Download presentation
Presentation is loading. Please wait.

1
Therapeutic Drug Monitoring Relates concentrations of drug in blood to response Blood concentrations surrogate for the concentration at the site of action When concentration correlates better than the dose with the drug effect – the dose cannot be titrated against response eg INR, cholesterol (pharmacodynamic markers) – the drug is being used to prevent infrequent occurrences - eg epilepsy – toxicity or failure of therapy (compliance ??)
 – the drug is being used to prevent infrequent occurrences - eg epilepsy – toxicity or failure of therapy (compliance )")
2
Conditions that must be met Measurement of concentrations available Blood concentrations can be accurately reliably and economically measured sufficient inter-individual variation of PK exists warrant individualisation of dose There is a clear relationship between concentration and beneficial and/or adverse effects, particularly if there is a narrow therapeutic index Therapeutic window known

3
Purpose of TDM To confirm/establish ‘effective’ concentrations – Maximizing efficacy To avoid or anticipate toxic concentrations – Consider also function of excretory organs and drug interactions To investigate unexpected lack of efficacy – To check compliance – Before increasing to unusually large doses Limited role in toxicology - drug screen

4
Pharmacokinetic Considerations Is the aim to provide constant concentrations? eg anticonvulsants Especially if drug concentrations likely to vary greatly between individuals on the same dose phenytoin Remember it takes around 5 half-lives to reach steady state Is the aim to achieve transient high concentrations without toxicity? eg gentamicin

5
Practical considerations Can the lab actually measure the drug? What sample is needed? What is the right timing? Is there an accepted ‘therapeutic range’ MEC threshold concentration above which efficacy is expected in most patients with the disorder MTC upper concentration above which the rate and severity of adverse effects become unacceptable – Cmax, Cmin, AUC

6
Problém – intra- a interindividální variabilita

7
Factors affecting interpretation of TDM Disease state: renal, liver… Habits: diet, smoking, drinking Physiology – pregnancy, age, weight Non-compliance Electrolyte balance: Digoxin vs K+ and Ca2+ Drug interaction, autoinduction Protein binding Bioavailability Sampling time

8
Methodological Difficulties in establishing ‘Therapeutic Range’ Good PK/PD data are seldom available – Ideally trials where participants were randomised to different plasma concentrations – with follow-up and – accurate and unbiased measurement of the outcomes

9
Drugs with TDM-guided dosing Antibioticsaminoglycosides: gentamicin, amikacin, tobramycine, netilmicine glycopeptide ATB: vancomycin B-lactam: PenC…….. Antifungal drugsflucytosine, itraconazole Protease inhbitors (HIV) saquinavir, indinavir, nelfinavir, ritonavir Immunosupressanscyclosorine, tacrolimus, sirolimus, mycophenolate, methotrexate, mercaptopurine/azathioprine
 saquinavir, indinavir, nelfinavir, ritonavir Immunosupressanscyclosorine, tacrolimus, sirolimus, mycophenolate, methotrexate, mercaptopurine/azathioprine.")
10
Drugs with TDM-guided dosing Antiepileptic drugsphenytoin, carbamazepine, valproate Antipsychoticsclozapine, lithium Cytostaticsmethotrexate, 5-fluorouracil, Otherdigoxin, theophylline

11
Anticonvulsants PD cannot be measured – PK maintenance Variable dose dependent kinetics + enzymatic changes 0 order kinetics of phenytoin small dose increases can produce disproportionate rises in blood levels and toxicity Most metabolised through cytochrome P450 system Concentration-related CNS toxicity can be partly avoided by TDM – severe skin rashes, liver and marrow toxicity cannot be predicted or avoided Sometimes free (unbound) concentrations need eg hypoalbuminaemia, pregnancy
 concentrations need eg hypoalbuminaemia, pregnancy")
12
Nelineární (saturabilní) kinetika fenytoinu u 5 epileptiků léčených různými dávkami.
 kinetika fenytoinu u 5 epileptiků léčených různými dávkami.")
13
Pokles vazebných míst při hypoalbuminémii zvyšuje volnou koncentraci léčiv s vysokou vazbou - fenytoin

14
Orders

15
Digoxin variable bioavailability + variable clearance (by kidney) P-gp the elderly Drug interactions are fairly common Relationship between concentration and effect is not constant concentrations soon after dosing are difficult to interpret. Range is approx 1 to 2 nmol/L Concentrations should be measure at least 6-8 hours after the last dose ‘sensitizing’ factors eg hypokalalaemia, hypothyroidism In atrial fibrillation titrate against the ventricular rate

16
Cyclosporin immunosuppressant in transplants Low therapeutic index – toxicity (kidney) is severe Interactions are common – eg calcium channel antagonists Plasma range 50-300 mg/L
 is severe Interactions are common – eg calcium channel antagonists Plasma range mg/L")
17
Theophylline Declining use in asthma Very narrow therapeutic index: – 55 - 110 umol/L (should be lower) At the high end toxicity is common – Toxicity is severe – GI, neuro, cardiac Interactions are common – erythromycin, cyclosporin, cimetidine, smoking
 At the high end toxicity is common – Toxicity is severe – GI, neuro, cardiac Interactions are common – erythromycin, cyclosporin, cimetidine, smoking")
18
PK/PD guided therapy of antibiotics f T>MICC max /MICAUC 0–24 /MIC b-Lactams Carbapenems Linezolid Erythromycin Clarithromycin Lincosamides Aminoglycosides Metronidazole Fluoroquinolones Telithromycin Daptomycin Fluoroquinolones Aminoglycosides Azithromycin Tetracyclines Glycopeptides Tigecycline Linezolid f T>MIC, time dependent antimicrobials; C max /MIC, concentration-dependent antimicrobials; AUC 0–24 /MIC, concentration-dependent antimicrobials with time dependence.

19
c Conc. Time MIC t (C > MIC) C max AUC C>MIC C min
 C max AUC C>MIC C min")
20
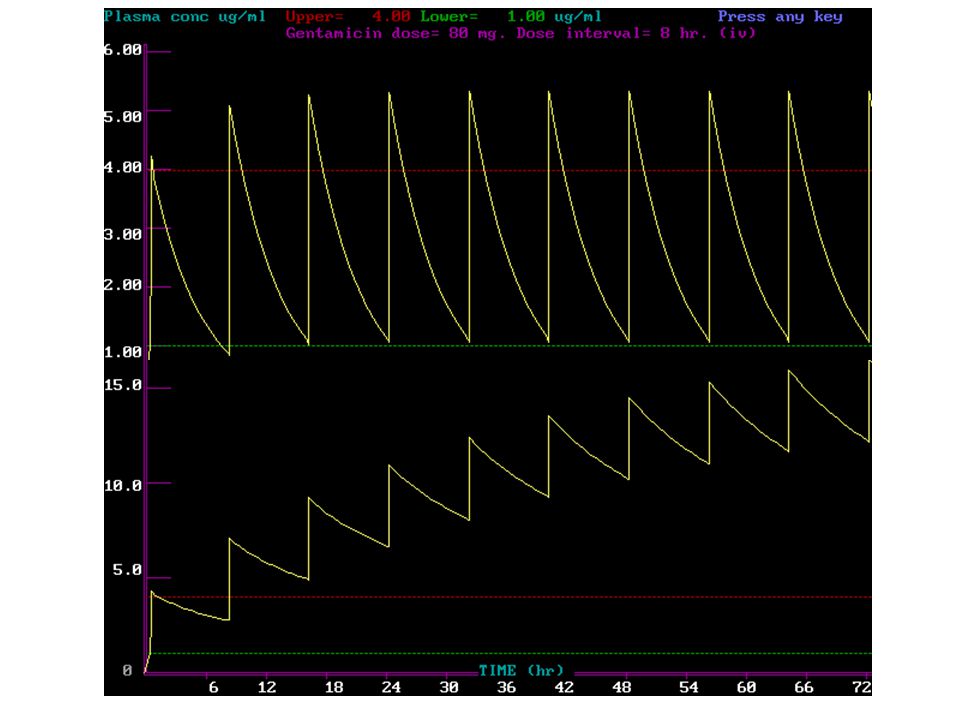
Gentamicin trend to once/daily dosing Toxicity relates to trough concentrations, – particularly with prolonged therapy Desirable range: – peak 6 - 10 mg/L – trough 1-2 mg/L

22
Plazmatické koncentrace gentamicinu u 6 nedonošených novorozenců s nízkou porodní hmotností 4. den postnatálního života. Ali, et al.: Pharmacokinetics of gentamicin

23
Plots of observed versus predicted gentamicin concentrations for the basic and final population models tested. Lanao J M et al. J. Antimicrob. Chemother. 2004;54:193-198 Ali, et al.: Pharmacokinetics of gentamicin

24
Simulated serum gentamicin concentrations and 68% confidence intervals using the final population model in a term newborn and in a premature infant following the administration of an iv dose of gentamicin of 10 mg/kg (0.5 h iv) to achieve target peak and trough serum levels of 15–20 mg/L and <0.5 mg/L, respectively. Lanao J M et al. J. Antimicrob. Chemother. 2004;54:193-198 Ali, et al.: Pharmacokinetics of gentamicin

25
Most evidence suggests that ototoxicity is less for once/day dosing than more frequent dosing

26
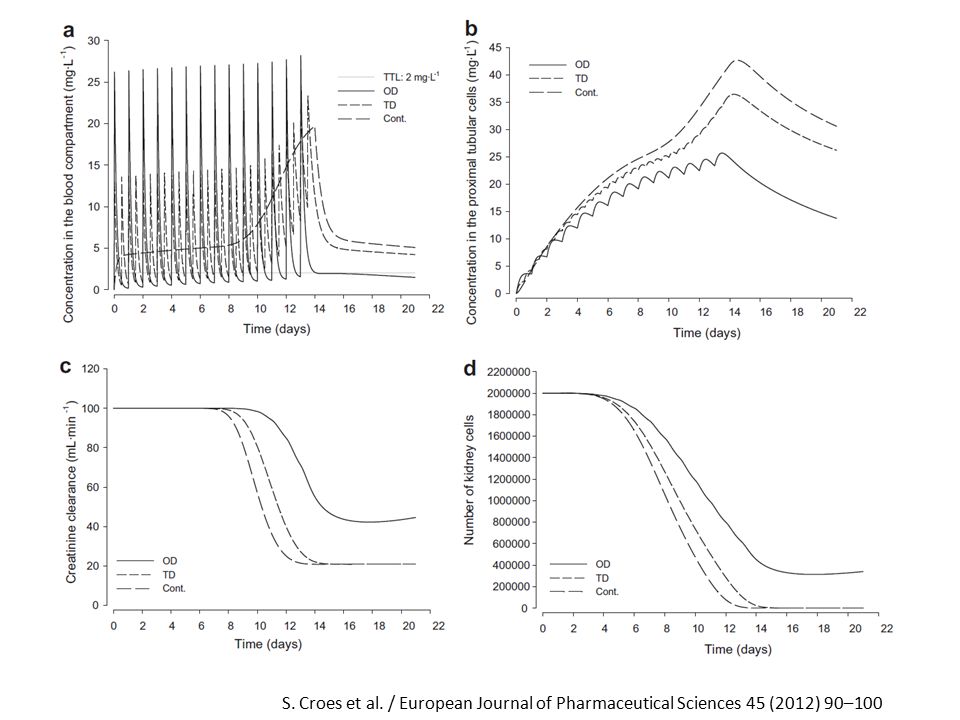
(a) Blood concentrations of aminoglycosides - 7 mg kg1 day1 OD (solid line), TD (dotted line) and continuous simulated infusions (dash-dotted line) versus the time in days. Also shown is the target trough level (TTL), (2 mg L1). (b) The corresponding reductions in number of viable bacteria versus the predicted time of eradication in days. The horizontal dashed-dotted line represents the target value for efficacy. Gentamicin S. Croes et al. / European Journal of Pharmaceutical Sciences 45 (2012) 90–100
, (2 mg L1). (b) The corresponding reductions in number of viable bacteria versus the predicted time of eradication in days. The horizontal dashed-dotted line represents the target value for efficacy. Gentamicin S. Croes et al. / European Journal of Pharmaceutical Sciences 45 (2012) 90–100.")
28
Vancomycin TDM Troughs should be obtained just prior to the next dose at steady-state conditions – (approximately after the fourth dose). Minimum serum vancomycin trough concentrations should always be maintained above 10 mg/L – to avoid development of resistance. – or a pathogen with an MIC of 1 mg/L, the minimum trough concentration would have to be at least 15 mg/L to generate the target AUC (Area under the curve):MIC of 400. Continuous infusion regimens not suitable – Do not improve patient outcomes when compared to intermittent infusions.
:MIC of 400. Continuous infusion regimens not suitable – Do not improve patient outcomes when compared to intermittent infusions..")
29
Vancomycin TDM - AE Nephrotoxicity – Data do not support using peak serum concentrations to monitor – Trough monitoring is recommended for patients receiving aggressive dosing – (i.e. to achieve sustained trough levels of 15–20 mg/L) and all patients at high risk of nephrotoxicity – (e.g. patients receiving concurrent nephrotoxins). for patients with unstable renal function – (i.e. deteriorating or significantly improving) and those receiving prolonged courses of therapy – (more than three to five days). Ototoxicity – TDM is not recommended for patients receiving vancomycin monotherapy. – should be considered for patients receiving additional ototoxics such as aminoglycosides. Martin JH et al. Clin Biochem Rev Vol 31 February 2010
 and all patients at high risk of nephrotoxicity – (e.g. patients receiving concurrent nephrotoxins). for patients with unstable renal function – (i.e. deteriorating or significantly improving) and those receiving prolonged courses of therapy – (more than three to five days). Ototoxicity – TDM is not recommended for patients receiving vancomycin monotherapy. – should be considered for patients receiving additional ototoxics such as aminoglycosides. Martin JH et al. Clin Biochem Rev Vol 31 February")
30
0 1 2 3 4 5 6 7 8 9 10 0 30 60 90 120 150 180 0 20 40 60 80 100 0 20 40 60 80 100 PASI Score (% of initial value) AUC ( mol · h · l -1 ) RBC MTX (nmol · l -1 ) r s = -0.912 P > 0.002 r s = -0.988 P > 0.002 MTX in psoriasis
 AUC ( mol · h · l -1 ) RBC MTX (nmol · l -1 ) r s = P > r s = P > MTX in psoriasis")
31
Průběh plazmatických koncentrací MTX po podávání celkové týdenní dávky 15 mg jednorázově a rozděleně do třech dílčích po 12 hod.

32
Predikce dávkování LDMTX.

33
Lithium for bipolar disorder Toxic neurological, cardiac, renal Narrow therapeutic range: 0.8 - 1.2 mmol/L acutely 0.5 - 0.75 mmol/L for maintenance Chronic concentrations of 3.0 are potentially lethal Renal clearance of Li can be affected by diuretics and NSAIDs

34
REQUEST FORM OF TDM Patient Name............................................. Date............................................... HN........................................................ Age.................................. Sex................................. Wt...................................... Ht......................................................... Ward.............................................Ordered by....................................................... Phone No.......................................... DRUG LEVEL REQUESTED.................................................................................................................................................. REASON FOR REQUEST : ( ) Suspected toxicity ( ) Compliance ( ) Therapeutic confirmation ( ) Absence of therapeutic response Please indicate when level is needed : ( ) within 24 h ( ) within 1-2 h ( ) stat ( ) others........................ TIME AND DATE OF LAST DOSE : Date.................... Route : IV, IM, SC, PO, Others........................... Time.................... Dose.......................... Freq.................................. THIS DRUG LEVEL IS FOR : SAMPLING TIME : ( ) Trough or predose level Date....................... Time......................... ( ) Peak level Date....................... Time........................ DOES THE PATIENT HAVE ORGAN-SYSTEM DAMAGE ? ( ) Renal ( ) Hepatic ( ) Cardiac ( ) GI ( ) Endocrine ( ) Others........................…. OTHER DRUG(S) PATIENT IS TAKING :.........................................................................................................…….. DRUG LEVEL & USUAL THERAPEUTIC RANGE............................................................................................……. INTERPRETATION...............................................................................................................................................…................................................................................................................................................................................……. Date.......................... Technologist................................. Time............................…………..
 Suspected toxicity ( ) Compliance ( ) Therapeutic confirmation ( ) Absence of therapeutic response Please indicate when level is needed : ( ) within 24 h ( ) within 1-2 h ( ) stat ( ) others TIME AND DATE OF LAST DOSE : Date Route : IV, IM, SC, PO, Others Time Dose Freq THIS DRUG LEVEL IS FOR : SAMPLING TIME : ( ) Trough or predose level Date Time ( ) Peak level Date Time DOES THE PATIENT HAVE ORGAN-SYSTEM DAMAGE . ( ) Renal ( ) Hepatic ( ) Cardiac ( ) GI ( ) Endocrine ( ) Others …. OTHER DRUG(S) PATIENT IS TAKING : …….. DRUG LEVEL & USUAL THERAPEUTIC RANGE ……. INTERPRETATION … ……. Date Technologist Time …………...")
35
Drug Time to steady state Sampling time Therapeutic range (mg/L) Aminoglycosides Amikacin Adults ( 30 y): ~ 7.5-75 h(1 h after IM) Gentamicin Children: ~ 2.5-12.5 h DibekacinNeonate: ~ 10-45 h Netilmicin Tobramicin Streptomycin 10-15 hPeak 1-2 h after IM Peak 15-40 Trough 5 umol/L duration of infusion 48 h > 0.5 umol/L 72 h > 0.05 umol/L Immunosuppressants Cyclosporine 1 d Day 3 or 4 of therapy, then 100-200 ug/L twice weekly for few weeks and reduce to every 1-2 mo
 Aminoglycosides Amikacin Adults ( 30 y): ~ h(1 h after IM) Gentamicin Children: ~ h DibekacinNeonate: ~ h Netilmicin Tobramicin Streptomycin hPeak 1-2 h after IM Peak Trough 5 umol/L duration of infusion 48 h > 0.5 umol/L 72 h > 0.05 umol/L Immunosuppressants Cyclosporine 1 d Day 3 or 4 of therapy, then ug/L twice weekly for few weeks and reduce to every 1-2 mo")
36
Drug Time to steady state Sampling time Therapeutic range (mg/L) Antiarrhythmics Disopyramide 1-2 d Trough 2-5 Lidocaine 1 h after LD 2 h after LD 1.5-5 5-10 h (no LD)6-12 h (no LD) Procainamide/NAPA Adult (no LD) Immediately after IV LD Procainamide 4-10 : normal renal 15-25 h2 h after start of IV infusion, NAPA 6-20 : renal insuff 30-65 h once more during 24 h period Oral: peak (1-4 h) and trough Quinidine 2 d Trough 2-5 Cardiac Glycosides Digitoxin 1 mo 8-24 h 13- 25 ug/L Digoxin 5-7 d 8-24 h 0.9- 2.2 ug/L May be longer in renal insufficiency
 Antiarrhythmics Disopyramide 1-2 d Trough 2-5 Lidocaine 1 h after LD 2 h after LD h (no LD)6-12 h (no LD) Procainamide/NAPA Adult (no LD) Immediately after IV LD Procainamide 4-10 : normal renal h2 h after start of IV infusion, NAPA 6-20 : renal insuff h once more during 24 h period Oral: peak (1-4 h) and trough Quinidine 2 d Trough 2-5 Cardiac Glycosides Digitoxin 1 mo 8-24 h ug/L Digoxin 5-7 d 8-24 h ug/L May be longer in renal insufficiency")
37
Drug Time to steady state Sampling time Therapeutic range (mg/L) Antiepileptics Carbamazepine 2-6 d Trough 4-10 Ethosuximide 1-2 wk Any time 40- 100 Phenobarbital 3 wk Any time 15- 40 Phenytoin 7 d 2-4 h 10- 20 Valproate 2-3 d Trough 50- 100 Bronchodilators Theophylline Adult: 2 d IV: 30 min after IV LD 10-20 Children: 1-2 d : 4-6 h after beginning therapy Infants: 1-5 d : 12-18 h after beginning therapy Newborn: 120 h Oral: peak Premy: 150 h 2 h after rapid release prep 4 h after sustained release prep
 Antiepileptics Carbamazepine 2-6 d Trough 4-10 Ethosuximide 1-2 wk Any time Phenobarbital 3 wk Any time Phenytoin 7 d 2-4 h Valproate 2-3 d Trough Bronchodilators Theophylline Adult: 2 d IV: 30 min after IV LD Children: 1-2 d : 4-6 h after beginning therapy Infants: 1-5 d : h after beginning therapy Newborn: 120 h Oral: peak Premy: 150 h 2 h after rapid release prep 4 h after sustained release prep")
38
Drug Time to steady state Sampling time Therapeutic range (mg/L) Analgesics Aspirin 1-5 d 1-3 h 150- 300 (antiinflam.) 250- 400 (rheumatic fev) Paracetamol 4 h postingestion > 200 toxicity 12 h postingestion > 50 Psychoactive Drugs Amitriptyline 3-8 d Trough 150-250 ug/L Imipramine 2-5 d Trough 150-250 ug/L Nortriptyline 4-20 d Trough 50- 150 ug/L Lithium 3-7 d Trough 0.6- 1.2 mEq/L
 Analgesics Aspirin 1-5 d 1-3 h (antiinflam.) (rheumatic fev) Paracetamol 4 h postingestion > 200 toxicity 12 h postingestion > 50 Psychoactive Drugs Amitriptyline 3-8 d Trough ug/L Imipramine 2-5 d Trough ug/L Nortriptyline 4-20 d Trough ug/L Lithium 3-7 d Trough mEq/L")
Similar presentations





>")

>")











