Download presentation
Presentation is loading. Please wait.

1
Arch lengthening and expansion

2
Arch lengthening Increasing the arch length using distal movement of posterior teeth or proclination of incisors

3
Arch expansion Management of “narrow” arches by increasing the upper or lower intercanine, inter-premolar and/or inter-molar width

4
Arch width changes with age
Male arches wider than female Lower intercanine width increases up to change to permanent dentition Upper and lower inter-molar width increases between ages 7 to 18 Little change in premolar width after age 12

5
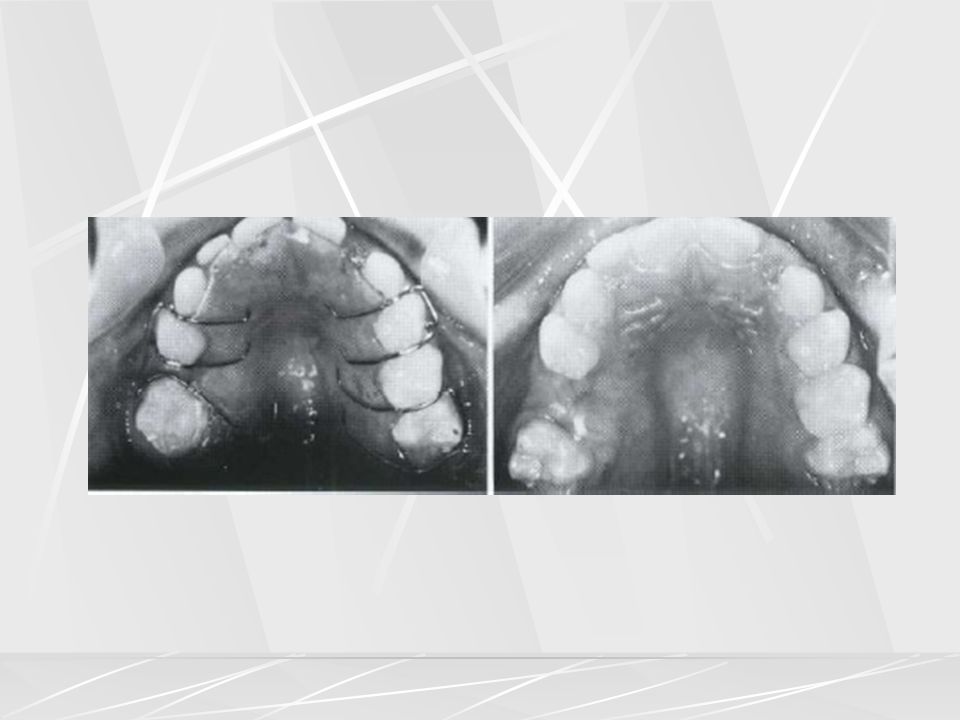
Arch expansion

6
Indications for arch expansion
Correction of posterior cross-bite Elimination of a displacement Avoiding creation of a cross-bite in cases needing distal movement of upper buccal segments “V” shaped arch in a thumb-sucker

8
Preparation for a bone graft in a cleft alveolus
Child with < 31mm of inter-molar width at age 7 yrs. Is unlikely to attain adequate arch dimensions through normal growth alone Minimal crowding in upper arch (1-2 mm) Interceptive orthodontics
 Interceptive orthodontics.")
9
Mobilization of maxillary sutural system for orthopedic correction of early CL III
Initial preparation for functional jaw orthopedics (FR III), facial mask therapy and orthognathic surgery
, facial mask therapy and orthognathic surgery.")
10
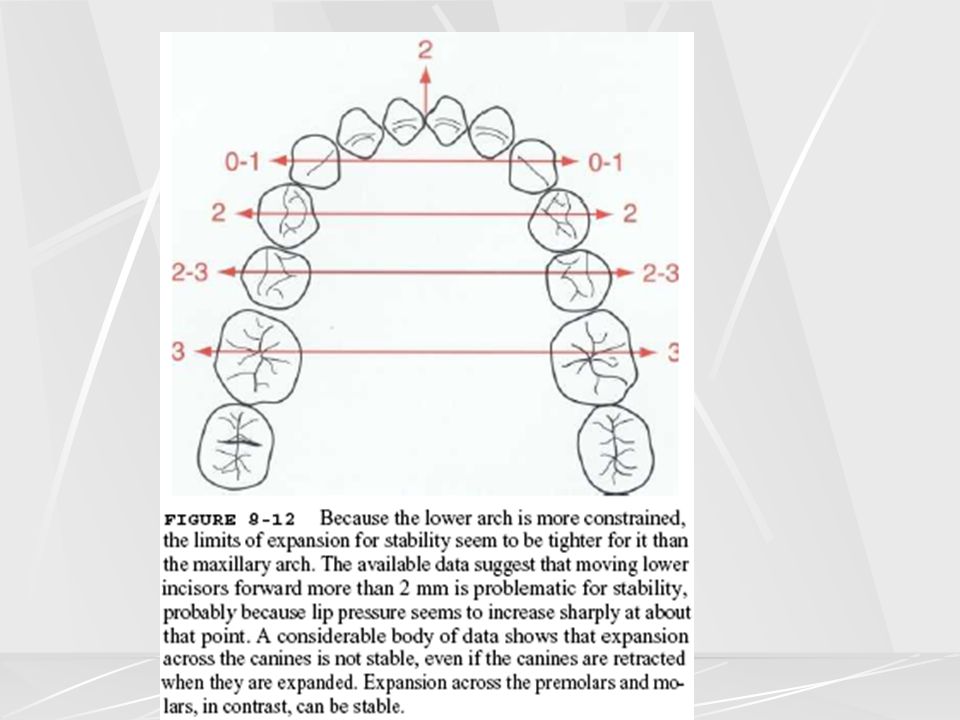
Clinical points Expansion where posterior teeth are tilted lingually may be expected to be stable Stable expansion of lower intercanine width unlikely unless canines lingually displaced Expansion more likely to be stable in absence of extractions

12
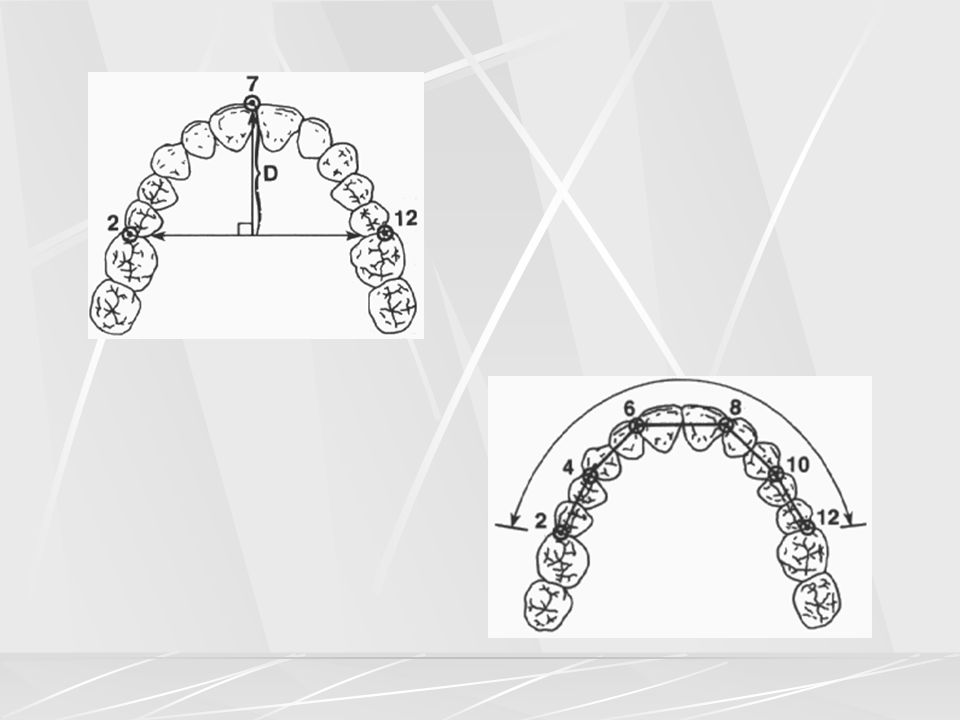
Correction of bilateral cross-bites is controversial: they may be left untreated if there is no displacement – the decision will depend on the pre-treatment inclination of the teeth and width of the underlying maxilla Over-expansion is advisable in anticipation of some relapse Increase in inter-molar width produces linear reduction in arch depth

13
1mm of arch expansion causes 0
1mm of arch expansion causes 0.3mm reduction in arch length ( equates to 0.6 mm space creation within the arch) Claims that expansion improves nasal respiration equivocal
 Claims that expansion improves nasal respiration equivocal.")
15
relapse Up to 40 % relapse has been found with all forms of active expansion Occurs via lingual tilting of molars Relapse less with fixed retainer than URA

16
complications Over expansion can cause scissors bite
Possible periodontal damage (equivocal evidence) Increase in MMP angle and lower face height thus worsening AOB
 Increase in MMP angle and lower face height thus worsening AOB.")
18
Appliances used for maxillary expansion

19
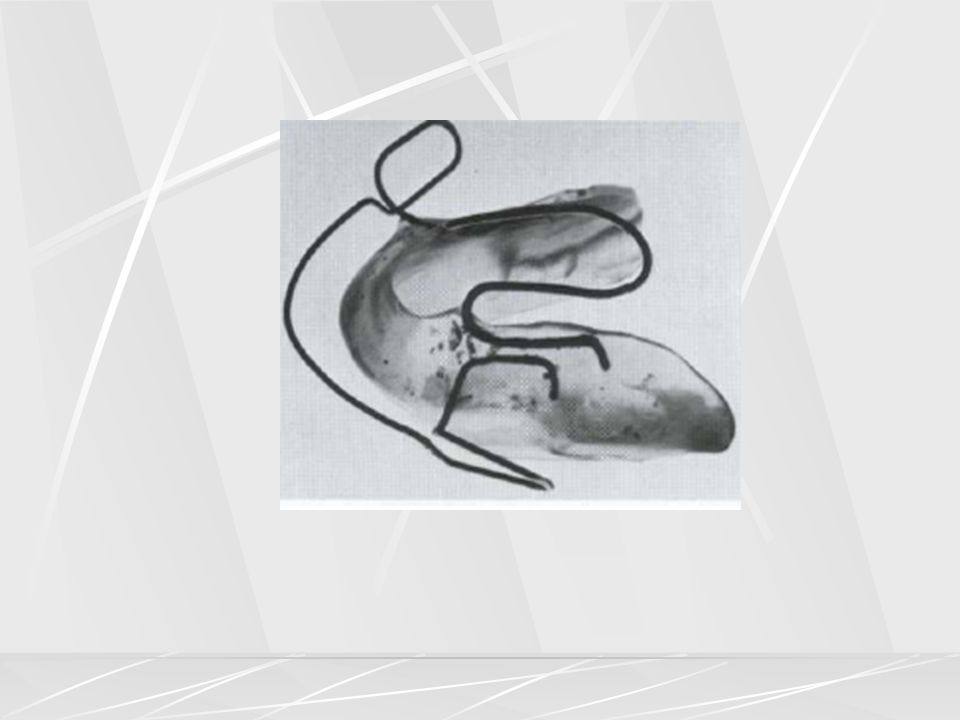
URA Design consists of an acrylic base plate which incorporates springs and retention clasps Relies on patient to turn screw two quarter turns per week Needs adequate seating and retention to produce expansion as the main effect is that of tipping Coffin springs are less well tolerated and retained but can provide differential expansion laterally and anteroposteriorly Coffin springs provide a continuous as opposed to interrupted orthodontic force

22
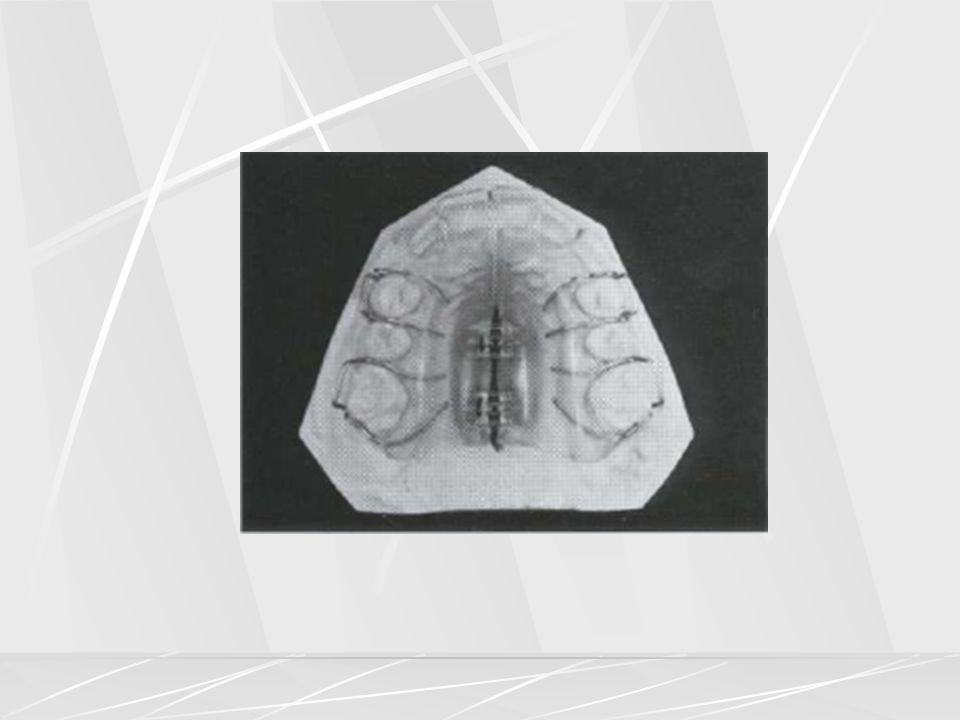
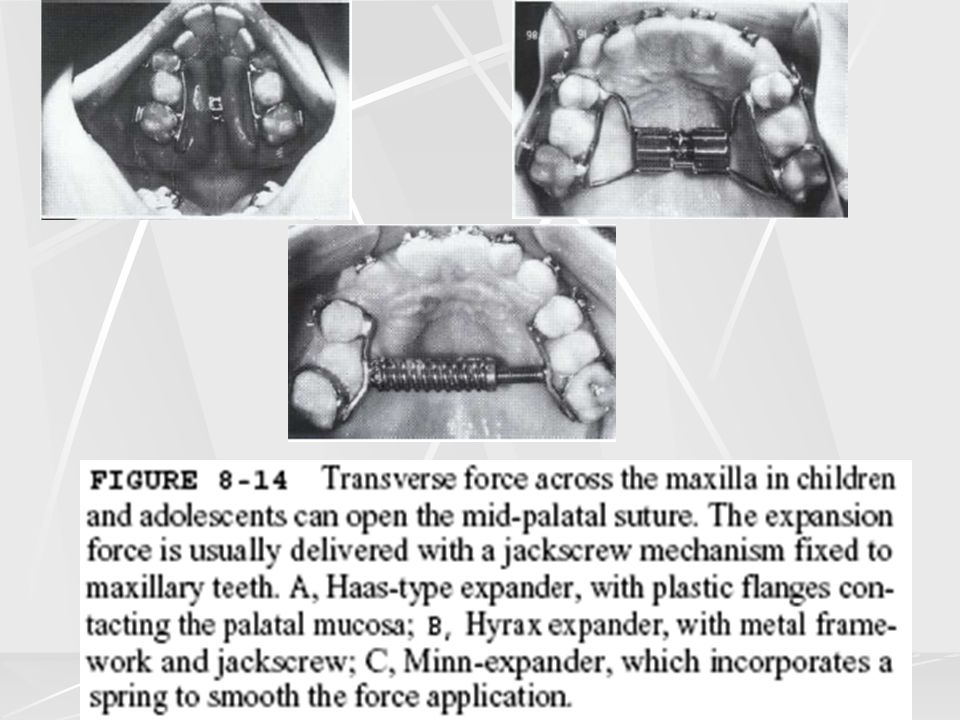
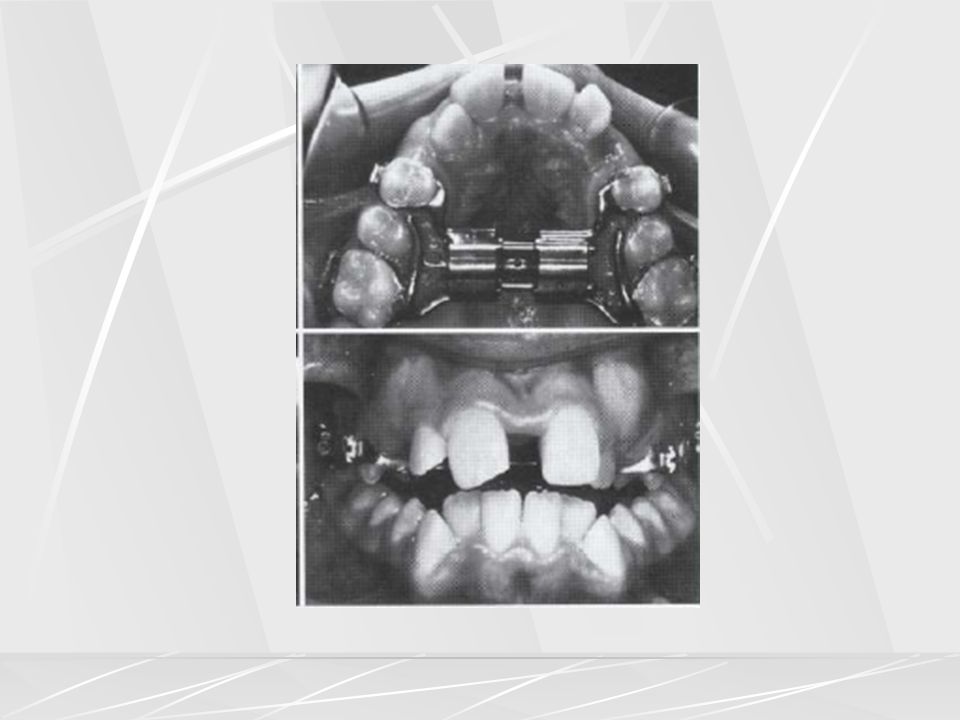
Rapid maxillary expander
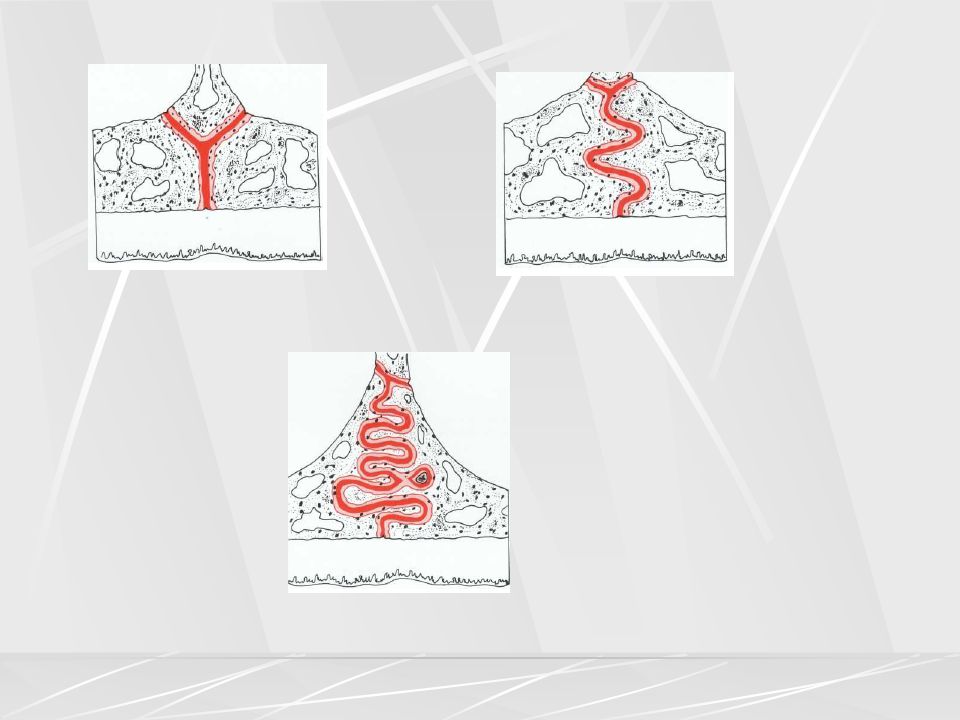
Design consists of an active plate, which incorporates a jackscrew which is attached to the teeth with wirework or acrylic Patient turns a “Hyrax” screw once a day ( mm/day) for 1-3 weeks (midline diastema develops quickly) May produce more bodily movement than other appliances There is evidence that mid palatal suture does split producing maxillary expansion
 for 1-3 weeks (midline diastema develops quickly) May produce more bodily movement than other appliances. There is evidence that mid palatal suture does split producing maxillary expansion.")
25
RME contd. Limitations are : Amount of available bone for expansion
Controversial evidence: Î periodontal breakdown compared with URA Care in choosing age for RME, due to Î resistance to maxillary base expansion which needs prolonged retention

27
RME contd. Bonded acrylic RME has occlusal coverage to reduce tipping and extrusion of molars No significant differences between bonded and banded RME

28
Surgically assisted RME
To overcome problems of expansion in non growing patients Use buccal corticotomy or Le Forte 1 osteotomy and/or midpalatal splits in conjunction with “hyrax” screw Claims: Less periodontal support loss unsubstantiated Increase in nasal air flow unsubstantiated

29
Evidence : Surgical and non-surgical techniques ; no difference in stability of expansion after one year Non-surgical expansion allows sufficient expansion in adults Problems : Surgical procedure associated with morbidity and risks Risk of nasal septum deviation

30
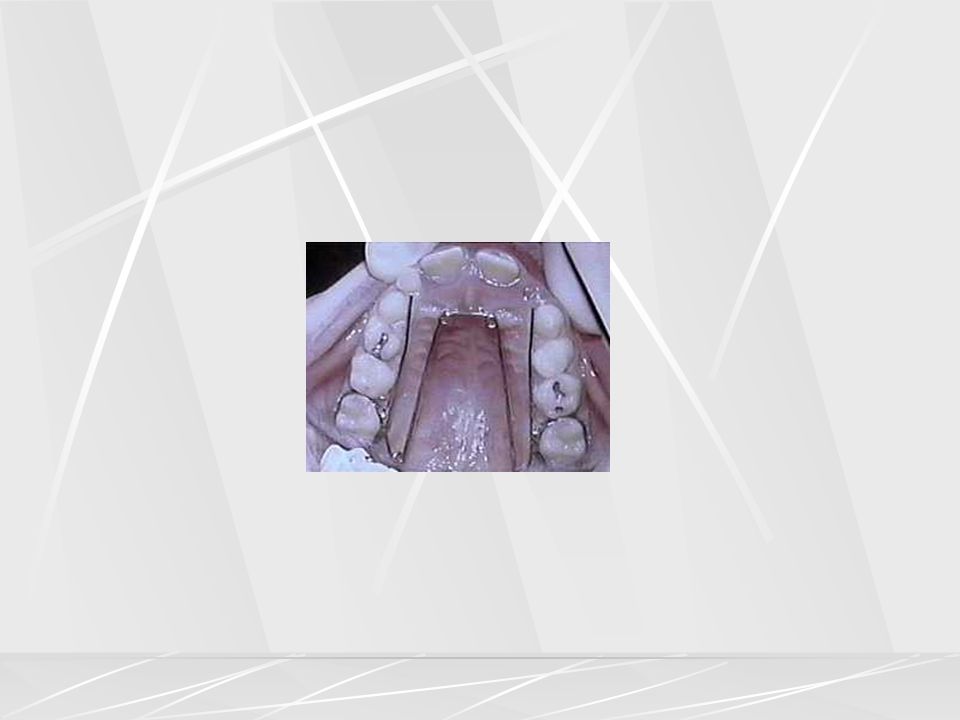
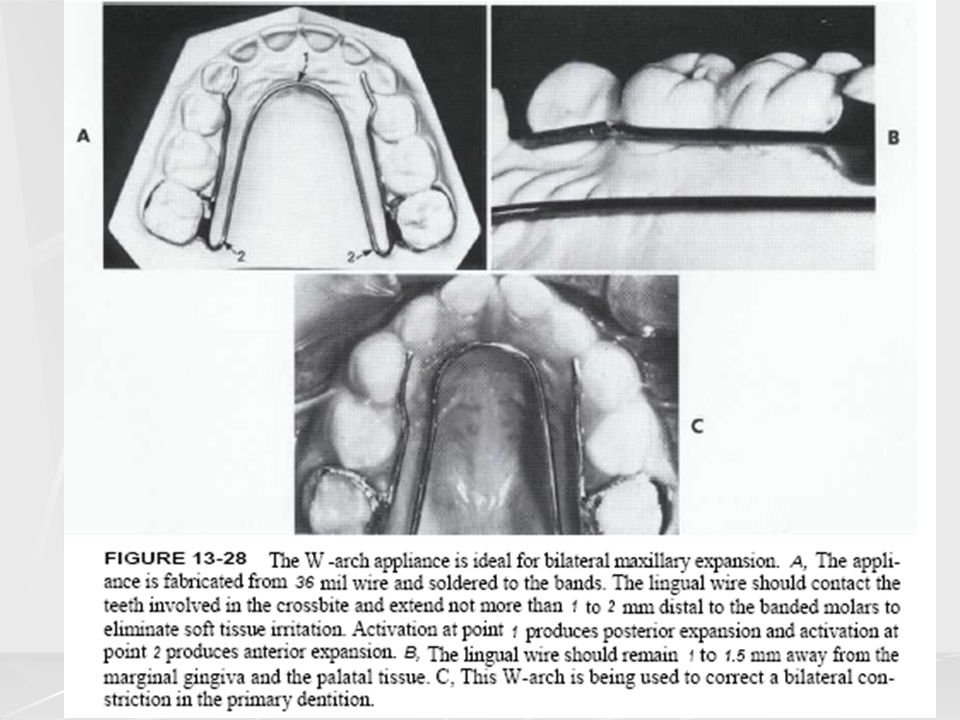
Quad /tri /bi helix Bi-helix used in mandibular arch in grossly narrowed or distorted arches, or to aid correction of a severe scissors bite Some differential expansion of inter-molar width possible (however changes in patient’s original archform may not be stable) Quad helix / tri helix fixed or removable, are useful in cleft cases Activated by half a tooth’s width on either side Provides some differential expansion and can derotate molars May produce less dental tipping than URA Unlike URA ,fixed quad helix is not reliable on patient’s compliance
 Quad helix / tri helix fixed or removable, are useful in cleft cases. Activated by half a tooth’s width on either side. Provides some differential expansion and can derotate molars. May produce less dental tipping than URA. Unlike URA ,fixed quad helix is not reliable on patient’s compliance.")
33
Fixed appliances Limited amount of expansion possible with fixed appliance alone Requires rectangular wire to prevent unfavorable dental tipping Unilateral expansion possible but requires placement of buccal root torque on correct side to prevent tipping

34
Functional appliances
Produce active expansion ( usually with either expansion screw or palatal arch) to prevent cross bite formation whilst a CL I relation is being obtained Frankel appliance produces passive expansion only by removing influence of buccal tissues with buccal shields
 to prevent cross bite formation whilst a CL I relation is being obtained. Frankel appliance produces passive expansion only by removing influence of buccal tissues with buccal shields.")
39
Arch lengthening

40
indications Non extraction cases with only very mild crowding (1-2 mm)
Any change in original arch form is likely to collapse, so lengthening must be kept to a minimum Half unit CL II molar relationship in a non-extraction case Correction of incisal relationship in CL III case by proclination if upper incisors Regain space lost by early loss of deciduous teeth Correction of retroclined mandibular incisors in CL II/2 cases,or CL II/1 cases with mandibular incisors trapped in palate

41
Arch lengthening procedures
Distalisation of upper buccal segments Distalisation of lower buccal segments Proclination of upper or lower incisors

42
Distalisation of upper buccal segments
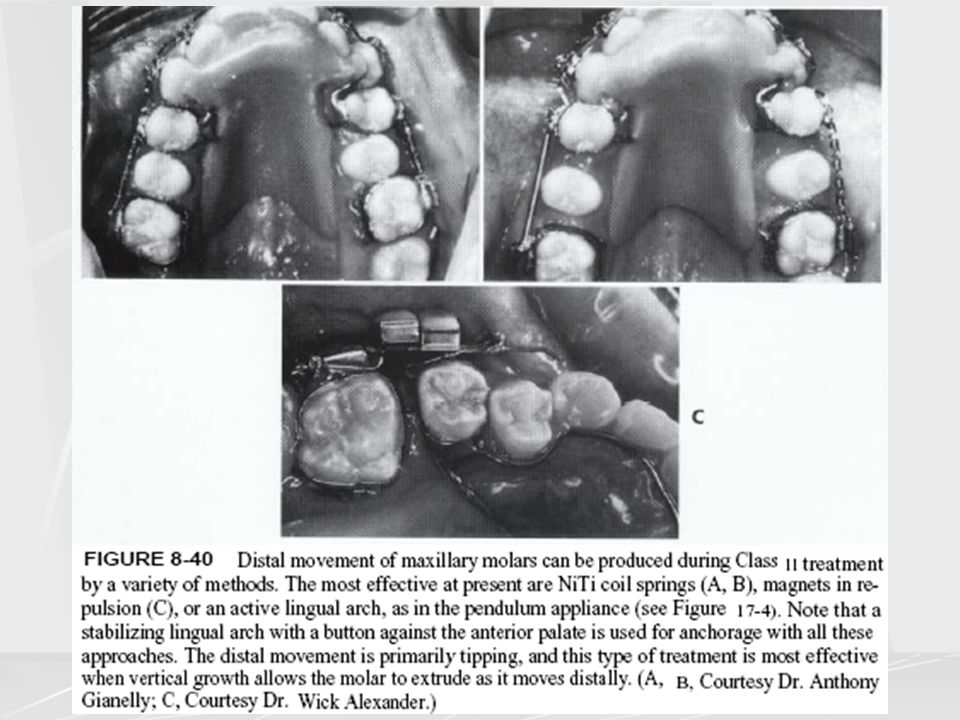
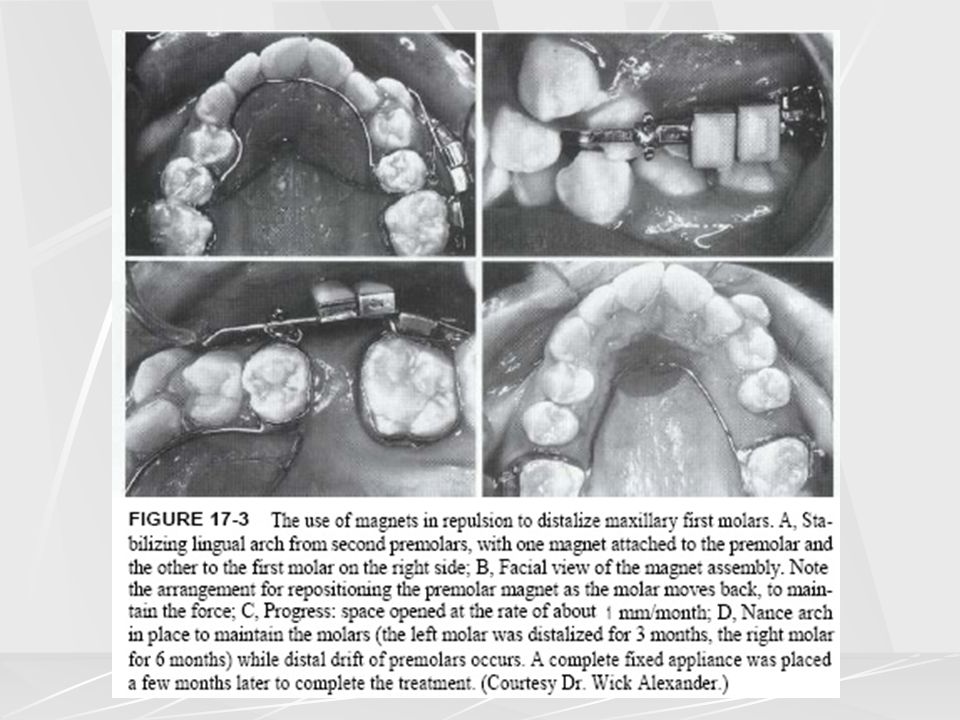
HG with URA ( palatal finger springs to upper 6s, bite plane, HG to 6s tubes) HG with no URA – HG to 6s tubes only. May take longer as there is no finger springs to prevent to prevent relapse during the day when HG is not worn Distalising super elastic Nickel titanium coil springs Magnets supported with CL II traction Active palatal arch (TPA)
 HG with no URA – HG to 6s tubes only. May take longer as there is no finger springs to prevent to prevent relapse during the day when HG is not worn. Distalising super elastic Nickel titanium coil springs. Magnets supported with CL II traction. Active palatal arch (TPA)")
47
Distalisation of lower buccal segments
Lip bumper ; not well tolerated Removable appliance and HG

49
Proclination of upper or lower incisors
URA ( split screw anteriorly, “Z” springs or “T” springs) ELSA (expansion and labial segment alignment appliance); recurved spring or “wiper” arms to procline incisors Labial crown torque ( rectangular wire in FA ) Avoiding the use of “lace backs” in CL III maxillary incisors Side effect of some FA is to procline the mandibular incisors if there is no incisal capping
 ELSA (expansion and labial segment alignment appliance); recurved spring or wiper arms to procline incisors. Labial crown torque ( rectangular wire in FA ) Avoiding the use of lace backs in CL III maxillary incisors. Side effect of some FA is to procline the mandibular incisors if there is no incisal capping.")
Similar presentations














>")











