Download presentation
Presentation is loading. Please wait.

1
Caries Management by Risk Assessment in Children
Niki Fallah D.D.S 3/26/13

2
Research Committee: Ling Zhan D. D. S. , Ph. D John D. B
Research Committee: Ling Zhan D.D.S., Ph.D John D. B. Featherstone M.Sc., Ph.D. Pamela Den Besten D.D.S., M.S. Jing Cheng, MD, MS, PhD

3
Background: Dental caries is the single most common chronic infectious disease amongst children in United States. Main bacteria: mutans streptococci (MS) Studies have demonstrated the progression of caries from the primary dentition to the permanent dentition as a major problem, with 6-9 year old age groups being at the highest risk. More than 51 million school hours are lost each year to dental-related illness. The annual cost of dental caries treatment in children accounts for as least $4.5 billion in the US
 Studies have demonstrated the progression of caries from the primary dentition to the permanent dentition as a major problem, with 6-9 year old age groups being at the highest risk. More than 51 million school hours are lost each year to dental-related illness. The annual cost of dental caries treatment in children accounts for as least $4.5 billion in the US.")
4
Caries Risk: Caries Balance
Caries progression occurs when the risk factors for caries outweigh the protective factors. The goal of caries management by risk assessment (CAMBRA) is to tip the balance to prevent new carious lesions from forming Protective factors include the reduction of cariogenic bacteria by antibacterial treatment, enhanced remineralization by fluoride, and increased salivary function. Identification of risk factors that imbalance the caries equilibrium and protective factors that restore the caries balance is the key for caries prevention
 is to tip the balance to prevent new carious lesions from forming. Protective factors include the reduction of cariogenic bacteria by antibacterial treatment, enhanced remineralization by fluoride, and increased salivary function. Identification of risk factors that imbalance the caries equilibrium and protective factors that restore the caries balance is the key for caries prevention.")
5
CAMBRA New strategies of Caries Management by Risk Assessment (CAMBRA) were implemented 8 years ago for adults in the pre-doctoral dental clinics at the University of California San Francisco (UCSF). These CAMBRA guidelines for adults are currently also recommended for children over 6 years. However, no study has been conducted to validate the efficacy of CAMBRA in children.
 were implemented 8 years ago for adults in the pre-doctoral dental clinics at the University of California San Francisco (UCSF). These CAMBRA guidelines for adults are currently also recommended for children over 6 years. However, no study has been conducted to validate the efficacy of CAMBRA in children.")
6
CAMBRA Protocol – Adult
Risk Level Antimicrobials Home Fluoride Professional CRA and F- Xylitol and/or Baking soda Low Not Indicated Regular OTC Fluoride containing toothpaste twice daily CRA every 12 months Moderate Rx 5000ppm fluoride toothpaste twice daily CRA every 6 months Fluoride varnish every 6 months Xylitol gum or mints. 8g daily High Chlorhexidine 0.12%rinse for 1 min daily for 1 week each month Extreme Trays for home application 5000ppm F- gel q d x 5min CRA every 3-6 monthsFluoride varnish every 3-6 months Xylitol gum or mints. 8g daily. Baking soda rinse 4-6 x daily Issues with this CAMBRA model for children: The control of MS infections through the use of chlorhexidine mouthrinses is frequently not possible in children because of taste and compliance issues. In general high concentration fluoride toothpaste is also not recommended for children due to the risk of fluorosis that results from accidental ingestion of high doses of fluoride during tooth development. However, diet may be more readily controlled in 6-9 year-old children.

7
Modified CAMBRA for children:
Eliminate chlorhexidine mouth-rinse and high concentration home use fluoride regimens for children aged 5-9 years. Adopt a regimen including more frequent professional fluoride application, xylitol products, and baking soda rinse for high and extreme risk patients. The regimen will focus on building good diet and oral hygiene habits and controlled office fluoride varnish delivery. Xylitol mints will be incorporated to modify the caries-causing oral microbial flora.

8
Xylitol: sugar sweetener, in the sugar alcohol or polyol family
commonly used as a sugar substitute, maintaining the same level of sweetness as table sugar with half the amount of calories. In the same category as other universally known sweeteners such as sorbitol, mannitol, and maltitol. xylitol has been well accepted to be non-cariogenic along with its cariostatic effect in chewing gum

9
Mechanism of Xylitol: Cannot be metabolized by MS.
It competes with sucrose in the intra-cellular metabolism process, reducing the energy source for MS. Short-term consumption of xylitol is associated with decreased S mutans levels in both saliva and plaque. Long-term habitual consumption of xylitol appears to have selective effects on S mutans strains This results in populations that are less virulent and less capable of adhering to tooth surfaces and, thus, are shed more easily from plaque into saliva

10
Aim: The aim of the study is to evaluate the efficacy of a modified Caries Management by Risk Assessment (CAMBRA) model in a clinical trial in children aged 6-9 years treated in a school-based community pediatric dental clinic setting. Specifically: Reducing MS & LB levels Improving the oral hygiene and dietary habits.
 model in a clinical trial in children aged 6-9 years treated in a school-based community pediatric dental clinic setting. Specifically: Reducing MS & LB levels. Improving the oral hygiene and dietary habits.")
11
Hypothesis: In 5-9 year old children, a modified CAMBRA protocol will significantly reduce the cariogenic bacterial load, improve oral hygiene care and dietary habits as compared to the conventional prevention regimen.

12
Study Design

13
Site selection and recruitment:
The UCSF school-based Pediatric Dental Clinic in the Tenderloin Community is located in Tenderloin Elementary School sponsored by a non-profit organization, Bay-Area Women. The clinic is operated one day a week by UCSF Pediatric Dentistry faculties, pediatric dental residents and staff. Over 200 children aged 5-9 years are currently enrolled in the school The clinic sees large numbers of low-income patients likely to be at high risk for caries.

14
Inclusion Criteria: Exclusion Criteria: 1) 5-9 years old
Participants will be patients of record at the UCSF Pediatric Dental Clinic in the Tenderloin Community and must be: 1) 5-9 years old 2) able to give informed assent, consent and answer questionnaires in English, Spanish, Chinese or Vietnamese by parents or guardian 3) unlikely to move from the school during the study period 4) willing to participate regardless of group assignment and comply with all study procedures. Exclusion Criteria: Persons with: 1) Long-term antibiotic use in the past month 2) Dental needs outside the realm of the community pediatric clinics, such as care provided in specialty clinics
 5-9 years old. 2) able to give informed assent, consent and answer questionnaires in English, Spanish, Chinese or Vietnamese by parents or guardian. 3) unlikely to move from the school during the study period. 4) willing to participate regardless of group assignment and comply with all study procedures. Exclusion Criteria: Persons with: 1) Long-term antibiotic use in the past month. 2) Dental needs outside the realm of the community pediatric clinics, such as care provided in specialty clinics.")
15
Materials/Method Modified CAMBRA regimen:
Building good diet and oral hygiene More frequent professional visits and office fluoride varnish Use of a daily xylitol mints

16
Sample size: n= 130 Randomization: Computer generated randomization sheets were used for subject assignment into intervention or control groups. Treatment team assignments were kept in consecutively numbered, sealed, opaque envelopes. Saliva analysis: MS and LB levels in saliva were measured by selective culture according to routine procedures. *All participants received a $10 Target gift card at each saliva collection, totaling $30 by the end of their participation in the study.

17
Caries Status Assessment:
Dr. Ling Zhan assessed caries status at the initial exam and at the final visit in a standard dental operatory in the clinic. Traditional DMFS/dmfs scores were obtained on all teeth. Non-cavitated lesions were recorded if any were noted. Supplementary radiographic evidence was used for proximal surfaces as part of patient care at the beginning and end of the study for all subjects. Caries risk categories were identified by using the CRA form that is being used at UCSF Pediatric Dentistry Clinic.

19
Statistical Analysis:
All data was entered into a computerized database. Demographics, compliance, and questionnaire items for the two groups were compared using Fisher exact tests, chi-square tests, t-tests, and Wilcoxon rank sum tests, depending on the scale of the item. Salivary components (MS, LB, and F) for the two groups were assessed with rank analysis of covariance (RANCOVA) adjusting for baseline values.
 for the two groups were assessed with rank analysis of covariance (RANCOVA) adjusting for baseline values.")
20
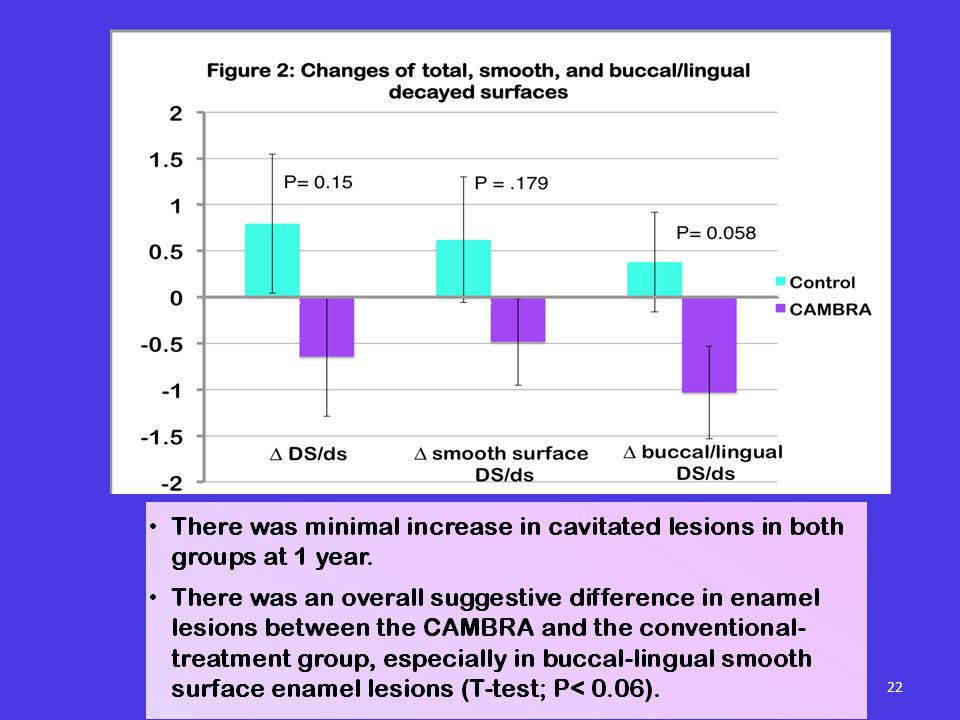
Results:

23
Conclusion:

24
Limitations of study: Actual number of subjects: 66
Patient compliance with xylitol Student transfer rate out of school School schedule (daily schedules, summer/winter vacation) Communication with parents
 Communication with parents.")
25
THANK YOU!

Similar presentations






 Initiative>")














