Download presentation
Presentation is loading. Please wait.

1
Does Africa need a rectal microbicide? IRMA and AVAC presentation 27 September 2011 Salim S. Abdool Karim Pro Vice-Chancellor (Research), University of KwaZulu-Natal Director: CAPRISA Professor of Clinical Epidemiology, Columbia University Adjunct Professor of Medicine, Cornell University Associate Member, The Ragon Institute of MGH, MIT and Harvard University
, University of KwaZulu-Natal Director: CAPRISA Professor of Clinical Epidemiology, Columbia University Adjunct Professor of Medicine, Cornell University Associate Member, The Ragon Institute of MGH, MIT and Harvard University.")
2
Outline The HIV epidemic in Africa Prevalence of HIV in MSM Rates of bisexual partnerships Prevalence of anal sex Risk factors for unprotected anal intercourse A new hope… Conclusion

3
Age Group (Years) HIV Prevalence (N=1237) ≤1610.6% 17-1821.3% 19-2033.0% 21-2244.3% 23-2451.1% HIV prevalence in pregnant women in rural Vulindlela, South Africa (2005-2008)
 HIV Prevalence (N=1237) ≤1610.6% % % % % HIV prevalence in pregnant women in rural Vulindlela, South Africa ( )")
4
The HIV epidemic in Africa: HIV prevalence by age and sex in four African countries Kenya Cameroon Lesotho Malawi

5
Population-level data on MSM are rare same-sex relations are criminalized in 37 out of 54 African countries and are punishable by death in four of these. Recent studies on MSM sex workers indicates widespread existence of MSM groups in Africa Mombasa, Kenya: ± 739 MSM sex workers working in the city Johannesburg, South Africa: ± 496 MSM sex workers (95% CI 437–555) working in city on any given Saturday night The HIV epidemic in Africa: The hidden side African Men who have Sex with Men
 working in city on any given Saturday night The HIV epidemic in Africa: The hidden side African Men who have Sex with Men.")
6
The HIV epidemic in Africa: A mosiac of both heterosexual and homosexual HIV transmission Source: UNAIDS. 2006 Report on the global AIDS epidemic. UNAIDS, Geneva

10
HIV prevalence among MSM in Africa HIV prevalence in MSM: Range: 6.2% in Egypt to 30.9% in Cape Town Source: Griensven et al. Current Opinion in HIV and AIDS 2009, 4:300–307

11
Estimates of HIV prevalence among MSM in sub-Saharan Africa YearHIV prevalence (95%CI)n Kenya2002–200510.6% (9–13)780 Tanzania200712.3% (10–15)509 Nigeria200613.4% (11–15)1125 South Africa2003–200514.1% (12–17)728 Malawi200821.4% (16–28)201 Senegal200721.8% (18–25)501 Zambia200633% (29–37)641 Adapted from: Smith AD, et al. Men who have sex with men and HIV/AIDS in sub-Saharan Africa. Lancet 2009; 374: 416–22

12
In South Africa Soweto Men's Study (N=378) HIV infection associated with: 6-9 partners (past 6 months) (OR 5.7, CI 4.0-8.2) any unprotected anal sex* (OR 4.4, CI 3.5-5.7) *past 6 months In Kenya Prevalent HIV infection in MSM (n=285) was associated with: recent receptive anal sex (OR, 6.1; CI, 2.4-16) exclusive sex with men (OR, 6.3; CI, 2.3-17), Factors associated with HIV infection among MSM
 HIV infection associated with: 6-9 partners (past 6 months) (OR 5.7, CI ) any unprotected anal sex* (OR 4.4, CI ) *past 6 months In Kenya Prevalent HIV infection in MSM (n=285) was associated with: recent receptive anal sex (OR, 6.1; CI, ) exclusive sex with men (OR, 6.3; CI, ), Factors associated with HIV infection among MSM")
14
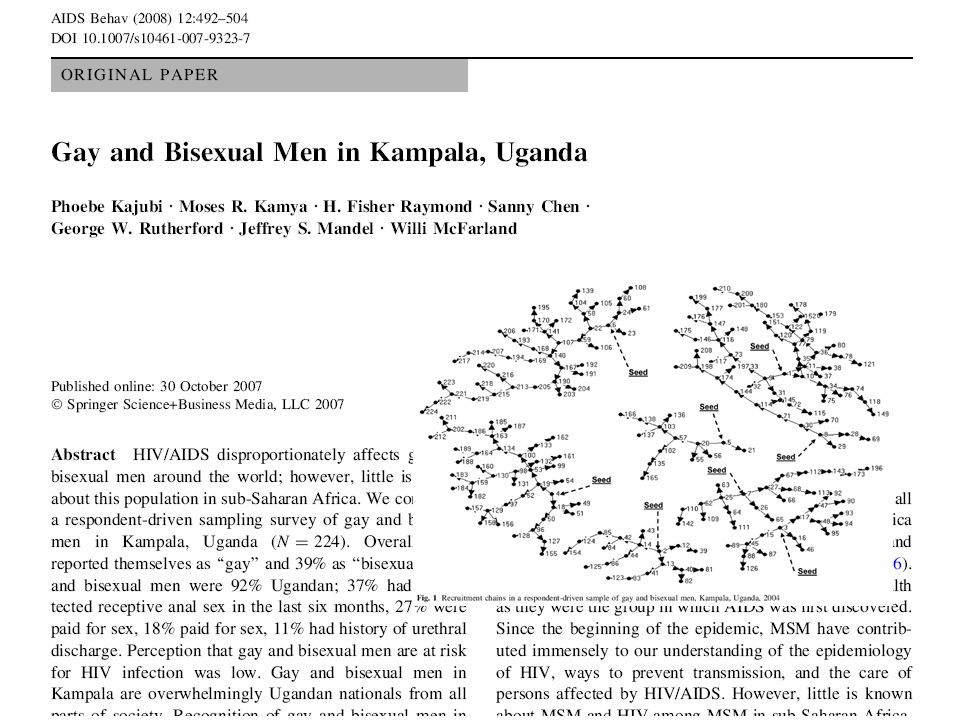
In Malawi, Namibia and Botswana cross-sectional study of MSM (n=537) showed: 34.1% were married or had a stable female partner, 53.7% had both male and female sexual partners In Egypt Survey among MSM (n=73) showed: 73.3% of MSM reported being bisexual In Kampala, Uganda Survey among MSM (n=224) reported: 39% self-identified as "bisexual” Rates of bisexual partnerships in Africa
 showed: 34.1% were married or had a stable female partner, 53.7% had both male and female sexual partners In Egypt Survey among MSM (n=73) showed: 73.3% of MSM reported being bisexual In Kampala, Uganda Survey among MSM (n=224) reported: 39% self-identified as bisexual Rates of bisexual partnerships in Africa")
15
Studies providing estimates of heterosexual sex among MSM (2003–2007) Source: Caceres, C. F., et al. (2008). Sex Transm Infect 84 Suppl 1: i49-i56. Global studies (range of results) African studies (range of results) Heterosexual sex in MSM, lifetime20 (25–86)3 (41–86) Heterosexual sex in MSM, last year16 (8–98)2 (50–69) Proportion of MSM who are married16 (3–42)2 (8–15)
. Sex Transm Infect 84 Suppl 1: i49-i56. Global studies (range of results) African studies (range of results) Heterosexual sex in MSM, lifetime20 (25–86)3 (41–86) Heterosexual sex in MSM, last year16 (8–98)2 (50–69) Proportion of MSM who are married16 (3–42)2 (8–15).")
17
In Cape Town, South Africa: Anonymous surveys of 2593 men and 1818 women: Anal intercourse (past 3 months): Men = 14%; Women = 10% Condom use during anal intercourse: Men = 67%; Women = 50% Kalichman et al (2009) In KwaZulu-Natal, South Africa: 42% of truck drivers (n=320) reported anal sex with female sex workers Ramjee et al (2002) In Kenya: Survey among FSW (n=147): 40.8% reported ever practising anal intercourse, 30% reported never or rarely using condoms during anal intercourse consistent condom use lower in anal sex than peno-vaginal intercourse Schwandt et al (2006) In Nigeria: anal sex practiced by 12% of public secondary schools students (N= 521) Bamidele et al (2009) Anal intercourse in heterosexual men & women
: Men = 14%; Women = 10% Condom use during anal intercourse: Men = 67%; Women = 50% Kalichman et al (2009) In KwaZulu-Natal, South Africa: 42% of truck drivers (n=320) reported anal sex with female sex workers Ramjee et al (2002) In Kenya: Survey among FSW (n=147): 40.8% reported ever practising anal intercourse, 30% reported never or rarely using condoms during anal intercourse consistent condom use lower in anal sex than peno-vaginal intercourse Schwandt et al (2006) In Nigeria: anal sex practiced by 12% of public secondary schools students (N= 521) Bamidele et al (2009) Anal intercourse in heterosexual men & women")
19
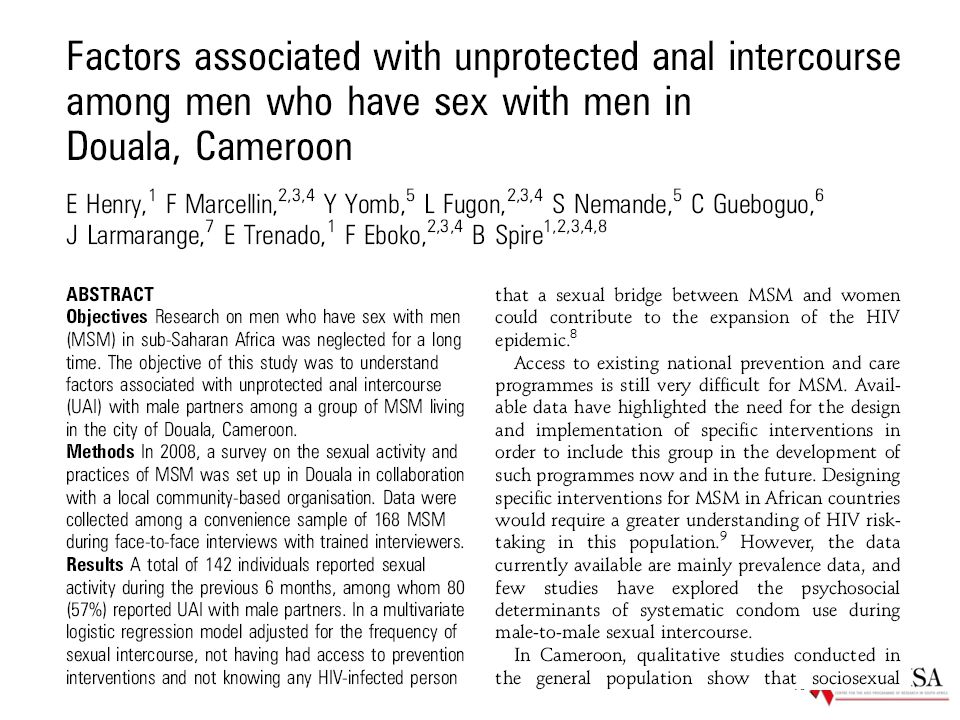
Cameroon: UAI risk increased in those not knowing any HIV-infected person (N=168, OR 1.89) Henry et al (2010) South Africa: UAI risk associated with regular drinking (N=147; OR 4.1) Lane et al. (2008) Uganda: UAI associated with having had an HIV test in the past 6 months (N=215, OR 2.81) Raymond et al (2009) Kenya: UAI linked to poor knowledge of increased HIV risk from UAI (N=425, OR: 1.9) Geibel et al. (2008) Factors associated with unprotected anal intercourse (UAI) in Africa
 Uganda: UAI associated with having had an HIV test in the past 6 months (N=215, OR 2.81) Raymond et al (2009) Kenya: UAI linked to poor knowledge of increased HIV risk from UAI (N=425, OR: 1.9) Geibel et al. (2008) Factors associated with unprotected anal intercourse (UAI) in Africa.")
20
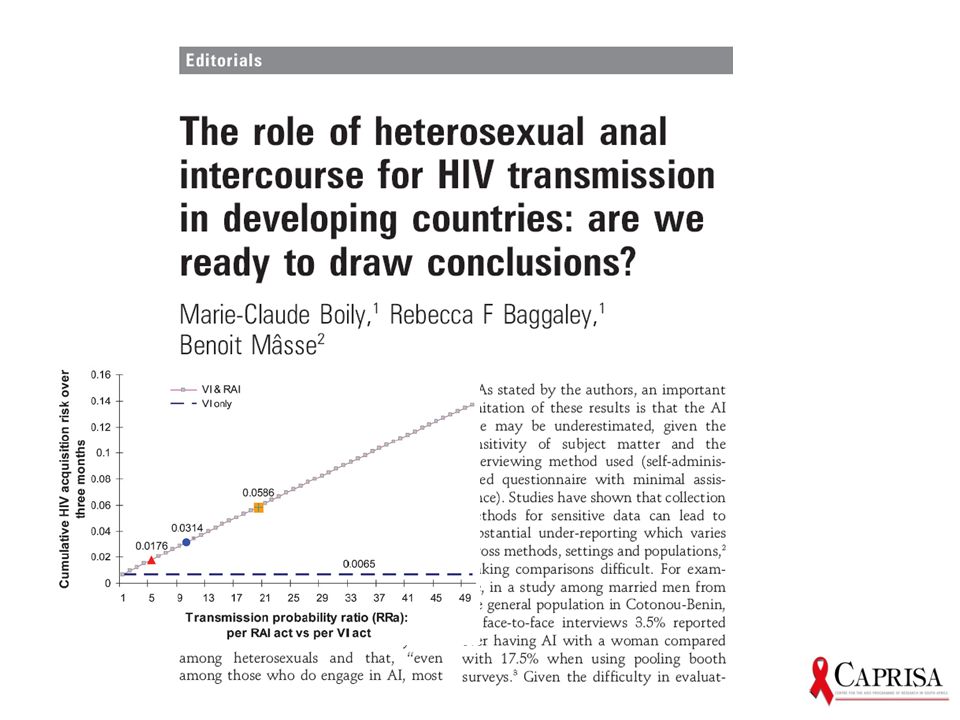
Risks associated with unprotected anal intercourse: HIV transmission Source: Baggaley et al. Int. J. Epidemiol. Advance Access published April 20, 2010

21
A new hope…

22
Stopped for futility Safe but not effective Increased HIV infection Kenya N-9 sponge trial FHI N-9 film trial UNAIDS COL-1492 trial CONRAD CS trial FHI SAVVY trial PopCouncil Carraguard trial HPTN PRO2000 & BufferGel trial 1 st class: Surfactants eg. N9, SAVVY 2 nd class: Polymers eg. PRO2000, Carraguard, Cellulose Sulfate (CS) 3 rd class: ARVs eg. Tenofovir gel CAPRISA 004 Tenofovir gel trial MDP 0.5% PRO2000 trial ‘90 ‘92 ’98 ’00 ‘03 ‘04 ‘04 ’05 ’05 ’07 ’09 ‘11 FHI CS Trial 2% PRO2000 Planned MTN003 –VOICE Tenofovir gel & tablet trial FACTS 001 Tenofovir gel trial CAPRISA 008 Tenofovir gel implementation trial Effective July 2010: Proof of Concept for microbicides IPM dapivarine ring
 3 rd class: ARVs eg. Tenofovir gel CAPRISA 004 Tenofovir gel trial MDP 0.5% PRO2000 trial ‘90 ‘92 ’98 ’00 ‘03 ‘04 ‘04 ’05 ’05 ’07 ’09 ‘11 FHI CS Trial 2% PRO2000 Planned MTN003 –VOICE Tenofovir gel & tablet trial FACTS 001 Tenofovir gel trial CAPRISA 008 Tenofovir gel implementation trial Effective July 2010: Proof of Concept for microbicides IPM dapivarine ring.")
23
23

24
131 infections after randomization 83 in placebo 48 in FTC/TDF Primary HIV analysis (1 May): 44% protection At the end of the study: 42% (95% CI 18%-60%) No effect on HSV-2 TDF-DP drug levels in blood << EC50 for HSV November 2010: Oral PrEP prevents HIV in MSM – iPrEx trial
: 44% protection At the end of the study: 42% (95% CI 18%-60%) No effect on HSV-2 TDF-DP drug levels in blood << EC50 for HSV November 2010: Oral PrEP prevents HIV in MSM – iPrEx trial")
25
CAPRISA 004 and iPrEX trials are in Science’s Top 10 Scientific Breakthroughs in 2010 25

26
May 2011: Proof that ART prevents HIV transmission from infected partners (HPTN 052) - 1763 discordant couples - 13 sites in Africa, America & Asia - ART at CD4 up to 550 vs only <250 - HIV incidence (placebo) = 2.2 per 100pys - 28 matched HIV inf n : 27 in delayed ART - 96% effective (excl. non-matched viruses) - Trial halted early for effectiveness - 1763 discordant couples - 13 sites in Africa, America & Asia - ART at CD4 up to 550 vs only <250 - HIV incidence (placebo) = 2.2 per 100pys - 28 matched HIV inf n : 27 in delayed ART - 96% effective (excl. non-matched viruses) - Trial halted early for effectiveness
 - Trial halted early for effectiveness discordant couples - 13 sites in Africa, America & Asia - ART at CD4 up to 550 vs only <250 - HIV incidence (placebo) = 2.2 per 100pys - 28 matched HIV inf n : 27 in delayed ART - 96% effective (excl. non-matched viruses) - Trial halted early for effectiveness.")
27
July 2011: Oral PrEP prevents HIV transmission in discordant couples (PartnersPrEP) -4,758 HIV serodiscordant couples enrolled -Kenya and Uganda -Daily oral TDF or TDF/FTC or Placebo -HIV incidence (placebo group) = 1.9 per 100pys -78 HIV infections after randomization -18 in TDF arm (62% protection) -13 in FTC/TDF arm (73% protection) -47 Placebo -4,758 HIV serodiscordant couples enrolled -Kenya and Uganda -Daily oral TDF or TDF/FTC or Placebo -HIV incidence (placebo group) = 1.9 per 100pys -78 HIV infections after randomization -18 in TDF arm (62% protection) -13 in FTC/TDF arm (73% protection) -47 Placebo
 -4,758 HIV serodiscordant couples enrolled -Kenya and Uganda -Daily oral TDF or TDF/FTC or Placebo -HIV incidence (placebo group) = 1.9 per 100pys -78 HIV infections after randomization -18 in TDF arm (62% protection) -13 in FTC/TDF arm (73% protection) -47 Placebo -4,758 HIV serodiscordant couples enrolled -Kenya and Uganda -Daily oral TDF or TDF/FTC or Placebo -HIV incidence (placebo group) = 1.9 per 100pys -78 HIV infections after randomization -18 in TDF arm (62% protection) -13 in FTC/TDF arm (73% protection) -47 Placebo")
28
July 2011: Oral PrEP prevents HIV in heterosexual men & women (Botswana TDF2) -1219 heterosexual men & women enrolled -Botswana -Daily oral TDF-FTC -HIV incidence rate (placebo) = 3.1 per 100pys -33 HIV infections after randomization -9 in FTC/TDF arm (63% protection) -24 in Placebo -1219 heterosexual men & women enrolled -Botswana -Daily oral TDF-FTC -HIV incidence rate (placebo) = 3.1 per 100pys -33 HIV infections after randomization -9 in FTC/TDF arm (63% protection) -24 in Placebo
 heterosexual men & women enrolled -Botswana -Daily oral TDF-FTC -HIV incidence rate (placebo) = 3.1 per 100pys -33 HIV infections after randomization -9 in FTC/TDF arm (63% protection) -24 in Placebo heterosexual men & women enrolled -Botswana -Daily oral TDF-FTC -HIV incidence rate (placebo) = 3.1 per 100pys -33 HIV infections after randomization -9 in FTC/TDF arm (63% protection) -24 in Placebo")
29
Clinical trial evidence for preventing sexual HIV transmission – July 2010 Efficacy Study Effect size (CI) Medical male circumcision (Orange Farm, Rakai, Kisumu) 54% (38; 66) HIV Vaccine (Thai RV144) 31% (1; 51) 0% 10 20 30 40 50 60 70 80 90 100% STD treatment (Mwanza) 42% (21; 58)
 Medical male circumcision (Orange Farm, Rakai, Kisumu) 54% (38; 66) HIV Vaccine (Thai RV144) 31% (1; 51) 0% % STD treatment (Mwanza) 42% (21; 58)")
30
Clinical trial evidence for preventing sexual HIV transmission – July 2011 Efficacy Study Effect size (CI) Medical male circumcision (Orange Farm, Rakai, Kisumu) 54% (38; 66) HIV Vaccine (Thai RV144) 31% (1; 51) 0% 10 20 30 40 50 60 70 80 90 100% STD treatment (Mwanza) 42% (21; 58) 39% (6; 60) Microbicide (CAPRISA 004 tenofovir gel) PrEP for MSMs (America’s, Thailand, South Africa) 44% (15; 63) Treatment for prevention (Africa, Asia, America’s) 96% (73; 99) PrEP for heterosexuals (Botswana TDF2) 63% (21; 48) PrEP for discordant couples (Partners PrEP) 73% (49; 85)
 Medical male circumcision (Orange Farm, Rakai, Kisumu) 54% (38; 66) HIV Vaccine (Thai RV144) 31% (1; 51) 0% % STD treatment (Mwanza) 42% (21; 58) 39% (6; 60) Microbicide (CAPRISA 004 tenofovir gel) PrEP for MSMs (America’s, Thailand, South Africa) 44% (15; 63) Treatment for prevention (Africa, Asia, America’s) 96% (73; 99) PrEP for heterosexuals (Botswana TDF2) 63% (21; 48) PrEP for discordant couples (Partners PrEP) 73% (49; 85)")
31
Note: PMTCT, Screening transfusions, Harm reduction, Universal precautions, etc. have not been included – this is focused on reducing sexual transmission Behavioural Intervention -Abstinence -Be Faithful HIV Counselling and Testing Coates T, Lancet 2000 Male Condoms Female Condoms Treatment of STIs Grosskurth H, Lancet 2000 Male circumcision Auvert B, PloS Med 2005 Gray R, Lancet 2007 Bailey R, Lancet 2007 Microbicides for women Abdool Karim Q, Science 2010 Treatment for prevention Donnell D, Lancet 2010 Cohen M, NEJM 2011 Behavioural positive prevention Fisher J, JAIDS 2004 Grant R, NEJM 2010 (MSM) Baeten J, 2011 (Couples) Paxton L, 2011 (Heterosexuals) Oral pre-exposure prophylaxis Post Exposure prophylaxis (PEP) Scheckter M, 2002 Vaccines Rerks-Ngarm S, NEJM 2009 COMBINATION HIV PREVENTION
 Baeten J, 2011 (Couples) Paxton L, 2011 (Heterosexuals) Oral pre-exposure prophylaxis Post Exposure prophylaxis (PEP) Scheckter M, 2002 Vaccines Rerks-Ngarm S, NEJM 2009 COMBINATION HIV PREVENTION.")
32
Note: PMTCT, Screening transfusions, Harm reduction, Universal precautions, etc. have not been included – this is focused on reducing sexual transmission Behavioural Intervention -Abstinence -Be Faithful HIV Counselling and Testing Coates T, Lancet 2000 Male Condoms Female Condoms Treatment of STIs Grosskurth H, Lancet 2000 Male circumcision Auvert B, PloS Med 2005 Gray R, Lancet 2007 Bailey R, Lancet 2007 Microbicides for women Abdool Karim Q, Science 2010 Treatment for prevention Donnell D, Lancet 2010 Cohen M, NEJM 2011 Behavioural positive prevention Fisher J, JAIDS 2004 Grant R, NEJM 2010 (MSM) Baeten J, 2011 (Couples) Paxton L, 2011 (Heterosexuals) Oral pre-exposure prophylaxis Post Exposure prophylaxis (PEP) Scheckter M, 2002 Vaccines Rerks-Ngarm S, NEJM 2009 HIV PREVENTION FOR MSM
 Baeten J, 2011 (Couples) Paxton L, 2011 (Heterosexuals) Oral pre-exposure prophylaxis Post Exposure prophylaxis (PEP) Scheckter M, 2002 Vaccines Rerks-Ngarm S, NEJM 2009 HIV PREVENTION FOR MSM.")
33
MSM and their needs are largely ignored in HIV prevention and treatment efforts in Africa Most AIDS prevention messages are targeted at heterosexual men and women emphasizing the risks of transmission through peno-vaginal sex and not through anal intercourse The needs of the many women who are unable to get men to use condoms in anal sex are ignored Hence the need for a rectal microbicide in Africa… Limitations of current HIV prevention in Africa

34
WHO is preparing to develop guidelines for tenofovir gel implementation for women

35
Conclusion HIV spreading in MSM AND heterosexuals in Africa Unprotected anal sex is a key HIV risk factor Current HIV prevention efforts are unable to contain or reduce the spread of HIV infection thro anal sex Combating HIV is not only about scaling-up proven prevention – but also new prevention technologies A rectal microbicide, as a new HIV prevention technology is urgently needed in Africa for the large number of people practicing anal sex, ie: Men who have Sex with Men Bisexual men Women

Similar presentations







 The End of AIDS Transmission? Robert M Grant, June 2012.>")














