Download presentation
Presentation is loading. Please wait.

1
PHL 417 1- PART-I IMMUNOMODULATORS 2- PART II ANTI-PARASITES

3
GOALS OF IMMUNOTHERAPY IN ORGAN TRANSPLANTS
IMMUNOSUPPRESSANTS GOALS OF IMMUNOTHERAPY IN ORGAN TRANSPLANTS 1- Prevention of the immune response example: acute rejection and vascular remodeling 2- prevention of complications of immunodeficiency Such as infections and malignancy 3-minimize drug induced and other non-immune toxicities

4
Foreign Cell or Protein
CLONAL EXPANSION Produce CD4 Then CD8 T RECOGNITION Antigen presentation Ag-presenting cell Antigen processing Antigen uptake Foreign Cell or Protein

5
Receptor-associated tyrosine kinases (ZAP-70, lck & fyn)
T-CELL RECEPTOR TCR Phospholipase C DAG phosphatidyl inositol IP3 NF-B & Other TF’s ? PKC Ca2+ NF-AT P Calcineurin NF-AT Oct P Oct IL-2

6
APC Steps Towards T-cell Clonal Expansion 4th step Proliferation
2nd STEP 3rd step APC Receptor Binding & Signaling Cell - cell signaling (IFN-, IL-1) Autocrine signaling (IL-2) 4th step Proliferation
 Autocrine. signaling. (IL-2) 4th step Proliferation.")
8
IFN- TNF- IMMUNOPHARMACOLOGY 0psonized bacteria Macrophage APC
B lymphocyte T lymphocyte IL-4,IL-5 IL-2 IL-2 TH1 TH2 IFN- TNF- IFN- IFN- Plasma Cells: IgG IgM IgA - IgD Activated Macrophage Activated Cytotoxic T cell Activated NK cells Memory B Cells CELL-MEDIATED IMMUNITY HUMORAL IMMUNITY

9
TYPE IMMUNE RESPONSES A- Primary immune system - it is efectively inhibited by immunosuppressants especially before antigen exposure i- celluar mediated immunity * mediated by T-lymphocyted * it causes lysis for foreign cell (cytotoxic cells) * Responsible for Organ transplant Rejection Ii- Humoral immune response * mediated by B-lymphocytes to produce Antibodies B- Secondary immune response (delayed) -it is in the memory of T-cells (CD8) - It is fast (1-3 days) in response It also has cellular & humoral immunity
 * Responsible for Organ transplant Rejection. Ii- Humoral immune response. * mediated by B-lymphocytes to produce Antibodies. B- Secondary immune response (delayed) -it is in the memory of T-cells (CD8) - It is fast (1-3 days) in response. It also has cellular & humoral immunity.")
10
CLASSIFICATION OF IMMUNOSUPPRESSANTS 1- INHIBIT INTERLEUKIN-2 PRODUCTION (calcineurin inhibitors) Cyclosporine, tacrolimus 2-INHIBIT INTERLEUKIN-2 ACTION Sirolimus , Everolimus, Mycophenolate{CELLCEPT}, Azathioprine(imuran) 3- INHIBIT CYTOKINE GENE EXPRESSION Glucocorticoid
 3- INHIBIT CYTOKINE GENE EXPRESSION. Glucocorticoid.")
11
4- ALKYLATING CYTOTOXIC AGENTS
- Cyclophosphamide, (methotrexate), chlorambucil 5- BLOCK T- CELL SURFACE MOLEUCULE INVOLVED IN SIGNALING Immunoglobulins Antibody against IL-2 RECEPTORS (Bsiliximab, Simulect ®) OKT3 (Muromonab) Rh0[d] immunoglobulin (Gamulin Rh ®)
, chlorambucil. 5- BLOCK T- CELL SURFACE MOLEUCULE INVOLVED IN SIGNALING. Immunoglobulins. Antibody against IL-2 RECEPTORS (Bsiliximab, Simulect ®) OKT3 (Muromonab) Rh0[d] immunoglobulin (Gamulin Rh ®)")
12
Sirolimus IL-2 Cyclosporin Tacrolimus Glucocorticoids Mycophenolate
Anti-CD3 Cyclosporin Tacrolimus Glucocorticoids Sirolimus IL-2 Mycophenolate Mitogenesis Glucocorticoids IL-2

13
Preventing IL-2-driven clonal expansion
Prevent TCR signaling for IL-2 gene transcription: CYCLOSPORIN & TACROLIMUS GLUCOCORTICOIDS Prevent mitogenic response to IL-2R stimulation Sirolimus & Mycophenolate, IMURAN Prevent activation of T-cell Via TCR Anti-TCR Antibody IL-2R IL-2 IL-2 mRNA Degradation GLUCOCORTICOIDS Mitogenesis IL-2

14
CYCLOSPORIN MECHANISM OF ACTION Antigen binds to T cell receptor (TCR) -- Ca intracellular Ca +calmodulin stimulates phospatase, calcineurin activation of transcription factors --transcription of IL-2 gene CYCLOSPORIN binds to cytosolic protein, cyclophilin (immunophilin) Drug-immunophilin complex INHIBITS CALCINEURIN and blocks transcription of IL-2 gene
 Drug-immunophilin complex INHIBITS CALCINEURIN and blocks transcription of IL-2 gene.")
15
Receptor-associated tyrosine kinases (ZAP-70, lck & fyn)
TCR Phospholipase C DAG phosphatidyl inositol IP3 NF-B & Other TF’s ? PKC Ca2+ NF-AT P NF-AT Calcineurin Oct P Oct IL-2

17
ACTION OF CYCLOSPORIN OR TACROLIMUS
Cyclophilin Cyclo Cyclo Oct P NF-AT P CALCINEURIN NF-AT Oct NF-AT Oct AP-1 NF-B OAP IL-2

18
ACTION OF CYCLOSPORIN OR TACROLIMUS
Cyclophilin Cyclo Cyclo Oct P NF-AT P Cyclo Calcineurin NF-AT Oct NF-AT Oct AP-1 NF-B OAP IL-2

19
CYCLOSPORIN ADVERSE EFFECTS
Increase risk of infection Nephrotoxicity Liver dysfunction Regular blood level monitoring to avoid kidney and liver toxicity Hirsutism Gum hypertrophy

20
TACROLIMUS (FK506) Mechanism of action similar to cyclosporin
At cellular level, it binds to FK binding protein (FKBP) which inhibits cytoplasmic phosphatase, calcineurin activation of transcription factor -- IL-2 gene activation
 which inhibits cytoplasmic phosphatase, calcineurin activation of transcription factor -- IL-2 gene activation.")
21
TACROLIMUS (FK506) Tacolimus can be given orally or intravenously FOR LIVER TRANSPLANT Half-life is 7 hrs It is 99 % metabolised in the liver It is active in preventing organ transplant rejection Adverse effects are similar to Cyclosporin

22
SIROLIMUS (RAPAMYCIN)
It Binds to intracellular immunophilin FKBP does not interfere with IL-2 gene transcription But the complex binds to and modulates the activity of Sirolimus effector protein Inhibits mitogenic response to IL-2 leading to Interferes with IL-2 signal transduction pathway blocking the cell cycle of activated T cell at G2 stage Does not inhibit IL-2 or IL-2 Receptor Does not inhibit calcineurin Resulting in: a decreased clonal proliferation of T cells

23
Preventing IL-2-driven clonal expansion
IL-2R Prevent mitogenic response to IL-2R stimulation Sirolimus (Rapamycin) Mitogenesis IL-2
 Mitogenesis. IL-2.")
24
SIROLIMUS (RAPAMUNE®)
ADVERSE EFFECTS Hyperlipidemia (hypercholesterolemia 38%)-57%)may requires statins & gemfibrozil Anemia 27-37% may require iron & erythropoietin Thrombocytopenia Hypertension Peripheral edema 54%-64% Increased incidence of nephrotoxicity if given with cyclosporin
-57%)may requires statins & gemfibrozil. Anemia 27-37% may require iron & erythropoietin. Thrombocytopenia. Hypertension. Peripheral edema 54%-64% Increased incidence of nephrotoxicity if given with cyclosporin.")
25
EVEROLIMUS (CERTICAN®)
MOA It acts at post IL-2 Receptor by blocking p70 s6 Kinase which involve cellular proliferation signal Leads to arrest cell cycle at the G1-S phase (similar to sirolimus) It is complementary to calcineurin inhibitor Which favor long-term graft survival
 It is complementary to calcineurin inhibitor. Which favor long-term graft survival.")
26
GLUCOCORTICOIDS are potent immunosuppressive and anti-inflammatory agents Suppress inflammatory reaction Suppress immune response Decrease clonal expansion of T& B cells and cytokine secreting T cells Decrease the production and action of cytokines e.g. interleukins, TNF , gM-CsF Decrease the generation of IgG

27
MECHANISM OF ACTION GLUCOCORTICOIDS
Steroid interact with cytosolic receptors activated receptor ,form steroid-receptor complexs Move into nucleus, bind to steroid responsive elements in the DNA Either repress transcription of or induce transcription of particular genes

28
Suppression of transcription OF IL-2 Reduced IL-2 mRNA stability
Glucocorticoids Suppression of transcription OF IL-2 Reduced IL-2 mRNA stability ( IL-2 mRNA Degradation)
")
29
GLUCOCORTICOID CLINICAL USES
As anti-inflammatory & immuno- suppressive therapy Asthma, allergic rhinitis, eczema, severe drug allergic reaction, rheumatoid arthritis ,organ transplant In neoplastic disease Hodgkin’s disease, acute lymphocytic leukaemia Replacement therapy In adrenal insufficiency

30
ADVERSE EFFECTS Suppress response to injury or infection
Suppress patients capacity to synthesize corticosteroids Metabolic effect Water and electrolyte imbalance Osteoporosis GI bleeding hyperglycemia

31
CYCLOPHOSPHAMIDE is a nitrogen mustard, an alkylating agent
Is inactive until metabolised by the liver into its active phosphoamide mustard Have alkyl groups which can cross link to two nucleophilic site of the DNA---defective replication Resulting in subsequent cell death

33
CYCLOPHOSPHAMIDE Has pronounced effect on the lymphocytes
Usually given orally for Autoimmune diseases ADVERSE EFFECTS: Depress bone marrow function GI disturbance Toxic metabolite acrolein Haemorrhagic cystitis

34
AZATHIOPURINE (IMURAN®)
It is metabolised to give mercapturine which is a purine analog interferes with purine synthesis and is cytotoxic on the dividing cell Inhibit clonal prolifeation in the induction phase of the immune response Inhibits both cell mediated and antibody mediated immune reactions

36
USED AZATHIOPURINE MAJOR SIDE EFFECT:
- in organ transplant to prevent rejection - Autoimmune diseases with glucocorticoids MAJOR SIDE EFFECT: - suppress bone marrow - Hepatotoxicity - Retinopathy

37
MYCOPHENOLATE a- Mofetil salt CELLCEPT ®
B- sodium salt (enteric coated) MYOFORTIC® Administered orally and is well absorbed A semisynthetic derivative of fungal antibiotic Converted to mycophenolic acid
 MYOFORTIC® Administered orally and is well absorbed. A semisynthetic derivative of fungal antibiotic. Converted to mycophenolic acid.")
38
Mycophenolate mofetil
HCl OCH3 CH3 OH O N esterase Mycophenolate mofetil (prodrug) COOH OCH3 CH3 OH O Mycophenolate
 COOH. OCH3. CH3. OH. O. Mycophenolate.")
39
Mycophenolic Acid 1- MOA
Inhibitor of de-novo guanosine monophosphate synthesis B and T cells depend on de-novo synthesis: -lack salvage pathway for guanine recovery Other cells have salvage pathway Specific inhibition of DNA synthesis, RNA synthesis & other GTP or cGMP requiring pathways

40
5-phosphoribosyl-1-pyrophosphate (PRPP)
Ribose-5P + ATP 5-phosphoribosyl-1-pyrophosphate (PRPP) Guanine Guanosine MP Inosine MP Adenosine MP Salvage Pathway (deficient in T & B cells) IMP dehydrogenase Mycophenolate
 Guanine Guanosine MP Inosine MP Adenosine MP. Salvage Pathway. (deficient in. T & B cells) IMP dehydrogenase. Mycophenolate.")
41
2- DRUG INTERACTION Magnesium and aluminium impairs absorption 3- USES - Trial used in kidney transplant with cyclosporine and steroids - Autoimmune diseases

42
4- ADVERSE EFFECTS Peptic ulcer & esophagitis Hypercholestrolemia Diarrhea

43
IMMUNOSUPPRESSANT REGIMENS
1- Basiliximab, cyclosporin, prednisolone 2- Basiliximab, Azathioprine, cyclosporin, prednisolone 3- Basiliximab, MMF, cyclosporin, prednisolone

44
4- Basiliximab, Everolimus, cyclosporin, prednisolone
5- Basiliximab, Sirolimus, cyclosporin, prednisolone **************************************** Basiliximab 20 mg divided into two doses: First dose should be given on day 0 and second dose given on day 4 if needed

45
IMMULOGLOBULINS Antibodies against human lymphocytes or their surface protein can have significant immunosupressant action

46
IMMULOGLOBULINS Antibodies against human lymphocytes or their surface protein can have significant immunosupressant action

47
POLYCLONAL ANTIBODIES
Binds to protein on the surface of lymphocyte triggering the complement response - lysis of the lymphocyte Indiscriminate action on all T cells EXAMPLE ANTI-THYMPHOCYTE Lymphocyte immune globulin ( killer cell) immunoglobulin (ATG, Atgam ®) Immunizing horse with human Thymphocyte
 immunoglobulin (ATG, Atgam ®) Immunizing horse with human Thymphocyte.")
48
ATG (Atgam ®) MOA - Eliminate antigen –reactive T-lymphocytes (killer cells CLINICAL USES 1- Prevention & treatment of acute renal and other organ allograft rejection 2- aplastic anemia who is not candidate for bone marrow transplant

49
ATG (Atgam ®) ADVERSE EFFECTS - FEVER - Allergic reaction
Therefore, it is premedicated by paracetamol & diphenhydramine & glucocorticoids

50
MONOCLONAL ANTIBODIES
Direct against surface components of T cells CD3 proteins with antigen receptors Example : Muromonab-CD3 (Orthoclone ®)
")
51
Muromonab-CD3 (Orthoclone ®)OKT3
1- MOA It binds with T-cell receptor-associated CD3 glycoprotein 2- CLINICAL USES Acute allograft rejection resistant to conventional therapy

52
Muromonab-CD3 (Orthoclone ®)OKT3
3- ADVERSE EFFECTS First dose effects flu-like symptoms (cytokine release syndrome) Manifested by fever, respiratory dystress Hypervolemic pulmonary edema
 Manifested by fever, respiratory dystress. Hypervolemic pulmonary edema.")
53
Rh[d] immunoglobulin (Gamulin®)
MOA: - Immunoglobulin against Rh antigen D Which prevents the interactions between the Rh antigen and maternal (mother) immune system CLINICAL USES Prophylaxis in Erythroblastosis fetalis Idiopathic thrombocytopenia
![Rh[d] immunoglobulin (Gamulin®)](http://slideplayer.com/slide/4472642/14/images/53/Rh%5Bd%5D+immunoglobulin+%28Gamulin%C2%AE%29.jpg "MOA: - Immunoglobulin against Rh antigen D. Which prevents the interactions between the Rh antigen and maternal (mother) immune system. CLINICAL USES. Prophylaxis in Erythroblastosis fetalis. Idiopathic thrombocytopenia.")
54
infliximab, Remicade ®]
MOA: Antibody against tumor necrosis factor alpha (TNF alpha) USED: - for crohn’s disease - Rheumatoid arthritis with methotrexate who inadequate respond to methotrexate alone CONTRAINDICATED: - CHF - & TUBERCULOSIS
![infliximab, Remicade ®]](http://slideplayer.com/slide/4472642/14/images/54/infliximab%2C+Remicade+%C2%AE%5D.jpg "MOA: Antibody against tumor necrosis factor alpha (TNF alpha) USED: - for crohn’s disease. - Rheumatoid arthritis with methotrexate who inadequate respond to methotrexate alone. CONTRAINDICATED: - CHF. - & TUBERCULOSIS.")
55
ETANERCEPT (Enbrel ®) MOA: it binds with TNF and
blocks its interaction with cell surface receptor CLINICAL USE - for rheumatoid arthritis & crohn.s disease

56
Daclizumab (Zenapax ® ) Basiliximab (Simulect ® )
MOA: IL-2 receptors antibody USE: in combination with other standard immunosuppressant such as: Cyclosporin, and glucorticoids It reduces the incidence of acute renal rejection ADVERSE EFFECTS: NO CRS

57
Interferon Type-I A- Interferon Alpha (prod. by leukocytes)
(antiviral (hepatitis C, interferon alfa-2b ), antiproliferative) malignant melanoma, renal cell carcinoma, hairy cell leukemia, Kaposi’s sarcoma B- Interferon Beta (prod. by fibroblasts) (antiviral, antiproliferative) relapsing type Multiple Sclerosis Type-II Interferon Gamma (prod. by lymphocytes) (stimulates NK cells and macrophages) chronic granulomatous disease
, antiproliferative) malignant melanoma, renal cell carcinoma, hairy cell leukemia, Kaposi’s sarcoma. B- Interferon Beta (prod. by fibroblasts) (antiviral, antiproliferative) relapsing type Multiple Sclerosis. Type-II. Interferon Gamma (prod. by lymphocytes) (stimulates NK cells and macrophages) chronic granulomatous disease.")
58
Interferon Many of these are in clinical use and are given intramuscularly or subcutaneously Recombinant forms of alpha interferon include: Alpha-2a drug name Roferon Alpha-2b drug name Intron A Alpha-n1 drug name Wellferon Alpha-n3 drug name AlferonN Alpha-con1 drug name Infergen Pegasys is recombinant interferon alpha-2a that is covalently conjugated with bis-monomethoxy polyethylene glycol (PEG)
")
59
Alpha-2a drug name Roferon
Uses in the treatment of patients with chronic hepatitis C Hairy cell leukemia AIDS-related Kaposi's sarcoma. Side Effects Depressive illness and suicidal behavior, including suicidal ideation, suicide attempt, and suicides,

60
Interferon Beta-1a drug name Avonex Beta-1b drug name Betaseron
Recombinant forms of beta interferon include: Beta-1a drug name Avonex Beta-1b drug name Betaseron Recombinant forms of gamma interferon include: Interferon Gamma (Actimmunex®)
")
61
Interferon Beta Mechanism of Action
Reduce the production of the TNFa , known to induce damage to myelin Reduce inflammation by: Switching cytokine production from type 1 (pro-inflammatory) to type 2 (anti-inflammatory) cells Decrease antigen presentation, to reduce the attack on myelin Reduce the ability of immune cells to cross the blood-brain barrier,
 to type 2 (anti-inflammatory) cells. Decrease antigen presentation, to reduce the attack on myelin. Reduce the ability of immune cells to cross the blood-brain barrier,")
62
Interferons : Avonex (Interferon -1a) manufacture by biogen, usa
Indication: relapsing forms of MS Dose: 30 mcg IM once weekly Reduces rate of clinical relapse Reduces the development of new lesions May delay progression of disability

63
Interferons : Rebif (Interferon -1a)
Indication: relapsing/remitting forms of MS Dose: 22 or 44 mcg SC 3 times per week Decreases frequency of relapse Delays the increase in the volume of lesions May delay progression of disability

64
Interferons : Betaseron (interferon beta-1b Bayer HealthCare Pharmaceuticals
Indication: Relapsing forms of MS Dose: 8 million IU SC every other day Reduces rate of clinical relapse Reduces the development of new lesions Delays the increase in the volume of lesions

65
Side Effects of Interferons
Common: Flu-like symptoms Chills Fever Muscle aches Asthenia (weakness) Betaseron and Rebif have injection site reactions
 Betaseron and Rebif have injection site reactions.")
66
Side Effects of Interferons
Uncommon: Severe depression Suicide Seizures Cardiac effects Anemia Elevated liver enzymes Severe hepatic injury, including cases of hepatic failure, has been reported in patients taking Avonex

67
PART II ANTI-PARASITES

68
ANTI-PARASITES 1- Drugs used in the treatment of Schisomiasis
2- Drugs used in the treatment of Malaria 3- Drugs used in the treatment of Amoebiasis & Filariasis 4- Drugs used in the treatment of Ascariasis & Oxyyuriasis 5- Drugs used in the treatment of Toxoplasmosis 6- Drugs used in the treatment of Tapeworms infections & Giardiasis

69
ANTI-PARASITES Disease 1- Drugs used in the treatment of Schisomiasis
Schistosoma Disease Schistosoma causes schistosomiasis. A- Schistosoma mansoni and Schistosoma japonicum affect the gastrointestinal tract B- whereas Schistosoma haematobium affects the urinary tract.

70
schistosomiasis The three species can be distinguished by the appearance of their eggs in the microscope: S. mansoni eggs have a prominent lateral spine

71
Schistosomiasis S. japonicum eggs have a very small lateral spine

72
Schistosomiasis S. haematobium eggs have a terminal spine the veins draining the urinary bladder. Schistosomes are

73
schistosomiasis cercariae Eggs are eliminated with feces or urine .
Under optimal conditions the eggs hatch and release miracidia which swim and penetrate specific snail intermediate hosts . The stages in the snail include 2 generations of sporocysts and the p cercariae roduction of cercariae

74
Schistosomiasis Upon release from the snail, the infective cercariae swim, penetrate the skin of the human host , and shed their forked tail, becoming schistosomulae . The schistosomulae migrate through several tissues and stages to their residence in the veins Adult worms in humans reside in the mesenteric venules in various locations,

75
Schistosomiasis For instance, S. japonicum is more frequently found in the superior mesenteric veins draining the small intestine and S. mansoni occurs more often in the superior mesenteric veins draining the large intestine . However, both species can occupy either location, and they are capable of moving between sites

76
Schistosomiasis The eggs are moved progressively
toward the lumen of the intestine (S. mansoni and S. japonicum) Eggs eliminated with feces
 Eggs eliminated with feces.")
77
Schistosomiasis S. haematobium most often occurs in the venous plexus of bladder , but it can also be found in the rectal venules. The eggs are moved progressively toward the bladder and ureters (S. haematobium), and are eliminated with urine .
, and are eliminated with urine. .")
78
Schistosomiasis Pathology of S. mansoni and S. japonicum schistosomiasis includes: - Katayama fever - hepatic perisinusoidal egg granulomas - Symmers’ pipe stem periportal fibrosis - portal hypertension - occasional embolic egg granulomas in brain or spinal cord.

79
Schistosomiasis Pathology of S. haematobium schistosomiasis includes:
- hematuria - scarring, calcification - squamous cell carcinoma - occasional embolic egg granulomas in brain or spinal cord.

80
Schistosomiasis Human contact with water is thus necessary for infection by schistosomes. Various animals, such as dogs, cats, rodents, pigs, hourse and goats, serve as reservoirs for S. japonicum, and dogs for S. mekongi.

82
A: Male and female Schistosoma mansoni adults
A: Male and female Schistosoma mansoni adults. The female lives in the male's schist (shown as a ventral opening) (6x). B: Clonorchis sinensis adult (6x). C: Paragonimus westermani adult (0.6x). D: S. mansoni cercaria (300x).
 (6x). B: Clonorchis sinensis adult (6x). C: Paragonimus westermani adult (0.6x). D: S. mansoni cercaria (300x).")
83
A: Male and female Schistosoma mansoni adults
A: Male and female Schistosoma mansoni adults. The female lives in the male's schist (shown as a ventral opening) (6x). B: Clonorchis sinensis adult (6x). C: Paragonimus westermani adult (0.6x). D: S. mansoni cercaria (300x).
 (6x). B: Clonorchis sinensis adult (6x). C: Paragonimus westermani adult (0.6x). D: S. mansoni cercaria (300x).")
84
Symptoms and Signs Cercarial Dermatitis Following cercarial penetration localized erythema develops progress to a pruritic maculopapular rash that persists for some days. Dermatitis can be caused by human schistosomes and, in non-tropical areas, by bird schistosomes that cannot complete their life cycle in humans (swimmer's itch).
.")
85
Symptoms and Signs Acute Schistosomiasis (Katayama Syndrome) A febrile illness may develop 2–8 weeks after exposure in first time (naive immune system) most commonly after heavy infection with S mansoni or S japonicum. Presenting symptoms and signs include acute onset of fever; headache; myalgias; cough; malaise; urticaria
 most commonly after heavy infection with S mansoni or S japonicum. Presenting symptoms and signs include acute onset of fever; headache; myalgias; cough; malaise; urticaria.")
86
Symptoms and Signs Acute Schistosomiasis (Katayama Syndrome) diarrhea, which may be bloody hepatosplenomegaly; lymphadenopathy; and pulmonary infiltrates. Localized lesions may occasionally cause severe manifestations, including CNS abnormalities and death. Acute schistosomiasis usually resolves in 2–8 weeks.

87
Symptoms and Signs Chronic Schistosomiasis Many infected persons have light infections and are asymptomatic but an estimated 50–60% have symptoms 5–10% have advanced organ damage. Asymptomatic infected children may suffer from anemia and growth retardation

88
Symptoms and Signs Chronic Schistosomiasis Symptomatic patients with intestinal schistosomiasis typically experience: abdominal pain fatigue Diarrhea hepatomegaly. .

89
Symptoms and Signs Chronic Schistosomiasis Over years develop: anorexia weight loss weakness colonic polyps and features of portal hypertension

90
Symptoms and Signs Chronic Schistosomiasis Late manifestations include: hematemesis from esophageal varices hepatic failure pulmonary hypertension. Urinary schistosomiasis may present within months of infection with hematuria and dysuria, most commonly in children and young adults.

91
Symptoms and Signs Chronic Schistosomiasis Fibrotic changes in the urinary tract can lead to hydroureter hydronephrosis bacterial urinary infections ultimately, kidney disease or bladder cancer.

92
Treatment of schistosomiasis
No specific therapy is available for the treatment of schistosomal dermatitis or Katayama syndrome. Antihistamines and corticosteroids may be helpful in ameliorating their more severe manifestations. In the late stage of schistosomiasis, therapy is directed at interrupting egg deposition by killing or sterilizing the adult worms.

93
Treatment of schistosomiasis
Several anthelmintic agents may be used. Praziquantel which is active against all three species of schistosomes, is the agent of choice. Unfortunately, several recent reports have suggested increased resistance to this single-dose oral agent in areas where it has been used in mass therapy programs

94
Treatment of schistosomiasis
S mansoni infections acquired in such areas may be treated with oxamniquine. Use of this agent is contraindicated in pregnancy. Multiple anthelmintic drugs are used

95
Treatment of schistosomiasis
Praziquantel Biltricide® (600 mg) - 20 mg/kg twice per day in 4-hour intervals for 1 day for S. mansoni and S. haematobium Praziquantel - 20 mg/kg three times per day in 4-hour intervals for 1 day for S. mekongi and S. japonica
 - 20 mg/kg twice per day in 4-hour intervals for 1 day for S. mansoni and S. haematobium. Praziquantel mg/kg three times per day in 4-hour intervals for 1 day for S. mekongi and S. japonica.")
96
Treatment of schistosomiasis
ALTERNATIVE TREATMENT Metrifonate 10 mg/kg orally every 14 days for three doses Oxamniquine 15 mg/kg orally twice daily for 2 days

97
Treatment of schistosomiasis
ALTERNATIVE TREATMENT Metrifonate 10 mg/kg orally every 14 days for three doses Oxamniquine 15 mg/kg orally twice daily for 2 days

98
Praziquantel Uses Trematode (Fluke) Infections Schistosomiasis Praziquantel is used for the treatment of schistosomiasis (bilharziasis) caused by all Schistosoma species pathogenic to humans. Praziquantel is effective against all stages of Schistosoma infection including the acute phase and the chronic phase
 caused by all Schistosoma species pathogenic to humans. Praziquantel is effective against all stages of Schistosoma infection including the acute phase and the chronic phase.")
99
Praziquantel Praziquantel is administered orally.
The tablets should not be chewed but can be halved or quartered to allow administration of individualized doses.

100
Praziquantel Mechanism of Action It causes focal vacuolization and subsequent disintegration of worms praziquantel increases permeability of the liver fluke tegument to calcium, presumably by interfering with the mechanism that regulates calcium binding or transport across the tegumental membrane.

101
Adverse Reactions Praziquantel
1- CV: Arrhythmia (including AV blocks, bradycardia, ectopic rhythms 2- CNS: Dizziness; headache; malaise; asthenia, somnolence, GI: Abdominal discomfort with or without nausea; abdominal pain, 4- HYPERSENSITIVITY: Due to death of parasite triggers immune system Increased liver enzymes .

102
METRIFONATE (TRICHLORFON)
Metrifonate is a safe, low-cost alternative drug for the treatment of Schistosoma haematobium infections. It is not active against S mansoni or S japonicum. It is not available in the USA. Basic Pharmacology Metrifonate, an organophosphate compound It transform to dichlorvos, its active metabolite.

103
METRIFONATE (TRICHLORFON)
The mode of action It is cholinesterase inhibition. This inhibition temporarily paralyzes the adult worms resulting in their shift from the bladder venous plexus to small arterioles of the lungs where they are trapped, encased by the immune system, and die.

104
METRIFONATE (TRICHLORFON)
The drug is not effective against S haematobium eggs live eggs continue to pass in the urine for several months after all adult worms have been killed. Clinical Uses In the treatment of S haematobium, an oral dose of 7.5–10 mg/kg is given three times at 14-day intervals.

105
METRIFONATE (TRICHLORFON)
Cure rates on this schedule are 44–93%, with marked reductions in egg counts in those not cured. Metrifonate was also effective as a prophylactic agent when given monthly to children in a highly endemic area In mixed infections with S haematobium and S mansoni, metrifonate has been successfully combined with oxamniquine.

106
METRIFONATE (TRICHLORFON)
Adverse Reactions, Contraindications, & Cautions Some studies note mild and transient cholinergic symptoms Such as: nausea and vomiting, diarrhea, abdominal pain, bronchospasm

107
METRIFONATE (TRICHLORFON)
Adverse Reactions, Contraindications, & Cautions headache, sweating, fatigue, weakness, dizziness, and vertigo. These symptoms may begin within 30 minutes and persist up to 12 hours. .

108
METRIFONATE (TRICHLORFON)
Adverse Reactions, Contraindications, & Cautions Metrifonate should not be used after recent exposure to insecticides or drugs that might potentiate cholinesterase inhibition. Metrifonate is contraindicated in pregnancy.

109
Oxamniquine Oxamniquine second-line drug after praziquantel for the treatment of Schistosoma mansoni infection only. S. haematobium and S. japonicum are refractory to Oxamniquine

110
Oxamniquine Pharmacology and mechanism of action Oxamniquine is effective only in the treatment of Schistosoma(s)mansoni The drug may induce its action by inhibiting DNA synthesis. it inhibited the synthesis of macromolecules in sensitive parasites and not in the resistant ones
mansoni. The drug may induce its action by inhibiting DNA synthesis. it inhibited the synthesis of macromolecules in sensitive parasites and not in the resistant ones.")
111
Adverse effects of Oxamniquine 1- only significant common side effect reported is mild to moderate dizziness with or without drowsiness, reported by up to 40% of treated patients. It starts up to 3 hours after a dose and usually lasts for 3 to 6 hours. 2- Other side effects include nausea, vomiting,abdominal pain, and diarrhoea .

112
Adverse effects of Oxamniquine 3- Transient fever, 38 to 39°C, peripheral bloodeosinophilia and pulmonary infiltrates (Loeffler’s syndrome) 4- epileptiform convulsions 5- Discoloration of the urine from orange to red may follow after the drug treatment (mostlikely due to a metabolite) . This is transitory and harmless

113
Contraindications and precautions Oxamniquine
- Patients with pre-existing central nervous system disturbances such as epilepsy - or psychiatric disorders should be treated with caution. Adults A single dose of 15 mg/kg. Children (<4 years) A single total dose of 20 mg/kg or two doses of 10 mg/kg in one day separated by an intervalof 3 to 8 hours.
 A single total dose of 20 mg/kg or two doses of 10 mg/kg in one day separated by an intervalof 3 to 8 hours.")
114
Doses Oxamniquine Adults A single dose of 15 mg/kg.
Children (<4 years) A single total dose of 20 mg/kg or two doses of 10 mg/kg in one day separated by an intervalof 3 to 8 hours.
 A single total dose of 20 mg/kg or two doses of 10 mg/kg in one day separated by an intervalof 3 to 8 hours.")
115
ANT-MALARIA

116
ANT-MALARIA MALARIA * The plasmodia are sporozoa in which the sexual and asexual cycles of reproduction are completed in different host species The sexual phase occurs within the gut of mosquitoes. mosquitoes subsequently transmit the parasite while feeding on a human. Within the red blood cells (RBCs) of the vertebrate, the plasmodia reproduce asexually
 of the vertebrate, the plasmodia reproduce asexually.")
117
ANT-MALARIA MALARIA they eventually burst from the erythrocyte and invade other RBCs. This event produces periodic fever and anemia in the host, a disease process known as malaria.

118
ANT-MALARIA * Four species of plasmodium typically cause human
1- Plasmodium falciparum Because of the lack of a dormant live stage, P. falciparum does not cause relapses 2- P vivax, P. vivax and P. ovale responsible for late relapse over 6 to 11 months after acute infection 3- P ovale. 4- P malariae P. malariae infections may persist for decades within the bloodstream, but relapse does not occur, except under rare circumstances, such as trauma or surgery

119
ANT-MALARIA MALARIA P. falciparum can invade erythrocytes at all stages of maturation, and is responsible for severe disease with the greatest mortality. It is often drug resistant. Because of the lack of a dormant live stage, P. falciparum does not cause relapses. › P. vivax and P. ovale cause acute illness, and they are also responsible for late relapse over 6 to 11 months after acute infection. › P. malariae infections may persist for decades within the bloodstream, but relapse does not occur, except under rare circumstances, such as trauma or surgery.

120
ANT-MALARIA MALARIA - P falciparum is responsible for the majority of serious complications and deaths. - Drug resistance is an important therapeutic problem, most notably with P falciparum.

121
ANT-MALARIA MALARIA - Mosquito ingests gametocytes from blood of infected human Sporozoites from oocyst reach mosquito salivary glands

122
MALARIA ANT-MALARIA Humans infected by mosquito bite
Rapid infection of hepatocytes starts asexual cycle in humans

123
ANT-MALARIA MALARIA Erythrocytic cycle begins with merozoite attachment to RBC receptor Trophozoites multiply in RBC to form new merozoites In 48 to 72 hours, RBCs rupture, releasing merozoites to infect new RBCs Intrahepatic dormancy causes relapses with P vivax and P ovale

124
ANT-MALARIA MALARIA Erythrocytic cycle begins with merozoite attachment to RBC receptor Trophozoites multiply in RBC to form new merozoites In 48 to 72 hours, RBCs rupture, releasing merozoites to infect new RBCs Intrahepatic dormancy causes relapses with P vivax and P ovale

125
ANT-MALARIA MALARIA Sickle cell trait limits intensity of P falciparum infection Other hemoglobinopathies can also exert protection

126
MALARIA ANT-MALARIA Changes induced in erythrocyte membrane
Binding to endothelium may cause micro-infarcts Causing Complications due to capillary blockade can be fatal, particularly in the brain. - Causing Cerebral malaria

127
ANT-MALARIA An anopheline mosquito inoculates plasmodium sporozoites to initiate human infection

128
ANT-MALARIA An anopheline mosquito inoculates plasmodium sporozoites to initiate human infection

129
ANT-MALARIA Circulating sporozoites rapidly invade liver cells exoerythrocytic stage tissue schizonts mature in the liver. Merozoites are subsequently released from the liver and invade erythrocytes. Only erythrocytic parasites cause clinical illness. Repeated cycles of infection can lead to the infection of many erythrocytes and serious disease

130
ANT-MALARIA - Species of plasmodia differ significantly in their ability to invade subpopulations of erythrocytes P vivax and P ovale attack only immature cells (reticulocytes) whereas P malariae attacks only senescent cells(old RBC). During infection with these species, therefore, no more than 1% to 2% of the cell population is involved.
 whereas P malariae attacks only senescent cells(old RBC). During infection with these species, therefore, no more than 1% to 2% of the cell population is involved.")
131
ANT-MALARIA - P falciparum, in contrast, invades ALL RBCs, regardless of age and may produce very high levels of parasitemia West African ancestry lacks Duffy blood group antigen , are therefore resistant to vivax malaria. RBC sialoglycoprotein, particularly glycoprotein A, has been implicated as the P. falciparum receptor site.

132
Clinical signs and symptoms Fever
Fever, the hallmark of malaria appears to be initiated by the process of RBC rupture that leads to the liberation of a new generation of merozoites (sporulation). the fever might result from the release of interleukin-1 (IL-1) and/or tumor necrosis factor (TNF) from macrophages involved in the ingestion of parasitic or erythrocytic debris.
. the fever might result from the release of interleukin-1 (IL-1) and/or tumor necrosis factor (TNF) from macrophages involved in the ingestion of parasitic or erythrocytic debris.")
133
Clinical signs and symptoms
Fever The resulting fever is irregular and hectic. Synchronization of sporulation causes cyclic fever fever occurs in distinct paroxysms at 48-hour or, in the case of P malariae, 72-hour intervals

134
Anemia Parasitized erythrocytes are phagocytosed by a stimulated reticuloendothelial system or RBCs are destroyed at the time of sporulation. At times, the anemia is disproportionate to the degree of parasitism. Depression of marrow function, sequestration of erythrocytes within the enlarging spleen, and accelerated clearance of nonparasitized cells all appear to contribute to the anemia.

135
Anemia Intravascular hemolysis, though uncommon, may occur, particularly in falciparum malaria. When hemolysis is massive, hemoglobinuria develops, resulting in the production of dark urine. This process in conjunction with malaria is known as blackwater fever.

136
Circulatory Changes The high fever results in significant vasodilatation. In falciparum malaria, vasodilatation leads to a decrease in the effective circulating blood volume and hypotension P falciparum impairs the microcirculation and precipitate tissue hypoxia, lactic acidosis, and hypoglycemia. Although all deep tissues are involved, the brain is the most intensely affected.

137
Central nervous system malaria.
This small cerebral blood vessel is blocked with many parasitized erythrocytes adherent to the endothelium.

138
Cytokines Elevated levels of IL-1 and TNF are consistently found in patients with malaria. TNF levels increase with parasite density, and high concentrations appear harmful. TNF has been shown to cause up-regulation of endothelial adhesion molecules

139
Cytokines high concentrations might precipitate cerebral malaria by increasing the sequestration of P falciparum–parasitized erythrocytes in the cerebral vascular endothelium. Alternatively, excessive TNF levels might precipitate cerebral malaria by directly inducing hypoglycemia and lactic acidosis. Elevated cytokine levels contribute to injury

140
Thrombocytopenia is common in malaria and appears to be related to both splenic pooling and a shortened platelet lifespan. Both direct parasitic invasion and immune mechanisms may be responsible. There may be an acute transient glomerulonephritis in falciparum malaria and progressive renal disease in chronic P malariae malaria. These phenomena probably result from the host immune response, with deposition of immune complexes in the glomeruli. Thrombocytopenia and nephritis common

141
The incubation period between the bite of the mosquito and the onset of disease is approximately 2 weeks. With P malariae and with strains of P vivax in temperate climates, however, this period is often more prolonged. Individuals who contract malaria while taking antimalarial suppressants may not experience illness for many months. In the interval between entry into the country and onset of disease exceeds 1 month in 25% of P falciparum infections 6 months in a similar proportion of P vivax cases.

142
The clinical manifestations of malaria vary with the species of plasmodia but typically include:
chills, fever, splenomegaly, and anemia. The hallmark of disease is the malarial paroxysm. This manifestation begins with a cold stage, which persists for 20 to 60 minutes. During this time, the patient experiences continuous rigors and feels cold.

143
With the consequent increase in body temperature,
the rigors cease and vasodilatation commences, Ushering(REACH) in a hot stage . The temperature continues to rise for 3 to 8 hours, reaching a maximum of 40° to 41.7°C before it begins to fall. The wet stage consists of a decrease in fever and profuse sweating. It leaves the patient exhausted but otherwise well until the onset of the next paroxysm. Malarial paroxysm: cold, hot, wet stages
 in a hot stage . The temperature continues to rise for 3 to 8 hours, reaching a maximum of 40° to 41.7°C before it begins to fall. The wet stage consists of a decrease in fever and profuse sweating. It leaves the patient exhausted but otherwise well until the onset of the next paroxysm. Malarial paroxysm: cold, hot, wet stages.")
144
Typical paroxysms first appear in the second or third week of fever, when parasite sporulation becomes synchronized. In falciparum malaria, synchronization may never take place, and the fever may remain hectic and unpredictable. The first attack is often severe and may persist for weeks in the untreated patient.

145
In falciparum malaria, capillary blockage can lead to several serious complications.
When the central nervous system is involved (cerebral malaria) the patient may develop delirium, convulsions, paralysis, coma, and rapid death. Acute pulmonary insufficiency frequently accompanies cerebral malaria, killing about 80% of those involved.
 the patient may develop delirium, convulsions, paralysis, coma, and rapid death. Acute pulmonary insufficiency frequently accompanies cerebral malaria, killing about 80% of those involved.")
146
When splanchnic capillaries are involved
the patient may experience vomiting, abdominal pain, and diarrhea with or without bloody stools. Jaundice and acute renal failure are also common in severe illness. These pernicious syndromes generally appear when the intensity of parasitemia exceeds 100,000 organisms per cubic millimeter of blood. Most deaths occur within 3 days.

147
Termination of Acute Attack
Several agents can destroy asexual erythrocytic parasites. Chloroquine, a 4-aminoquinoline, has been the most commonly used. It acts by inhibiting the degradation of hemoglobin, thereby limiting the availability of amino acids necessary for growth. It has been suggested that the weak basic nature of chloroquine also acts to raise the pH of the food vacuoles of the parasite, inhibiting their acid proteases and effectiveness

148
Termination of Acute Attack
chloroquine-resistant strains of P falciparum are now widespread in Africa and Southeast Asia Resistance of chloroquine and other drugs now common with P falciparum Other schizonticidal agents include quinine/quinidine, antifolate–sulfonamide combinations, mefloquine, halofantrine, and the artemisinins. Unfortunately, resistance to all of these agents is increasing. The artemisinins are also unique in their capacity to reduce transmission by preventing gametocyte development.

149
Combination therapy may be necessary
Termination of Acute Attack There is a growing consensus that the most effective way to slow the further development of drug-resistant strains of P falciparum is to use one of the artemisinins in combination with quinine/quinidine, antifolate–sulfonamide compounds, mefloquine, or halofantrine. Combination therapy may be necessary

150
Radical Cure In P vivax and P ovale infections, hepatic schizonts persist and must be destroyed to prevent reseeding of circulating erythrocytes with consequent relapse. Primaquine, an 8-aminoquinaline, is used for this purpose. Some P vivax infections acquired in Southeast Asia and New Guinea fail initial therapy owing to relative resistance to this 8-aminoquinaline.

151
Radical Cure Retreatment with a larger dose of primaquine is usually successful. Unfortunately, primaquine may induce hemolysis in patients with glucose-6-phosphate dehydrogenase deficiency. Persons of Asian, African, and Mediterranean ancestry should thus be screened for this abnormality before treatment.

152
Radical Cure Chloroquine destroys the gametocytes of P vivax, P ovale, and Pmalariae but not those of P falciparum. Primaquine and artemisinins, however, are effective for this latter species. Primaquine used to destroy hepatic schizonts of P vivax and P ovale

153
Treatment: General Approach
It is preferable that treatment for malaria should not be initiated until the diagnosis has been established by laboratory investigations. "Presumptive treatment" without the benefit of laboratory confirmation should be reserved for extreme circumstances (strong clinical suspicion, severe disease, impossibility of obtaining prompt laboratory diagnosis). Once the diagnosis of malaria has been made, appropriate antimalarial treatment must be initiated immediately. Treatment should be guided by three main factors:
. Once the diagnosis of malaria has been made, appropriate antimalarial treatment. must be initiated immediately. Treatment should be guided by three main factors:")
154
The infecting Plasmodium species
The clinical status of the patient The drug susceptibility of the infecting parasites as determined by the geographic area where the infection was acquired and the previous use of antimalarial medicines

155
The infecting Plasmodium species:
Determination of the infecting Plasmodium species for treatment purposes is important for three main reasons. Firstly, P. falciparum and P. knowlesi infections can cause rapidly progressive severe illness or death while the other species, P. vivax, P. ovale, or P. malariae, are less likely to cause severe manifestations.

156
Secondly, P. vivax and P. ovale infections also require
treatment for the hypnozoite forms that remain dormant in the liver (Primaquine) and can cause a relapsing infection. Finally, P. falciparum and P. vivax species have different drug CENTERS FOR DISEASE CONTROL AND PREVENTION resistance patterns in differing geographic regions. For P. falciparum and P. knowlesi infections, the urgent initiation of appropriate therapy is especially critical
 and can cause a relapsing infection. Finally, P. falciparum and P. vivax species have different drug. CENTERS FOR DISEASE CONTROL AND PREVENTION. resistance patterns in differing geographic regions. For P. falciparum and P. knowlesi infections, the urgent initiation of appropriate therapy is especially critical.")
157
1- uncomplicated or severe malaria.
The clinical status of the patient: Patients diagnosed with malaria are generally categorized as having either 1- uncomplicated or severe malaria. Patients diagnosed with uncomplicated malaria can be effectively treated with oral antimalarials.

158
2- COMPLICATED MALARIA patients who have one or more of the following clinical criteria : a- impaired consciousness/coma b- severe normocytic anemia [hemoglobin<7] c- renal failure d- acute respiratory distress syndrome e- hypotension f- disseminated intravascular coagulation

159
2- COMPLICATED MALARIA g- spontaneous bleeding
h- acidosis, hemoglobinuria k- jaundice L- repeated generalized convulsions, and/or parasitemia of > 5%) are considered to have manifestations of more severe disease and should be treated aggressively with parenteral antimalarial therapy
 are considered to have manifestations of more severe disease and should be treated aggressively with parenteral antimalarial therapy.")
160
Treatment: Uncomplicated Malaria
P. falciparum or Species Not Identified – Acquired in Areas Without Chloroquine Resistance 1- Chloroquine. A chloroquine dose of 600 mg base (= 1,000 mg salt) should be given initially, followed by 300 mg base (= 500 mg salt) at 6, 24, and 48 hours after the initial dose for a total chloroquine dose of 1,500 mg base (=2,500 mg salt).
 should be given initially, followed by 300 mg base (= 500 mg salt) at 6, 24, and 48 hours after the initial dose for a total chloroquine dose of 1,500 mg base (=2,500 mg salt).")
161
Treatment: Uncomplicated Malaria
2- Alternatively, hydroxychloroquine may be used at a dose of 620 mg base (=800 mg salt) po given initially followed by 310 mg base (=400 mg salt) po at 6, 24, and 48 hours after the initial dose for a total hydroxychloroquine dose of 1,550 mg base (=2,000 mg salt). Prompt initiation of an effective regimen is vitally important and so using any one of the effective regimens that readily at hand would be the preferred strategy.
 po given initially followed by 310 mg base (=400 mg salt) po at 6, 24, and 48 hours after the initial dose for a total hydroxychloroquine dose of 1,550 mg base (=2,000 mg salt). Prompt initiation of an effective regimen is vitally important and so using any one of the effective regimens that readily at hand would be the preferred strategy.")
162
2- P. falciparum or Species Not Identified – Acquired in Areas With Chloroquine Resistance :
For P. falciparum infections acquired in areas with chloroquine resistance, four treatment options are available. The first two treatment options are : - MALARONE Tablet contains 250 mg of atovaquone and 100 mg of proguanil or artemether-lumefantrine (Coartem). These are fixed dose combination medicines that can be used for non-pregnant adult and pediatric patients. Both of these options are very efficacious.
. These are fixed dose combination medicines that can be used for non-pregnant adult and pediatric patients. Both of these options are very efficacious.")
163
3- Quinine sulfate plus doxycycline,
tetracycline, or clindamycin is the next treatment option. For the quinine sulfate combination options, quinine sulfate plus either doxycycline or tetracycline is generally preferred to quinine sulfate plus clindamycin because there are more data on the efficacy of quinine plus doxycycline or tetracycline. Quinine treatment should continue for 7 days for infections acquired in Southeast Asia and for 3 days for infections acquired in Africa or South America.

164
4- The fourth option, Mefloquine,
is associated with rare but potentially severe neuropsychiatric reactions when used at treatment doses. We recommend this fourth option only when the other options cannot be used. For pediatric patients, the treatment options are the same as for a adults except the drug dose is adjusted by patient weight.

165
If using a quinine-based regimen for children less than eight years old
* doxycycline and tetracycline are generally not indicated therefore, quinine can be given alone for a full 7 days regardless of where the infection was acquired

166
or given in combination with clindamycin as recommended above.
In rare instances, doxycycline or tetracycline can be used in combination with quinine in children less than eight years old if other treatment options are not available or are not tolerated, and the benefit of adding doxycycline or tetracycline is judged to outweigh the risk.

167
If infections initially attributed to "species not identified" are subsequently diagnosed as being due to P. vivax or P. ovale additional treatment with primaquine should be administered ( P. vivax and P. ovale) INORDER TO ERADICATE RESEEDING
 INORDER TO ERADICATE RESEEDING.")
168
P. malariae and P. knowlesi
There has been no widespread evidence of chloroquine resistance in P. malariae and P. knowlesi species therefore, chloroquine (or hydroxychloroquine) may still be used for both of these infections. In addition, any of the regimens listed above for the treatment of chloroquine-resistant malaria may be used for the treatment of P. malariae and P. knowlesi infections.
 may still be used for both of these infections. In addition, any of the regimens listed above for the. treatment of chloroquine-resistant malaria may be used for the treatment of P. malariae and P. knowlesi infections.")
169
P. vivax and P. ovale Chloroquine (or hydroxychloroquine) remains an effective choice for all P. vivax and P. ovale infections except for P. vivax infections acquired in Papua New Guinea or Indonesia. The regimens listed for the treatment of P. falciparum are also effective and may be used. Reports have confirmed a high prevalence of chloroquine-resistant P. vivax in these two specific areas(Papua New Guinea or Indonesia ). Rare cases of chloroquine-resistant P. vivax have also been documented in Burma (Myanmar), India, and Central and South America.
 remains an effective choice for all P. vivax and P. ovale infections except for P. vivax infections acquired in Papua New Guinea or Indonesia. The regimens listed for the treatment of P. falciparum are also effective and may be used. Reports have confirmed a high prevalence of chloroquine-resistant P. vivax in these two specific areas(Papua New Guinea or Indonesia ). Rare cases of chloroquine-resistant P. vivax have also been documented in Burma (Myanmar), India, and Central and South America.")
170
Persons acquiring P. vivax infections from regions other than Papua New Guinea or Indonesia should initially be treated with chloroquine. If the patient does not respond to chloroquine, treatment should be changed to one of the two regimens recommended for chloroquine-resistant P. vivax infections

171
Persons acquiring P. vivax infections in Papua New Guinea or Indonesia should initially be treated with a regimen recommended for chloroquine-resistant P. vivax infections. The three treatment regimens for chloroquine-resistant P. vivax infections are: A- quinine sulfate plus doxycycline or tetracycline B- or, Atovaquone-proguanil C- or mefloquine. These three treatment options are equally recommended.

172
In addition to requiring blood stage treatment, infections with P
In addition to requiring blood stage treatment, infections with P. vivax and P. ovale can relapse due to hypnozoites that remain dormant in the liver. To eradicate the hypnozoites patients should be treated with a 14-day course of primaquine CDC recommends a primaquine phosphate dose of 30 mg (base) by mouth daily for 14 days. Because primaquine can cause hemolytic anemia in persons with glucose-6-phosphate-dehydrogenase (G6PD) deficiency persons must be screened for G6PD deficiency prior to starting primaquine treatment.
 by mouth daily for 14 days. Because primaquine can cause hemolytic anemia in persons with glucose-6-phosphate-dehydrogenase (G6PD) deficiency. persons must be screened for G6PD deficiency prior to starting primaquine treatment.")
173
same as for adults except the drug dose is adjusted by patient weight.
For persons with borderline G6PD deficiency or as an alternate to the above regimen, primaquine may be given at the dose of 45 mg (base) orally one time per week for 8 weeks consultation with an expert in infectious disease and/or tropical medicine is advised if this alternative regimen is considered in G6PD-deficient persons. Primaquine must not be used during pregnancy. For pediatric patients, the treatment options are the same as for adults except the drug dose is adjusted by patient weight.
 orally one time per week for 8 weeks. consultation with an expert in infectious disease and/or tropical medicine is advised if this alternative regimen is considered in G6PD-deficient persons. Primaquine must not be used during pregnancy. For pediatric patients, the treatment options are the. same as for adults except the drug dose is adjusted by patient weight.")
174
For children less than 8 years old, doxycycline and tetracycline are generally not indicated
therefore, for chloroquine-resistant P. vivax, Mefloquine is the recommended treatment. If it is not available or is not being tolerated and if the treatment benefits outweigh the risks: atovaquone-proguanil or artemether-lumefantrine should be used instead.

175
Alternatives For Pregnant Women
Malaria infection in pregnant women is associated with high risks of both maternal and perinatal morbidity and mortality. pregnant women have a reduced immune response and therefore less effectively clear malaria infections. In addition, malaria parasites sequester and replicate in the placenta. Pregnant women are three times more likely to develop severe disease than non-pregnant women acquiring infections from the same area.

176
For pregnant women diagnosed with uncomplicated malaria
Malaria infection during pregnancy can lead to miscarriage, premature delivery, low birth weight, congenital infection, and/or perinatal death. For pregnant women diagnosed with uncomplicated malaria caused by P. malariae, P. vivax, P. ovale, or chloroquine-sensitive P. falciparum infection, prompt treatment with chloroquine (treatment schedule as with non-pregnant adult patients) is recommended. Alternatively, hydroxychloroquine may be given instead.
 is recommended. Alternatively, hydroxychloroquine may be given instead.")
177
For pregnant women diagnosed with uncomplicated malaria caused by chloroquine-resistant P. falciparum infection prompt treatment with either Mefloquine or a combination of quinine sulfate and clindamycin is recommended. Quinine treatment should continue for 7 days for infections acquired in Southeast Asia and for 3 days for infections acquired elsewhere; clindamycin treatment should continue for 7 days regardless of where the infection was acquired.

178
For pregnant women diagnosed with uncomplicated malaria caused by chloroquine-resistant P. vivax infection, prompt treatment with mefloquine is recommended. Doxycycline and tetracycline are generally not indicated for use in pregnant women. However, in rare instances, doxycycline or tetracycline can be used in combination with quinine if other treatment options are not available or are not being tolerated, and the benefit of adding doxycycline or tetracycline is judged to outweigh the risks.

179
as a pregnancy category C medications
According to its U.S. labels, atovaquone/proguanil and artemether-lumefantrine are classified: as a pregnancy category C medications and are generally not indicated for use in pregnant women because there are no adequate, well-controlled studies in pregnant women. However, for pregnant women diagnosed with uncomplicated malaria caused by chloroquine-resistant P. falciparum infection atovaquone/proguanil or artemether-lumefantrine may be used if other treatment options are not available or are not being tolerated, and if the potential benefit is judged to outweigh the potential risks.

180
For P. vivax or P. ovale infections, primaquine phosphate for radical treatment of hypnozoites should not be given during pregnancy. Pregnant patients with P. vivax or P. ovale infections should be maintained on chloroquine prophylaxis for the duration of their pregnancy. The chemoprophylactic dose of chloroquine phosphate is 300mg base (=500 mg salt) orally once per week. After delivery, pregnant patients with P. vivax or P. ovale infections who do not have G6PD deficiency should be treated with primaquine
 orally once per week. After delivery, pregnant patients with P. vivax or P. ovale infections who do not have G6PD deficiency should be. treated with primaquine.")
181
Treatment: Severe Malaria
Pregnant women diagnosed with severe malaria should be treated aggressively with parenteral antimalarial therapy Patients who are considered to have manifestations of more severe disease should be treated aggressively with parenteral antimalarial therapy regardless of the species of malaria seen on the blood smear. Oral antimalarial drugs are not recommended for the initial treatment of severe malaria.

182
Treatment: Severe Malaria
for the initial treatment of severe malaria. If severe malaria is strongly suspected but a laboratory diagnosis cannot be made at that time blood should be collected for diagnostic testing as soon as it is available and parenteral antimalarial drugs may be started.

183
Treatment: Severe Malaria
Since 1991, quinidine gluconate has been the only parenterally administered antimalarial drug available in the United States. It is recommended to give a loading dose of 6.25 mg base/kg (=10 mg salt/kg) of quinidine gluconate infused intravenously over 1-2 hours followed by a continuous infusion of mg base/kg/min (=0.02 mg salt/kg/min). An alternative regimen is an intravenous loading dose of 15mg base/kg (=24 mg salt/kg) of quinidine gluconate infused intravenously over 4 hours.
 of quinidine gluconate infused intravenously over 1-2 hours followed by a continuous infusion of mg. base/kg/min (=0.02 mg salt/kg/min). An alternative regimen is an intravenous loading dose of 15mg base/kg (=24 mg salt/kg) of quinidine gluconate infused intravenously over 4 hours.")
184
Treatment: Severe Malaria
every 8 hours, starting 8 hours after the loading dose . At least 24 hours of quinidine gluconate infusion (or 3 intermittent doses) are recommended once the parasite density is < 1% and the patient can take oral Medication the patient can complete the treatment course with an oral regimen such as oral quinine at the same dosage for uncomplicated malaria
 are recommended. once the parasite density is < 1% and the patient can take oral. Medication. the patient can complete the treatment course with an oral regimen such as oral quinine at the same dosage for uncomplicated malaria.")
185
Treatment: Severe Malaria
(for a combined treatment course of quinidine/quinine for 7 days for malaria acquired in Southeast Asia and 3 days for malaria acquired elsewhere). Other oral regimens such as atovaquone-proguanil or artemether-lumefantrine may be used instead of an oral quinine based regimen
. Other oral regimens such as atovaquone-proguanil or artemether-lumefantrine may be used instead of an oral quinine based regimen.")
186
Treatment: Severe Malaria
Initial (including loading) doses of parenteral quinidine do not need to be reduced in persons with renal failure. If renal failure persists or the patient does not improve clinically the maintenance dosage should be reduced by one third to one half on the third treatment day. As with treatment of uncomplicated P. falciparum, quinidine/quinine therapy should be combined with doxycycline, tetracycline, or clindamycin.
 doses of parenteral quinidine do not need to be reduced in persons with renal failure. If renal failure persists or the patient does not improve clinically. the maintenance dosage should be reduced by one third to one half on the. third treatment day. As with treatment of uncomplicated P. falciparum, quinidine/quinine therapy should be combined with doxycycline, tetracycline, or clindamycin.")
187
Treatment: Severe Malaria
If the patient is unable to tolerate oral therapy doxycycline (100mg every 12 hours) or clindamycin (5 mg base/kg every 8 hours) may be given intravenously until the patient can be switched to oral therapy. Rapid intravenous administration of doxycycline or clindamycin should be avoided. * If the patient can tolerate oral therapy, doxycycline (100 mg every 12 hours), tetracycline (250mg every 6 hours), or clindamycin (20 mg base/kg/day divided three times per day) for 7 days are options.
 or clindamycin (5 mg base/kg every 8 hours) may be given intravenously until the patient can be switched to oral therapy. Rapid intravenous administration of doxycycline or clindamycin. should be avoided. * If the patient can tolerate oral therapy, doxycycline (100 mg every 12 hours), tetracycline (250mg every 6 hours), or clindamycin (20 mg base/kg/day divided three times per day) for 7 days are options.")
188
Treatment: Severe Malaria
Parenteral quinidine gluconate is cardiotoxic and so a baseline EKG should be obtained before initiating therapy. Quinidine should be administered in an intensive care setting with continuous cardiac and frequent blood pressure monitoring. At the dosages required for the treatment of falciparum malaria, quinidine gluconate: may cause ventricular arrhythmia, hypotension, hypoglycemia, and prolongation of the QTc interval.

189
Treatment: Severe Malaria
The quinidine gluconate infusion should be slowed or stopped for an increase in the QRS complex by > 50%, a QTc interval > 0.6 seconds a QTc interval that is prolonged by more than 25% of the baseline value or hypotension unresponsive to fluid challenge. Because most deaths from severe malaria occur within the first hours, the goal of a loading dose is to quickly reach therapeutic concentrations at a time when they are needed most.

190
Treatment: Severe Malaria
Recent use of other drugs that may prolong the QTc interval (e.g., quinine or mefloquine) should be considered when determining whether a patient should receive a loading dose of quinidine gluconate. Because there is less evidence on which to base decisions with quinidine gluconate, recommendations for administration of a loading dose are based on experience with loading doses of quinine. A loading dose of quinidine gluconate should be given unless the patient has received more than 40 mg/kg quinine in the previous 2 days
 should be considered when determining whether a patient should receive a loading dose of quinidine gluconate. Because there is less evidence on which to base decisions with quinidine gluconate, recommendations for administration of a loading dose are based on experience with loading doses of quinine. A loading dose of quinidine gluconate should be given unless the patient has received more than 40 mg/kg quinine in the previous 2 days.")
191
Treatment: Severe Malaria
or has received mefloquine in the previous 12 hours. Consulting a cardiologist and a physician with experience in treating malaria is advised when treating malaria patients with quinidine gluconate. Glucose must be monitored closely as quinidine- (or quinine-) induced hyperinsulinemic hypoglycemia can occur.
 induced hyperinsulinemic. hypoglycemia can occur.")
192
Treatment: Severe Malaria
With the advent of newer anti-arrhythmic agents, quinidine gluconate has been dropped from many hospital formularies and fewer clinicians have experience with the drug. To ensure the availability of quinidine in health care facilities, hospital drug services need to maintain or add quinidine gluconate injection to formularies. If quinidine gluconate injection is not available on the hospital formulary, the hospital should be able to immediately locate a nearby health care facility that stocks it. If a local source cannot be found, quinidine gluconate should be requested from the local or regional distributor

193
Treatment: Severe Malaria
If quinidine is unavailable, or in patients with adverse effects or contraindications to quinidine, or in patients with a parasitemia >10% of baseline at 48 hours after initiation of IV quinidine, parenteral artesunate is available as an investigational new drug through CDC. If both quinidine and artesunate can be obtained in similar time frames the treating physician may choose either option.

194
Treatment: Severe Malaria
While exchange transfusion has not been proven beneficial in an adequately powered randomized controlled trial it has been an option in the treatment of severe malaria since 1974. CDC recommends that exchange transfusion be strongly considered for persons with a parasite density of more than 10% or if complications such as cerebral malaria, acute respiratory distress syndrome, or renal complications exist. Exchange transfusion is thought to have beneficial effects by removing infected red

195
Treatment: Severe Malaria
improving the rheological properties of blood, and reducing toxic factors such as parasite-derived toxins harmful metabolites, and cytokines. The risks of exchange transfusion include : fluid overload, febrile and allergic reactions, metabolic disturbances (e.g., hypocalcemia) red blood cell alloantibody sensitization transmissible infection, and line sepsis.
 red blood cell alloantibody sensitization. transmissible infection, and line sepsis.")
196
Treatment: Severe Malaria
The risks of exchange transfusion include : Thus, the potential benefits of exchange transfusion should be weighed against the risks. The parasite density should be monitored every 12 hours until it falls below 1%, which usually requires the exchange of 8-10 units of blood in adults

197
Treatment: Severe Malaria
The risks of exchange transfusion include : Thus, the potential benefits of exchange transfusion should be weighed against the risks. The parasite density should be monitored every 12 hours until it falls below 1%, which usually requires the exchange of 8-10 units of blood in adults

198
Mefloquine Treatment of mild to moderate malaria caused by mefloquine-susceptible strains of Plasmodium falciparum or P. vivax . Prevention of malaria caused by P. falciparum or P. vivax . Patients with acute P. vivax need subsequent treatment with 8-aminoquinolone to prevent relapse. Mechanism of action is unknown PREVENT INGESTION OF HEMOGLOBIN Contraindications Acute depression; history of psychosis or convulsions; hypersensitivity to the drug or related compounds (eg, quinine, quinidine). Pregnancy: Category C
. Pregnancy: Category C.")
199
Mefloquine Adverse effects mental status changes cardiac abnormalities

200
Chloroquine Mechanism of action Uses Prevention of Malaria
Chloroquine is used for prevention of malaria caused by Plasmodium malariae, P. ovale, P. vivax, or susceptible strains of P. falciparum. Mechanism of action Concentrates in parasite food vacuoles and prevents heme metabolism, thereby causing toxicity and cell death due to the buildup of soluble heme Chloroquine: GI upset; pruritus; visual disturbances; ECG changes Quinine: Cinchonism (tinnitus, headache, dizziness, nausea); Coombs’ positive hemolytic anemia
; Coombs’ positive hemolytic anemia.")
201
Quinine Treatment of uncomplicated P. falciparum malaria.
Uses Treatment of uncomplicated P. falciparum malaria. Mechanism of action Inhibits nucleic acid synthesis, protein synthesis, and glycolysis in Plasmodium falciparum and can bind with hemozoin in parasitized erythrocytes. Contraindications Prolonged QT interval G6PD deficiency myasthenia gravis optic neuritis

202
Quinine Adverse Reactions
CV: Atrial fibrillation, AV block, bradycardia QT prolongation Cinchonism pregnancy: Category C

203
Primaquine Mechanism of action Uses
Radical cure or prevention of relapse in vivax malaria; after termination of chloroquine phosphate suppressive therapy in areas where vivax malaria is endemic. Mechanism of action Primaquine acts against primary and latent hepatic stages of Plasmodium spp. and prevents relapses in P. vivax and P. ovale infections. It has gametocytocidal activity against P. falciparum and other Plasmodium species. primaquine is inactive against asexual blood stage parasites.

204
Primaquine Mechanism of action
Primaquine may be converted to electrophilic intermediates that act as oxidation-reduction mediators. Such activity could contribute to antimalarial effects by generating reactive oxygen species or by interfering with mitochondrial electron transport in the parasite Some strains of P. vivax can exhibit partial resistance to primaquine

205
Primaquine Adverse reaction Leukopenia
hemolytic anemia in G-6-PD deficiency methemoglobinemia in NADH methemoglobin reductase deficiency. Primaquine is not recommended because of the potential risk of haemolytic effects in the fetus.

206
USES: MALARONE ® Tablet contains:
250 mg of atovaquone and 100 mg of proguanil USES: MALARONE is indicated for the treatment of acute, uncomplicated P. falciparum malaria. MALARONE has been shown to be effective in regions where the drugs chloroquine, halofantrine, mefloquine, and amodiaquine may have unacceptable failure rates- presumably due to drug resistance. Prevention of Malaria: MALARONE is indicated for the prophylaxis of P. falciparum malaria, including in areas where chloroquine resistance has been reported

207
MALARONE ® Tablet contains:
250 mg of atovaquone and 100 mg of proguanil Mechanism of actions: Atovaquone is a selective inhibitor of parasite mitochondrial electron transport. Proguanil hydrochloride primarily exerts its effect by means of the metabolite cycloguanil, a dihydrofolate reductase inhibitor. Inhibition of dihydrofolate reductase in the malaria parasite disrupts deoxythymidylate synthesis.

208
MALARONE ® Tablet contains:
250 mg of atovaquone and 100 mg of proguanil Mechanism of actions: Activity In Vitro and In Vivo: Atovaquone and cycloguanil (an active metabolite of proguanil) are active against the erythrocytic and exoerythrocytic stages of Plasmodium spp. Enhanced efficacy of the combination compared to either atovaquone or proguanil alone was demonstrated in clinical studies in both immune and non-immune patients
 are active against the erythrocytic and exoerythrocytic stages of Plasmodium spp. Enhanced efficacy of the combination compared to either atovaquone or proguanil alone was demonstrated in clinical studies in both immune and non-immune patients.")
209
MALARONE ® Concomitant treatment with tetracycline has been associated with approximately a 40% reduction in plasma concentrations of atovaquone. Toxicities Hepatic Effects Elevations in AST and ALT have occurred In most patients, liver enzyme values returned to normal by day 28 of follow-up.

210
MALARONE ® Pregnancy Category C.
Atovaquone and proguanil may be used in pregnant women if the potential benefits outweigh the risks. CDC states that the drug may be used in pregnant women for treatment of uncomplicated malaria caused by chloroquine-resistant P. falciparum if other treatment options are not available or are not tolerated CDC states that the drug should not be used for prevention of malaria in pregnant women.

211
Coartem ® Coartem contains a fixed ratio of 1:6 parts of Artemether 20 mg and Lumefantrine 120 mg. Artemether is a semisynthetic chiral acetal derivative from artemisinin, Artemether is a prodrug that is rapidly converted to dihydroartemisinin isolated from the plant Artemisia annua. Lumefantrine is a racemic mixture of a synthetic fluorene derivative Similarl in structure to : (quinine, mefloquine, halofantrine), lumefantrine belongs to the aryl-aminoalcohol family.
, lumefantrine belongs to the aryl-aminoalcohol family.")
212
Coartem is not approved for the prevention of malaria
Artemether-Lumefantrine (Coartem ® ). INDICATIONS Treatment, including stand-by emergency treatment of children and infants with acute uncomplicated infections due to Plasmodium falciparum or mixed infections including P. falciparum. Because Coartem is effective against both drug-sensitive and drug-resistant P. falciparum it is also recommended for malaria infections acquired in areas where the parasites may be resistant to other antimalarials. Coartem is not approved for the prevention of malaria
. INDICATIONS. Treatment, including stand-by emergency treatment of children and infants with acute uncomplicated infections due to Plasmodium falciparum or mixed infections including P. falciparum. Because Coartem is effective against both drug-sensitive and drug-resistant P. falciparum it is also recommended for malaria infections acquired in areas where the parasites may be resistant to other antimalarials. Coartem is not approved for the prevention of malaria.")
213
Artemether-Lumefantrine (Coartem ® ). Mechanism of Actions:
The site of antiparasitic action of both components is the food vacuole of the malarial parasite where they are thought to interfere with the conversion of haem, a toxic intermediate produced during haemoglobin breakdown to the non-toxic haemozoin, malaria pigment. Lumefantrine is thought to interfere with the polymerisation processin

214
Mechanism of Actions: Artemether generates reactive metabolites as a result of the interaction between its peroxide bridge and haem iron. Both artemether and lumefantrine have a secondary action involving inhibition of nucleic acid- and protein synthesis within the malarial parasite. Data from in vitro and in vivo studies show that Coartem did not induce resistance. The antimalarial activity of the combination of lumefantrine and artemether in Coartem is greater than that of either substance alone.

215
Artemether-Lumefantrine (Coartem ® ) CONTRAINDICATIONS
First trimester of pregnancy in situations where other suitable and effective anti-malarials are available Patients with a family history of congenital prolongation of the QTc interval Patients taking drugs that are known to prolong the QTc interval such as: antiarrhythmics of classes IA and III

216
Artemether-Lumefantrine (Coartem ® ). CONTRAINDICATIONS
- neuroleptics, antidepressant agents, - certain antibiotics including some agents of the following classes: macrolides fluoroquinolones, imidazole, and triazole antifungal agents Patients with known disturbances of electrolyte balance e.g. hypokalaemia or hypomagnesaemia.

217
Artemether-Lumefantrine (Coartem ® ). Adverse Reactions
prolongation of the QT interval (prolonged heart palpitations signs of hypersensitivity skin rash, hives, other skin reactions rapid heartbeat difficulty breathing or swallowing, swelling of the lips, tongue, face, tightness or throat, hoarseness

218
Drugs used in the treatment of Amoebiasis
Amebiasis is a protozoal infection caused by pathologic strains of Entamoeba histolytica or Entamoeba dispar. Infection with these organisms leads to ulceration of the colon and diarrhea and, on occasion, liver abscess. ETIOLOGY Most people with the organism have no significant invasion of the colonic mucosa and are asymptomatic. These are called "cyst passers.“

219
Drugs used in the treatment of Amoebiasis
Disease is worldwide in distribution, but much more prevalent in underdeveloped nations with poor sanitation. Contaminated water or vegetables are often the source for infection in humans.

220
Drugs used in the treatment of Amoebiasis
Symptoms NONINVASIVE Symptoms of noninvasive disease are mild, with diarrhea only. INVASIVE Invasive disease is associated with crampy abdominal pain and bloody, mucoid diarrhea. • Fevers occur in one-third of patients. Fulminant disease with peritonitis and perforation as well as toxic megacolon is rare

221
Drugs used in the treatment of Amoebiasis
Symptoms INVASIVE AMEBIC LIVER ABSCESS This may present with fevers tenderness to palpation over the liver. Diarrhea and active amebic colitis are often not present at the time of abscess discovery. Rare rupture of the abscess may lead to peritonitis.

222
Drugs used in the treatment of Amoebiasis
1- ASYMPTOMATIC CYST PASSER WITHOUT INVASIVE DISEASE Iodoquinol 650 mg orally three times per day for 20 days Paromomycin 500 mg orally three times per day for 7 days

223
Drugs used in the treatment of Amoebiasis
ASYMPTOMATIC CYST PASSER WITHOUT INVASIVE DISEASE For mild to moderate GI symptoms oral metronidazole: 500 to 750 mg tid in adults (12 to 17 mg/kg tid in children) for 7 to 10 days is recommended. Metronidazole should not be given to pregnant women. Alcohol must be avoided because of the drug's disulfiram like effect
 for 7 to 10 days is recommended. Metronidazole should not be given to pregnant women. Alcohol must be avoided because of the drug s disulfiram like effect.")
224
Drugs used in the treatment of Amoebiasis
ASYMPTOMATIC CYST PASSER WITHOUT INVASIVE DISEASE Alternatively, tinidazole 2 g po once/day in adults (50 mg/kg [maximum 2 g] po once/day in children > 3 yr) for 3 days can be used. When taken with alcohol, tinidazole also has a disulfiram like effect and it should not be used during pregnancy in terms of GI adverse effects, it is generally better tolerated than metronidazole
 for 3 days can be used. When taken with alcohol, tinidazole also has a disulfiram like effect. and it should not be used during pregnancy. in terms of GI adverse effects, it is generally better tolerated than metronidazole.")
225
Drugs used in the treatment of Amoebiasis
For severe intestinal and extraintestinal amebiasis metronidazole Metronidazole: 750 mg tid in adults (12 to 17 mg/kg tid in children) for 7 to 10 days is used. Alternatively, tinidazole 2 g po once/day in adults (50 mg/kg [maximum 2 g] po once/day in children > 3 yr) for 5 days can be used.
 for 7 to 10 days is used. Alternatively, tinidazole 2 g po once/day in adults (50 mg/kg [maximum 2 g] po once/day in children > 3 yr) for 5 days can be used.")
226
Drugs used in the treatment of Amoebiasis
For severe intestinal and extraintestinal amebiasis, metronidazole A course of metronidazole or tinidazole should be followed by a 2nd oral drug to eradicate residual cysts in the lumen. Options are: Iodoquinol or Paromomycin OR Diloxanide

227
Drugs used in the treatment of Amoebiasis
Asymptomatic people who pass E. histolytica cysts should be treated with : Paromomycin or iodoquinol or diloxanide furoate

228
Drugs used in the treatment of Amoebiasis
LIVER ABSCESS Metronidazole 750 mg orally or intravenously three times per day for 10 days followed by iodoquinol 650 mg orally three times per day for 20 days

229
Drugs used in the treatment of Amoebiasis
For severe intestinal and extraintestinal amebiasis, metronidazole A course of metronidazole or tinidazole should be followed by a 2nd oral drug to eradicate residual cysts in the lumen. Options are Iodoquinol 650 mg po tid in adults (10 to 13 mg/kg [maximum of 2 g/day] tid in children) for 20 days Paromomycin 8 to 11 mg/kg tid for 7 days Diloxanide furoate 500 mg po tid in adults (7 mg/kg po tid in children) for 10 days Diloxanide furoate is not available commercially in the US. Therapy should include rehydration with fluid and electrolytes and other supportive measures. Asymptomatic people who pass E. histolytica cysts should be treated with paromomycin ,iodoquinol , or diloxanide furoate (see above for doses). Although metronidazole andtinidazole have some activity against E. histolytica cysts, it is not sufficient for them to be used for cyst eradication. Treatment is not necessary for E. dispar or E. moshkovskii infections. However, if fecal antigen testing to differentiate them from E. histolytica is not available, the decision to treat is made clinically (eg, by the likelihood of exposure to E. histolytica). Iodoquinol 650 mg orally three time per day for 20 days › Paromomycin 500 mg orally three times per day for 7 days LIVER ABSCESS • Metronidazole 750 mg orally or intravenously three times per day for 10 days, followed by iodoquinol 650 mg orally three times per day for 20 days For a large abscess (>3 cm), aspiration and needle drainage is indicated. Smaller abscesses resolve with medical treatment.
 for 20 days. Paromomycin 8 to 11 mg/kg tid for 7 days. Diloxanide furoate 500 mg po tid in adults (7 mg/kg po tid in children) for 10 days. Diloxanide furoate is not available commercially in the US. Therapy should include rehydration with fluid and electrolytes and other supportive measures. Asymptomatic people who pass E. histolytica cysts should be treated with paromomycin ,iodoquinol , or diloxanide furoate (see above for doses). Although metronidazole andtinidazole have some activity against E. histolytica cysts, it is not sufficient for them to be used for cyst eradication. Treatment is not necessary for E. dispar or E. moshkovskii infections. However, if fecal antigen testing to differentiate them from E. histolytica is not available, the decision to treat is made clinically (eg, by the likelihood of exposure to E. histolytica). Iodoquinol 650 mg orally three time per day for 20 days. › Paromomycin 500 mg orally three times per day for 7 days. LIVER ABSCESS. • Metronidazole 750 mg orally or intravenously three times per day for 10 days, followed by iodoquinol 650 mg orally three times per day for 20 days. For a large abscess (>3 cm), aspiration and needle drainage is indicated. Smaller abscesses resolve with medical treatment.")
230
Drugs used in the treatment of Filariasis
Caused by filarial nematodes – Wuchereria bancrofti – Brugia malayi – Brugia timori – Mansonella perstans – Onchocerca volvulus – Loa loa – Mansonella streptocerca – Mansonella ozzardi

231
Drugs used in the treatment of Filariasis
Humans are infected by bites of infected mosquitoes Larvae move to the lymphatics and lymph nodes where they mature over months The thread-like adult worms can live for many years and produce large numbers of microfilariae, which are infective to mosquitoes Microfilariae are released into the circulation, usually at night except in the South Pacific where microfilaremia peaks during daylight hours

232
Drugs used in the treatment of Filariasis

233
Drugs used in the treatment of Filariasis
Acute Disease Initial manifestation is often acute lymphangitis, with fever, painful lymph nodes, edema, and inflammation spreading peripherally from involved lymph nodes Lymphangitis and lymphadenitis of the upper and lower extremities is common Genital involvement occurs with W bancroftiinfection – Epididymitis – Orchitis – Scrotal pain and tenderness

234
Drugs used in the treatment of Filariasis
Chronic disease Most common manifestation is swelling of the extremities or genitals due to chronic lymphatic inflammation and obstruction Extremities become increasingly swollen,

235
Drugs used in the treatment of Filariasis
Diethylcarbamazine – Drug of choice, but cannot cure infections due to its limited action against adult worms – Therapy may be accompanied by allergic symptoms (eg, fever, headache, malaise, hypotension, and bronchospasm) probably due to release of antigens from dying worms – Therefore, begin treatment with lower dosage and escalate over first 4 days – Use ivermectin plus albendazole instead
 probably due to release of antigens from dying worms. – Therefore, begin treatment with lower dosage and escalate over first 4 days. – Use ivermectin plus albendazole instead.")
236
Drugs used in the treatment of Filariasis
Drainage of hydroceles provides symptomatic relief Doxycycline (100–200 mg/day orally for 4–6 weeks) – Kills obligate intracellular Wolbachia bacteria, leading to death of adult filarial worms Secondary bacterial infections much be treated
 – Kills obligate intracellular Wolbachia bacteria, leading to death of adult filarial worms. Secondary bacterial infections much be treated.")
237
Drugs used in the treatment of Oxyyuriasis(pinworm)
The intestinal nematode (roundworm) Enterobius vermicularis causes pinworm infection. MODE OF TRANSMISSION Fecal-oral ingestion of the egg, direct person-to-person contact, or indirect contact via contaminated hands, dust, food, or objects (such as bedding, clothing, toys, bathwater, toilet seats) Eggs can remain infective indoors for 2–3 weeks. Humans are the only known natural host animal pinworms do not infect humans.
 Enterobius vermicularis causes pinworm infection. MODE OF TRANSMISSION. Fecal-oral ingestion of the egg, direct person-to-person contact, or indirect contact via contaminated hands, dust, food, or objects (such as bedding, clothing, toys, bathwater, toilet seats) Eggs can remain infective indoors for 2–3 weeks. Humans are the only known natural host. animal pinworms do not infect humans.")
238
Drugs used in the treatment of Oxyyuriasis
CLINICAL PRESENTATION asymptomatic, common symptoms include: nocturnal perianal and perineal pruritus and restless sleep. Urethritis, vaginitis, salpingitis, hepatitis, or peritonitis may occur if adult worms migrate from the perineum to other sites. Secondary bacterial infection of skin may occur from scratching.

239
Drugs used in the treatment of Oxyyuriasis
Diagnosis is made by identifying the worm or its eggs by: Direct visualization of female adult worms near anus or on sheets or underclothing or pajamas at night, about 2–3 hours after patient falls asleep. Microscopic identification of worm eggs by using the “scotch tape test” on 3 consecutive mornings. The adhesive side of clear transparent—not translucent—cellophane tape is pressed to the skin around the anus when patient first awakens, before washing or bathing. The tape is then directly affixed to a microscope slide and examined under low power for eggs.

240
Drugs used in the treatment of Oxyyuriasis
Eggs and worms are rarely found in routine stool samples. TREATMENT . Drugs of choice are mebendazole, albendazole, or pyrantel pamoate. Treat all household contacts and caretakers at the same time as the patient. Daily morning bathing removes a large proportion of eggs; change underclothing and bedding frequently and launder in hot water.

241
Drugs used in the treatment of Oxyyuriasis
Reinfection occurs easily; instruction about prevention is mandatory to eliminate continued infection and spread. PREVENTIVE MEASURES FOR TRAVELERS Strict observance of good hand hygiene is essential (proper handwashing; maintaining clean

242
Drugs used in the treatment of Ascariasis
Ascariasis lumbricoides is the largest intestinal nematode parasite of humans, reaching up to 40 cm in length. Most infected individuals have low worm burdens and are asymptomatic. Clinical disease arises from larval migration in the lungs or effects of the adult worms in the intestines. Life Cycle Adult worms live in the lumen of the small intestine. Mature female Ascaris worms are extraordinarily fecund, each producing up to 240,000 eggs a day, which pass with the feces. Ascarid eggs, which are remarkably resistant to environmental stresses, become infective after several weeks of maturation in the soil and can remain infective for years. After infective eggs are swallowed, larvae hatched in the intestine invade the mucosa migrate through the circulation to the lungs, break into the alveoli, ascend the bronchial tree, and return—through swallowing—to the small intestine where they develop into adult worms. Between 2 and 3 months elapse between initial infection and egg production. Adult worms live for 1–2 years.

243
Drugs used in the treatment of Ascariasis
Ascarid eggs, which are remarkably resistant to environmental stresses, become infective after several weeks of maturation in the soil and can remain infective for years. After infective eggs are swallowed, larvae hatched in the intestine invade the mucosa migrate through the circulation to the lungs, break into the alveoli, ascend the bronchial tree, and return—through swallowing—to the small intestine where they develop into adult worms. Between 2 and 3 months elapse between initial infection and egg production. Adult worms live for 1–2 years.

244
Drugs used in the treatment of Ascariasis
Transmission typically occurs through fecally contaminated soil and is due either to a lack of sanitary facilities or to the use of human feces as fertilizer. Infection outside endemic areas, though uncommon, can occur when eggs on transported vegetables are ingested. Clinical Features During the lung phase of larval migration, 9–12 days after egg ingestion, patients may develop an irritating nonproductive cough and burning substernal discomfort that is aggravated by coughing or deep inspiration. Dyspnea and blood-tinged sputum are less common. In heavy infections small-bowel obstructionof surgical acute abdomen.

245
Drugs used in the treatment of Ascariasis
Treatment: Ascariasis Ascariasis should always be treated to prevent potentially serious complications. Albendazole (400 mg once), mebendazole (100 g twice daily for 3 days or 500 mg once), or ivermectin (150–200 g/kg once) is effective. These medications are contraindicated in pregnancy, however. Pyrantel pamoate (11 mg/kg once; maximum, 1 g) is safe in pregnancy. Nitazoxanide (7.5 mg/kg once; maximum, 500 mg) has also been used in ascariasis.
, mebendazole (100 g twice daily for 3 days or 500 mg once), or ivermectin (150–200 g/kg once) is effective. These medications are contraindicated in pregnancy, however. Pyrantel pamoate (11 mg/kg once; maximum, 1 g) is safe in pregnancy. Nitazoxanide (7.5 mg/kg once; maximum, 500 mg) has also been used in ascariasis.")
246
Drugs used in the treatment of Toxoplasmosis
caused by protozoan Toxoplasma gondii. Infection in humans is usually asymptomatic. Severe infections usually occur in an immunocompromised patient or by the transplacental passage of parasites from an infected mother to the fetus (congenital toxoplasmosis).
.")
247
Drugs used in the treatment of Toxoplasmosis
There are two stages in the life cycle of T. gondii: The sexual phase results in the formation of oocysts in the cat's intestine. The sporulated oocysts are ingested by an intermediate host (e.g., a human). Bradyzoites or sporozoites are released and transformed to rapidly dividing tachyzoites which can infect any organ. Immune responses are able to eliminate most of the tachyzoites, and a tissue cyst is formed.
. Bradyzoites or sporozoites are released and transformed to rapidly dividing tachyzoites. which can infect any organ. Immune responses are able to eliminate most of the tachyzoites, and a tissue cyst is formed.")
248
Drugs used in the treatment of Toxoplasmosis
Cases are caused by eating undercooked meat or contaminated vegetables ingestion of sporulated oocysts from contaminated soil. Congenital toxoplasmosis Only one of five pregnant women infected with T. gondii develop clinical signs. Women who are seropositive before pregnancy usually are protected against acute infection and do not give birth to congenitally infected neonates.

249
Drugs used in the treatment of Toxoplasmosis
If the acute infection in the mother goes untreated congenital infection occurs in approximately 15% of the fetuses during the first trimester, 30% of the fetuses during the second trimester, and 60% of the fetuses during the third trimester. Toxoplasmosis and HIV infection In areas with high seroprevalence for toxoplasmosis 25% to 50% of all AIDS patients, who are not receiving antiretroviral therapy, will develop CNS toxoplasmosis.

250
Drugs used in the treatment of Toxoplasmosis
The combination of pyrimethamine plus sulfadiazine is the regimen of choice for acute therapy. For acute therapy, the usual dose is 4 to 8 g/d of sulfadiazine and a loading dose of 100 to 200 mg, followed by 50 to 75 mg/d of pyrimethamine Leucovorin should always be coadministered with pyrimethamine to prevent the folinic acid deficiency and ameliorate the hematologic toxicity of pyrimethamine. Duration of treatment should be individualized, but it usually is for 6 to 8 weeks. .

251
Drugs used in the treatment of Toxoplasmosis
ALTERNATIVE TREATMENT Pyrimethamine (accompanied by folinic acid) combined with clindamycin is clearly an effective and acceptable alternative. The combination of clarithromycin with pyrimethamine also seems effective . Azithromycin may have a role in combination with pyrimethamine. Steroids may produce transient clinical and radiographic improvement in CNS
 combined with clindamycin is clearly an effective and acceptable alternative. The combination of clarithromycin with pyrimethamine also seems effective . Azithromycin may have a role in combination with pyrimethamine. Steroids may produce transient clinical and radiographic improvement in CNS.")
252
Drugs used in the treatment of Tapeworms infections
Life cycle of Taenia saginata

253
Adult beef tapeworm (Taenia saginata).
.")
254
Drugs used in the treatment of Tapeworms infections
Life cycle Mature segments are detached and pass out with the faeces disintegrate and the eggs are set free and eaten by the intermediate host (the pig). Humans are occasionally infected by cysticerci (cysticercosis), as are other primates, sheep and dogs. The oncosphere penetrates the gut wall and enters the bloodstream, settling in the muscles, especially the heart, and becomes a cysticercus (5–20 mm) known as cysticercus cellulosae.
. Humans are occasionally infected by cysticerci. (cysticercosis), as are other primates, sheep and dogs. The oncosphere penetrates the gut wall and enters the bloodstream, settling. in the muscles, especially the heart, and becomes a cysticercus. (5–20 mm) known as cysticercus cellulosae.")
255
Drugs used in the treatment of Tapeworms infections
Taenia Species • T. saginata Microbiologic Characteristics • A tapeworm Incubation Period • Eggs appear in the stool 10 to 14 weeks after infection with T. saginata. • Symptoms (if any) may delay even more. Epidemiology • Worldwide • More frequent in populations where beef is consumed insufficiently cooked
 may delay even more. Epidemiology. • Worldwide • More frequent in populations where beef is consumed insufficiently cooked.")
256
Drugs used in the treatment of Tapeworms infections
Taenia Species • T. saginata Infections • Beef tapeworm infection, which is usually asymptomatic. It may cause mild gastrointestinal symptoms. Treatment • Niclosamide 2 g PO in a single dose Alternative Treatment • Praziquantel 25 mg/kg PO (children, 10–15 mg/kg) in a single dose Prevention • Thorough cooking of beef
 in a single dose. Prevention. • Thorough cooking of beef.")
257
Drugs used in the treatment of Tapeworms infections
Taenia Species • Taenia solium the central nervous system (CNS) is the most significant site for infection The pig (intermediate host) ingests the egg and larvae are formed. The larvae travel via the bloodstream throughout the pig and achieve high concentrations in the muscle.
 is the most significant site for infection. The pig (intermediate host) ingests the egg and larvae are formed. The larvae travel via the bloodstream throughout the pig and achieve high concentrations in the muscle.")
258
Drugs used in the treatment of Tapeworms infections
• Taenia solium Clinical Manifestations • Seizures Headache • Possible signs of hydrocephalus Symptoms depend on the number, size, and location of the lesions. • Intraventricular disease leads to hydrocephalus Subretinal or intravitreal disease may lead to blindness. • Cysts may present in the orbit, leading to blindness. COMPLICATIONS • Hydrocephalus • Seizures • Blindness

259
Drugs used in the treatment of Tapeworms infections
Taenia Species • Taenia solium FOR NEUROCYSTERCERCOSIS • Praziquantel 50 mg/kg every day for 15 days • Albendazole 15 mg/kg every day for 1 to 4 weeks Expect an inflammatory reaction to the medications; steroids are often given with treatment to alleviate inflammation in the CNS, which can cause headache and seizures Antiseizure medications may be considered. FOR TAPEWORM INFECTION ALONE • Praziquantel 10 mg/kg, single dose.

260
Drugs used in the treatment of Giardiasis
An infection of the upper small bowel with Giardia lamblia, which may cause diarrhea. ETIOLOGY • A flagellate protozoon, G. lamblia (Giardia intestinalis), that exists in trophozoite and cyst forms. The infective form is the cyst of the parasite. Cysts are infective as soon as passed and remain infective in water for a few months. When ingested by a new host, they excyst in the upper gastrointestinal tract and liberate trophozoites, which attach with their suckers to the surface of the duodenal or jejunal mucosa and multiply by binary fission. When trophozoites drop off the duodenal and jejunal mucosa, they are carried on with the contents in the gut and encyst.
, that exists in trophozoite and cyst forms. The infective form is the cyst of the parasite. Cysts are infective as soon as passed and remain infective in water for a few months. When ingested by a new host, they excyst in the upper gastrointestinal tract and liberate trophozoites, which attach with their suckers to the surface of the duodenal or jejunal mucosa and multiply by binary fission. When trophozoites drop off the duodenal and jejunal mucosa, they are carried on with the contents in the gut and encyst.")
261
Drugs used in the treatment of Giardiasis
Commonest where standards of sanitation are low Infection is usually sporadic and spreads from person to person directly by the fecal–oral route or indirectly by ingestion of fecally contaminated water or food. Epidemics mainly occur where gross Giardia cyst contamination of water supplies occurs. Epidemics resulting from person-to-person transmission sometimes occur in childcare centers, in institutions for mentally retarded persons Humans are the principal reservoir of infection, but wild beavers and other animals have also been found to be infected in North America.

262
Drugs used in the treatment of Giardiasis
SYMPTOMS The main symptom is diarrhea may continue for weeks or months if untreated. Stool: pale, offensive, bulky, with much flatus but no blood or mucus Crampy abdominal pain, urgent call to stool Bloating and steatorrhea

263
Drugs used in the treatment of Giardiasis
Metronidazole (with efficacy up to 80%–95%) Avoid alcohol intake, as it may produce side effects such as headache and flushing. In children, dosage modified: 5 mg/kg tid for 7 days Tinidazole (with efficacy up to 90%): not applicable in the United States In adults: A single dose of 2 g is usually effective.
 Avoid alcohol intake, as it may produce side effects such as headache and flushing. In children, dosage modified: 5 mg/kg tid for 7 days. Tinidazole (with efficacy up to 90%): not applicable in the United States. In adults: A single dose of 2 g is usually effective.")
264
Drugs used in the treatment of Giardiasis
ALTERNATIVE TREATMENT Mepacrine/quinacrine Furazolidone (with efficacy up to 80%) Caution: Haemolysis in patients with G-6PD deficiency TREATMENT FAILURE A failure rate of about 10% to 20% is expected.
 Caution: Haemolysis in patients with G-6PD deficiency. TREATMENT FAILURE. A failure rate of about 10% to 20% is expected.")
265
Thank you

Similar presentations


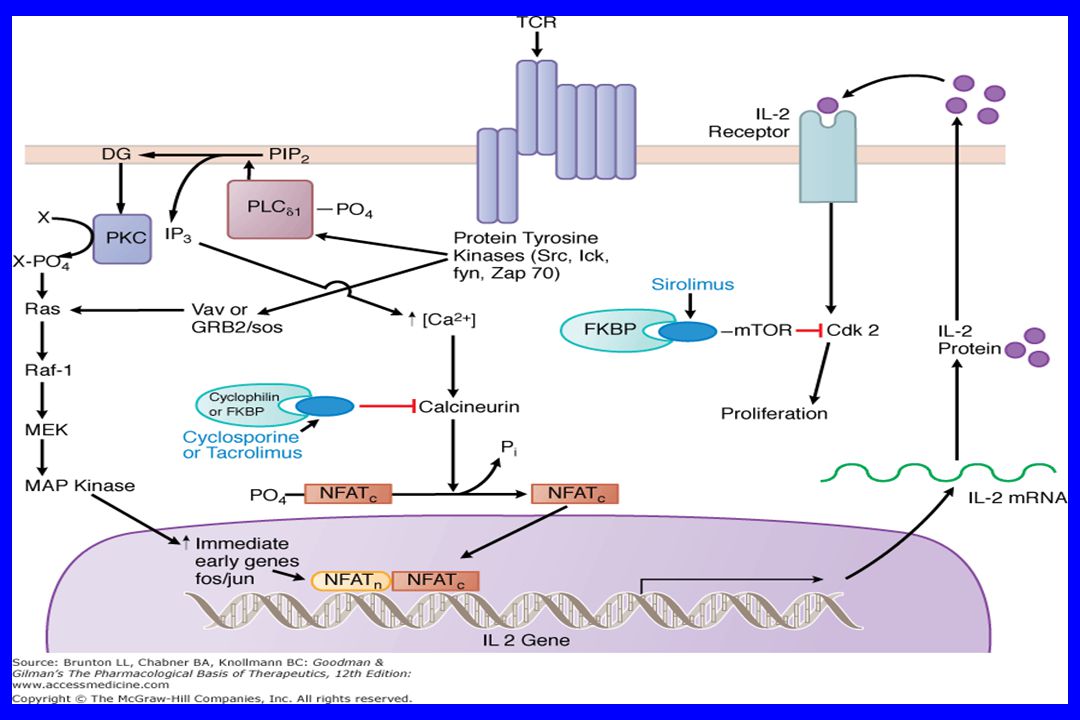



>")













 The adaptive immune system:>")

>")
 Doç.Dr.Hrisi BAHAR.>")
>")
