on WHO Surgical Checklist)
Use an OR Checklist (based on WHO Surgical Checklist)
")
31
Surgical Checklist

33
Results of Starting Checklist
Variable % Decrease p value Total disruptions/case 47 <0.01 Miscommunications/case Time circulator gone Henrickson. J Amer Coll Surgeons 2009; 208:

34
Does the Checklist Impact Mortality?
22 item checklist modeled on WHO 25,513 patients followed Record of checklist completion: Not done Partial - at least 1 of 22 done Completed - all done van Klei. Ann Surg 2012; 255: 44-9

35
Checklist Completion and Mortality
Adjusted Odds Ratio Mortality All patients 0.85 ( ) van Klei. Ann Surg 2012; 255: 44-9
 van Klei. Ann Surg 2012; 255:")
36
Checklist Completion and Mortality
Adjusted Odds Ratio Mortality All patients 0.85 ( ) Completed 0.44 ( ) Partial 1.09 ( ) Not done 1.16 ( van Klei. Ann Surg 2012; 255: 44-9
 Completed 0.44 ( ) Partial 1.09 ( ) Not done 1.16 ( van Klei. Ann Surg 2012; 255:")
39
Reducing our own bioburden
Hand hygiene (and/or surgical scrub) Appropriate attire Including covering hair Monitor for skin lesions
 Appropriate attire. Including covering hair. Monitor for skin lesions.")
40
Hand Hygiene In/Out of Room Multiple opportunities during case

41
Healthcare worker attire is not sterile and is commonly contaminated with potentially pathogenic bacteria both in the course of duties at work and in care, maintenance and wearing of attire outside the hospital setting. Studies consistently show that 25 to 50% of hospital ‘scrubs’ are contaminated with potentially pathogenic bacteria such as MRSA and Acinetobacter baumannii. At the University of Maryland Medical Center 30% of scrubs of ICU nurses are contaminated with these bacteria (unpublished data not shown below). Additional data from UMMC has shown that after caring for patients with a multidrug-resistant organism, healthcare workers acquire these bacteria on their clothing between 20 to 40% of the time. Researchers at VCU have shown in a simulated setting that bacteria contaminating healthcare worker white coats can easily transfer to pig skin. Further, researchers at U Miami have shown that contamination of healthcare hands, which are known to be the primary vector of transmission of bacteria to patients, is correlated with contamination of attire (scrubs and white coats). These and other studies suggest that attire, and in particular contaminated attire, do play a role in transmission of bacteria to patients in the hospital setting. In the OR setting, several studies below are worth noting demonstrating that the bacteria that contaminate OR scrubs worn under sterile gowns can penetrate through these gowns and be cultured, which in turn can then be spread via surgeon hands to the patient. Further, bacteria on the scrubs can be found in air samples in the OR. In a very interesting report of an outbreak of Gordonia bronchialis sternal wound infections, investigators identified a single nurse whose clothing and washing machine were contaminated with G. bronchialis. Removal of potential pathogenic microorganisms during the laundering process has been shown to be reliant on several factors including water temperature, appropriate use of detergent and ironing. Healthcare worker clothing laundered at home is more likely to be contaminated with potential bacteria than attire laundered by a healthcare facility (or third party). In one study, investigators found that scrubs were contaminated 39% of the time at the beginning (compared to 50% of the time at the end of a shift) even when considered “clean” by the healthcare worker. At a study done at UMMC, white coats of surgeons and internists were contaminated with S. aureus 22.8% of the time, and there was a higher portion of coats contaminated if the scrubs were cleaned at home (59%) compared to cleaning in the hospital laundry facility (29%). Another study showed that hospital laundered scrubs had significantly fewer bacterial counts than home laundered scrubs (p < 0.01). And a separate study demonstrated that ‘clean’ re-useable scrubs laundered at home had higher bacterial colony count than scrubs laundered by third party facility or hospital and these ‘clean’ scrubs were more similar to ‘worn” scrubs with respect to bacterial counts.
. In one study, investigators found that scrubs were contaminated 39% of the time at the beginning (compared to 50% of the time at the end of a shift) even when considered clean by the healthcare worker. At a study done at UMMC, white coats of surgeons and internists were contaminated with S. aureus 22.8% of the time, and there was a higher portion of coats contaminated if the scrubs were cleaned at home (59%) compared to cleaning in the hospital laundry facility (29%). Another study showed that hospital laundered scrubs had significantly fewer bacterial counts than home laundered scrubs (p < 0.01). And a separate study demonstrated that ‘clean’ re-useable scrubs laundered at home had higher bacterial colony count than scrubs laundered by third party facility or hospital and these ‘clean’ scrubs were more similar to ‘worn scrubs with respect to bacterial counts.")
42
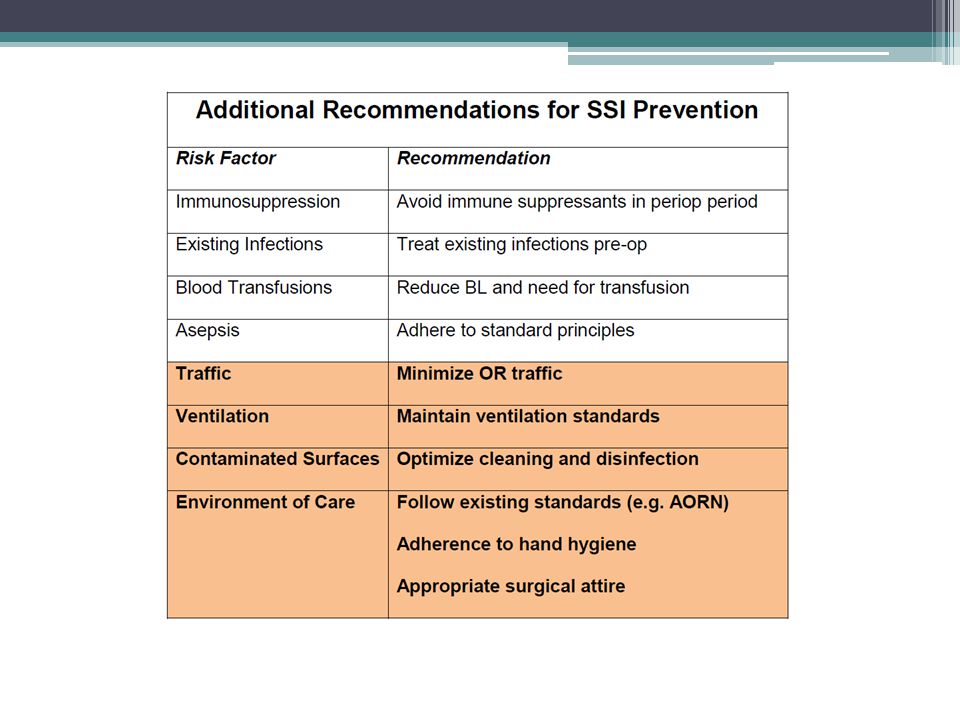
Managing Air Flow

43
Microbial Air Counts and OR Traffic
68% of the variance in total CFU/m3 (p = 0.001) explained by Traffic flow (door openings) Number of persons (clutter) in the OR Procedure duration In addition, the data showed a strongly positive correlation between the A weaker, yet still positive correlation between AE Andersson et al. AJIC 2012, Jan 28 epublished
 explained by. Traffic flow (door openings) Number of persons (clutter) in the OR. Procedure duration. In addition, the data showed a strongly positive correlation between the. A weaker, yet still positive correlation between. AE Andersson et al. AJIC 2012, Jan 28 epublished.")
46
Door Openings 284 operations 22 pts had SSI: Risk factors for SSI:
Mastectomy (n = 5; 2.8%) Colon resection (n = 16; 21.6%) Aorta reconstruction (n = 1; 2.8%) Risk factors for SSI: Wound class: p < 0.001 Emergency procedure: p = 0.001 Door openings/hour 0-6 vs > 6: p = 0.02 prospective surveillance of SSI and implementation of bundle elements: timing of perioperative prophy abx, hygiene disicipline = door openings, appropriate hair removal, periop normothermia FJ Prakken, et al. NED TIJDSCHR GENEESKD. 2011;155:A3269
 Colon resection (n = 16; 21.6%) Aorta reconstruction (n = 1; 2.8%) Risk factors for SSI: Wound class: p < Emergency procedure: p = Door openings/hour 0-6 vs > 6: p = prospective surveillance of SSI and implementation of bundle elements: timing of perioperative prophy abx, hygiene disicipline = door openings, appropriate hair removal, periop normothermia. FJ Prakken, et al. NED TIJDSCHR GENEESKD. 2011;155:A3269.")
47
Reasons for Door Openings
177 (33.5%) = necessary 40 = expert consultations 137 = supplies & equipment 184 (35.7%) = semi-necessary 76 = surgical team members entering or leaving 134 = breaks 168 (31.8%) = unnecessary 30 = logistics, like planning other operations 45 = social 93 = no detectable reason AE Andersson et al. AJIC 2012, Jan 28 epublished
 = necessary. 40 = expert consultations. 137 = supplies & equipment. 184 (35.7%) = semi-necessary. 76 = surgical team members entering or leaving. 134 = breaks. 168 (31.8%) = unnecessary. 30 = logistics, like planning other operations. 45 = social. 93 = no detectable reason. AE Andersson et al. AJIC 2012, Jan 28 epublished.")
48
Door Openings Number of door openings varied by specialty
19-50 door openings/hour OR doors open: ~20 seconds/opening 15-20 min/hour Requests for information > breaks (~25%) > supplies (~20%) RJ Lynch, et al. Am J Med Qual 2009;24;45-52
 > supplies (~20%) RJ Lynch, et al. Am J Med Qual 2009;24;")
49
Strategies to Reduce Door Opening

50
Key Point Up to 60% of surgical site infections may be preventable and there are multiple strategies aims at reducing infection

51
Key Points – SSI Prevention
Up to 60% of SSI are preventable Antibiotic prophylaxis is very important Be aware of your own bioburden Be aware of impact of traffic/door openings

52
Key Points Surgical antimicrobial prophylaxis is the most important intervention in the prevention of SSI Essential elements include: Selection of appropriate agent Timing (within 1 hour of incision) Dose (weight-based, re-dosing) Minimizing adverse events
 Dose (weight-based, re-dosing) Minimizing adverse events.")
53
WASH YOUR HANDS! ANY QUESTIONS?

Similar presentations




: What the Direct Caregiver Should Know>")

>")












 after Colorectal Surgery? A Lunch Symposium held during SISNA 2007 at the Westin Harbour Castle Hotel.>")

