Download presentation
Presentation is loading. Please wait.

1
ORTHODONTIC MANAGEMENT
OF CLEFT LIP AND PALATE PATIENTS

2
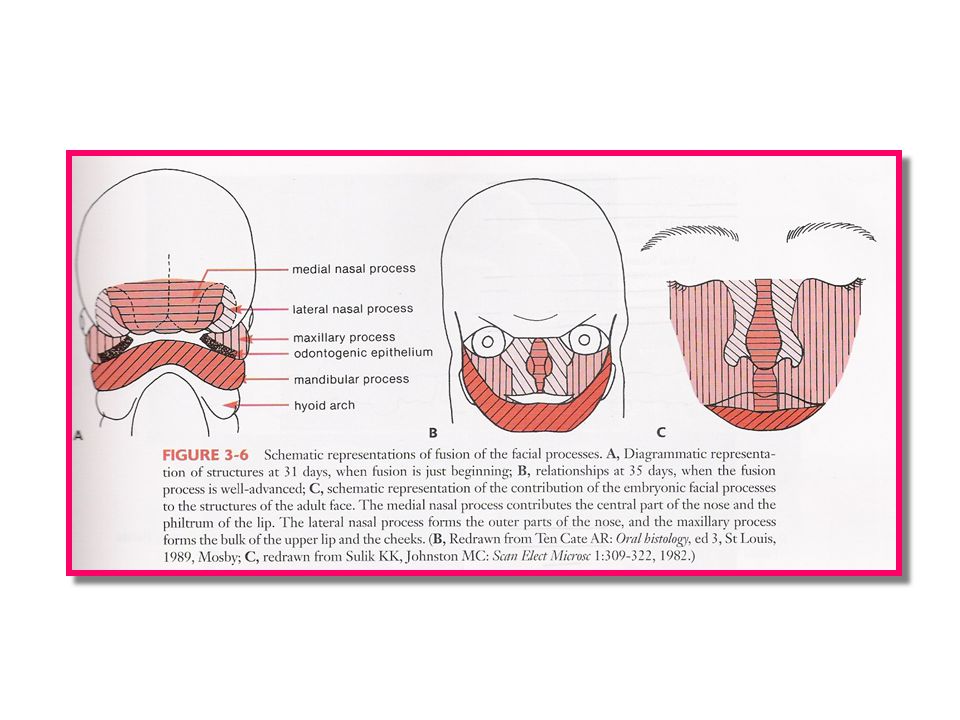
Normal Lip and Palatal Development
Fusion of lip 4– 6th week I.U. 8th to 12th week fusion of palate - Palate closure facilitated by the epithelial break down and proliferation of mesenchyme

3
Etiology of C.L./C.P. Heredity - Genetic Disorder
- Deficient Neural crest cells. - Decreased migration of Neural Crest Cells

4
Etiology of C.L./C.P. Environment:- - Teratogens - Late Pregnancies
- Folic acid deficiency

6
Cleft lip Failure of fusion between the median and lateral nasal processes and the maxillary prominance , during the 6th week of development Midline cleft of the upper lip could develop because of a split within the median nasal process. A notch in the alveolar process will accompany a cleft lip even if there is no cleft of the secondary palate.

7
Cleft palate Closure of the secondary palate by elevation of the palatal shelves follows that of the primary palate by nearly 2 weeks. About 60% of individuals with cleft lip also have a palatal cleft

9
Classification 1. Davis and Ritchie 2. Veau 3. Fogh-Anderson 4. I.P.R.S.

10
Treatment approach to a CL/CP patient
Inter disciplinary management essential Cleft lip and/or palate team consists of :- 1. Plastic surgeon 2. Maxillofacial surgeon 3. Pediatrician 4. Orthodontics 5. Speech therapist 6. Pedodontics 7. Prosthodontist 8. General Physician 9. General dentist

11
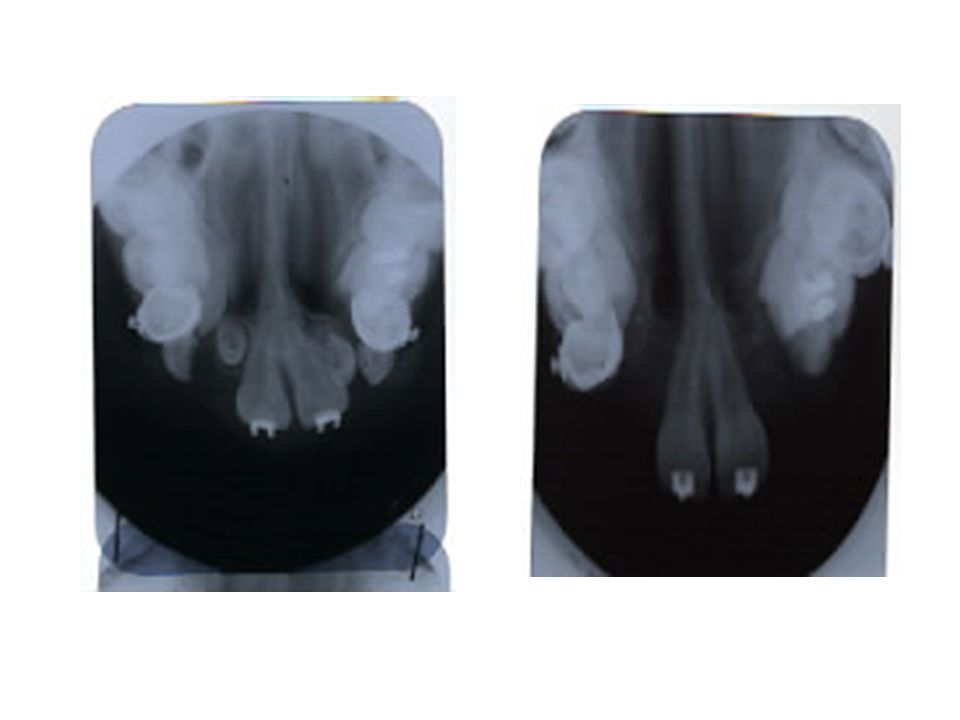
Clinical features associated to cleft patient: 1
Clinical features associated to cleft patient: 1. Natal or neonatal teeth 2. Congenitally missing teeth 3. Supernumerary teeth 4. Ectopic eruption of teeth 5. Anomalies in tooth morphology 6. Decreased periodontal support to permanent teeth erupting adjacent to cleft site 7. Mobile premaxilla. 8. Anterior and posterior crossbite. 9. Deficient maxilla.

12
Role of Orthodontics a. Infant Orthopedics b. Treatment in deciduous dentition c. Treatment in mixed dentition - Early - Late d. Treatment in permanent dentition

13
Role of presurgical orthopedics Proposed Benefits 1
Role of presurgical orthopedics Proposed Benefits 1. Control and modify the post-natal maxillary and Orofacial development 2. Stimulation of palatal shelf growth 3. Constriction of expanded anterior part of maxilla Reposition of premaxilla to aid the surgeon prior to lip repair or primary bone grafting.

14
Appliance:- Bonnet Bulb prosthesis Acrylic plates

17
Treatment in Deciduous dentition -. No treatment -
Treatment in Deciduous dentition - No treatment - Regular Check up If needed, equilibration of C’s

18
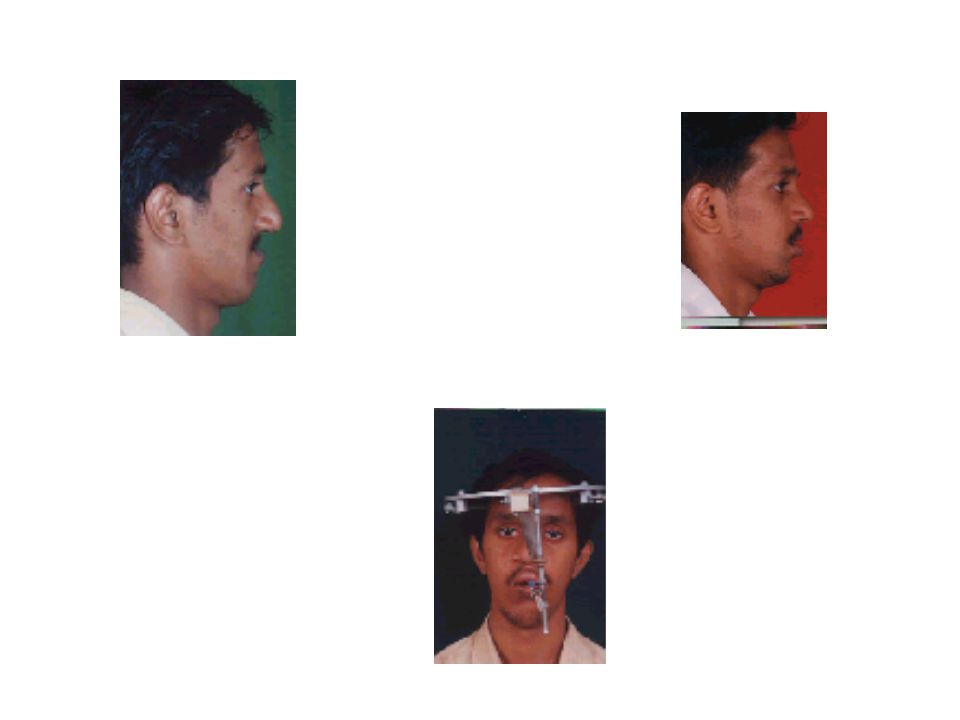
Mixed Dentition :- Maxillary protraction Maxillary protraction is done using face mask

19
Face mask therapy Indications 1. Sagittal deficiency of maxilla 2
Face mask therapy Indications 1. Sagittal deficiency of maxilla 2. Anterior cross bite 3. Low mandibular plane angle Contraindication :- - True mandibular prognathism - High mandibular plane angle. Advantage:- No Need of RME.

20
CORRECTION OF CROSSBITE
1.Rapid maxillary expansion Slow expansion screw. 3.Quad-helix

21
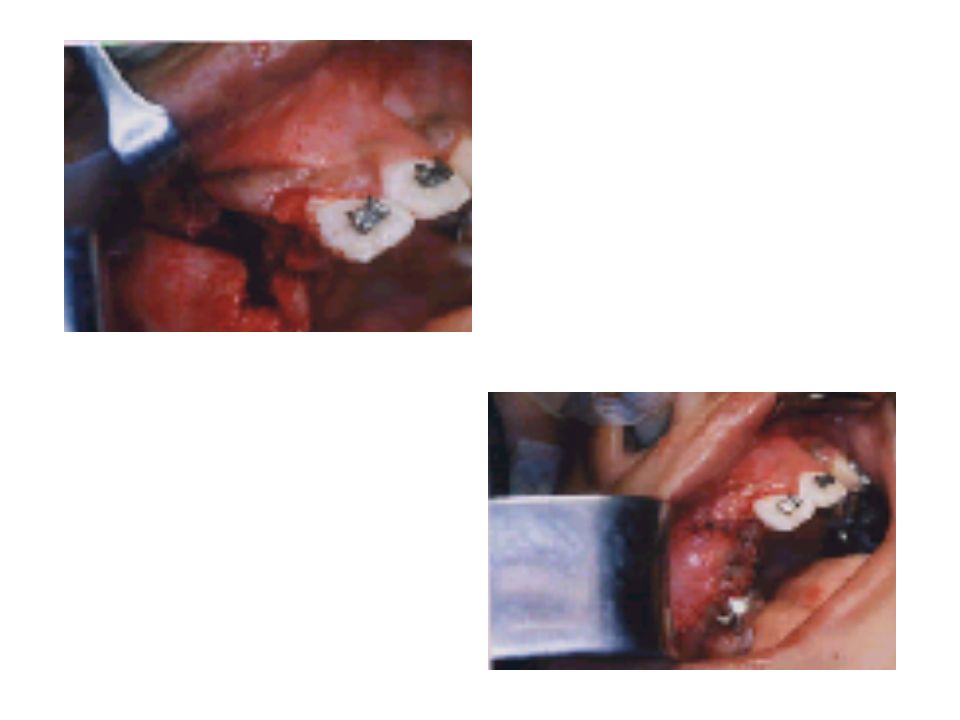
Alveolar bone grafting Types :- -. Primary bone grafting – 2yrs of age
Alveolar bone grafting Types :- - Primary bone grafting – 2yrs of age. - Secondary bone grafting – 6-15years, 1/3 of the unerupted root formed - Delayed secondary grafting.

22
Indications for Alveolar bone Graft 1. To stabilize the premaxilla 2
Indications for Alveolar bone Graft 1. To stabilize the premaxilla 2. To close the oronasal fistula 3. To ensure better periodontal support to erupting teeth and teeth adjacent to cleft site. 4. To lend support to the depressed lip over the cleft. 5. To provide bony continuity in the alveolus for tooth eruption and for orthodontic movement of teeth adjacent to cleft into their optimal position .

23
Donor Site- Cancellous bone from Iliac crest
Donor Site- Cancellous bone from Iliac crest. Orthodontic movement of teeth into or through the cleft site is not recommended unless bone grafting is done. Alveolar bone grafts have no effect on growth.

26
Treatment in permanent Dentition This is the phase of comprehensive Orthodontic treatment.

27
Treatment in permanent Dentition Main features including :- 1
Treatment in permanent Dentition Main features including :- 1. Face mask therapy prior RME Tooth movement to finalize the occlusion Management of arches 4. Correction of individual tooth irregularity 5. Closure of spaces wherever possible 6. Planned space maintenance in areas of missing teeth for prosthetic replacement. 7. Pre and postsurgical orthodontics.

29
Distraction Osteogenesis Indicated in cases of severe maxillo- mandibular discrepancy. Advantages:- Less relapse tendency.

31
Retention:- One of the nightmares for an orthodontist Greater chance of relapse in CLP patients b’coz of the Surgical scar. Usually require a long term retention. Appliances:- - Fixed lingual retainer - Upper Hawley’s retainer

32
Responsibility of Orthodontist in treatment of CLP
Responsibility of Orthodontist in treatment of CLP. THE MANAGEMENT OF THE DENTITION AND BASAL BONE RELATIONSHIP WITH PROPER SEQUENCING FOR ACHIEVING MAXIMAL FACIAL GROWTH, FUNCTIONALLY STABLE OCCLUSION AND PLEASING FACIAL ESTHETICS.

33
“There is no area of dentistry more fascinating and satisfying than rendering dental care to the unfortunate patients with cleft lip and palate”.

34
THANK YOU

Similar presentations




















 INTERCEPTIVE ORTHODONTICS McDonald, Avery, Dean. Dentistry For The Child And.>")


