Download presentation
Presentation is loading. Please wait.

1
OHSS PREVENTION: YES, WE CAN! Shahar Kol, IVF Unit Rambam Health Care Campus, and Faculty of Medicine, Technion, Israel Institute of Technology, February, 2014

2
Faculty Disclosure X No, nothing to disclose Yes, please specify: Off-Label Product Use Will you be presenting or referencing off-label or investigational use of a therapeutic product? No XYes, please specify:The use of GnRH agonists for ovulation triggering in IVF

3
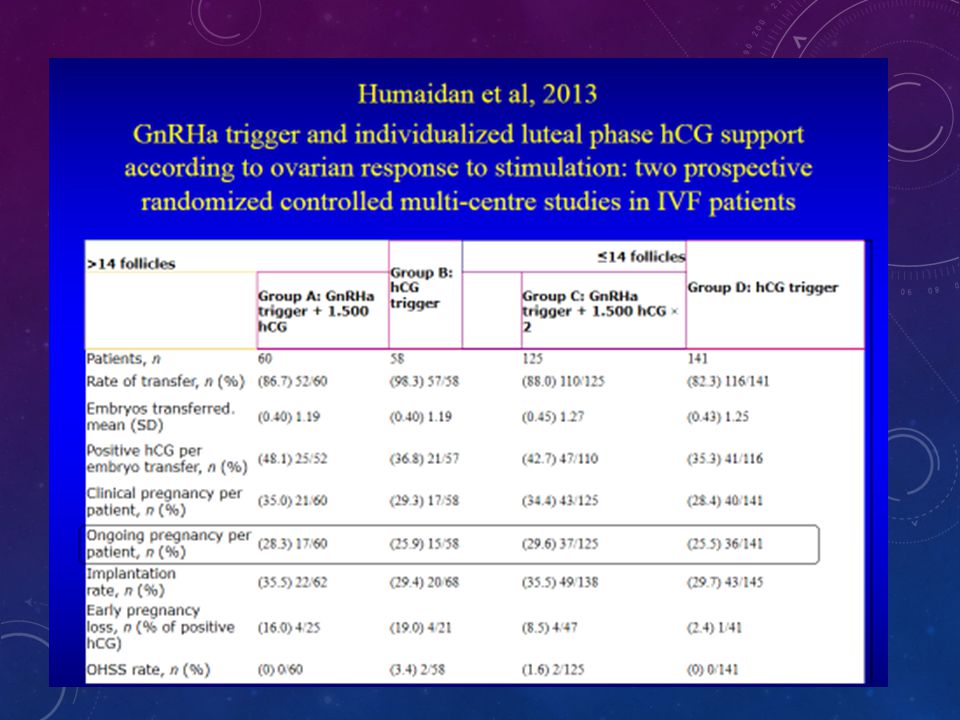
CONTENT OHSS: is it still a problem? No OHSS post agonist trigger! Mechanism? Failures? The question of pregnancy rate. Agonist trigger: back to physiology. Agonist trigger is not the issue, luteal support is. Meta-analysis should follow. A revolution in the making.

4
OHSS: IS IT STILL A PROBLEM? “We did not have a single case in years.”

5
SEVERE OHSS: IS IT STILL A PROBLEM ? “In 2003-2005, 4 deaths (of the 12) were due to OHSS”. ~3 OHSS-related deaths per 100,000 ART cycles.

6
Braat et al, 2010 Three OHSS-related deaths (3:100,000 ART cycles), all had their embryos frozen.
, all had their embryos frozen.")
7
INCIDENCE OF OHSS F&S January 2006 Objective Objective: to determine OHSS incidence in 2,524 antagonist-based cycles (1801 patients). Results Results: fifty three patients (2%) were hospitalized because of OHSS. Conclusions Conclusions: clinically significant OHSS is a limitation even in antagonist cycles. “There is more than ever an urgent need for alternative final oocyte maturation – triggering medication”
 were hospitalized because of OHSS. Conclusions Conclusions: clinically significant OHSS is a limitation even in antagonist cycles. There is more than ever an urgent need for alternative final oocyte maturation – triggering medication .")
8
HOW TO PREVENT OHSS? Agonist trigger is the most effective approach.

9
PRE-ANTAGONIST ERA

10
ANTAGONIST ERA Use of a single bolus of GnRH agonist triptorelin to trigger ovulation after GnRH antagonist ganirelix treatment in women undergoing ovarian stimulation for assisted reproduction, with special reference to the prevention of ovarian hyperstimulation syndrome: preliminary report: Short communication. Itskovitz-Eldor et al. 2000

11
OHSS % (n)n Ovulation trigger Oocyte source Trial typeReference 0 (0/13) 31(4/13) 15 13 GnRHa hCG ownRCT, high risk Babayof et al 2006 0 (0/33) 31 (10/32) 33 32 GnRHa hCG ownRCT, high risk Engamnn et al 2008 0 (0/30) 17 (5/30) 30 GnRHa hCG donorsRCT Acevedo et al 2006 0 (0/1046) 1.3 (13/1031) 1046 1031 GnRHa hCG donorsRetrospective Bodri et al 2009 0 (0/40)40 GnRHa own Observational, High risk Griesinger et al 2010 0 (0/152) 2 (3/150) 152 150 GnRHa hCG ownRCT Humaidan et al 2009 0 (0/23) 4 (1/23) 23 GnRHa hCG own Retrospective, case- controlled, high risk Engmann et al 2006 0 (0/42)42 GnRHa hCG - cancelled own Retrospective case- control, high risk Manzanares et al 2009 0 (0/254) 6 (10/175) 254 175 GnRHa hCG donorsRetrospective Hernandez et al 2009 0 (0/82) 7 (5/69) 82 69 GnRHa hCG own Retrospective, high risk Orvieto et al 2006 0 (0/32) 1 (1/42) 32 42 GnRHa hCG donors Retrospective, high risk: agonist arm only Shapiro et al 2007 0 (0/44) 7 (3/44) 44 GnRHa hCG donorsRCT Sismanoglu et al 2009 8 (1/12)12 GnRH, luteal rescue with hCG 1500IU own Observational, high risk Humaidan et al 2009 0 (0/106) 8 (9/106) 106 GnRHa hCG donorsRCT Galindo et al 2009 0 (0/50) 16(8/50) 50 GnRHa hCG donorsRCT Melo at al 2009 0 (0/45) 15 (33) 45 GnRHa hCG ownRCT, high risk Shahrokh et al 2010 16 publications Agonist: 2,005 patients, not a single case of OHSS! hCG: 92 cases in 1,810 patients, 5.1%

12
WHAT REALLY WORKS: Youssef MA, et al. Human Reprod Update 2010;16:459–466 ● GnRH agonist versus hCG for oocyte triggering in GnRH antagonist ART cycles Total events 0 (GnRH) 21 (hCG)
 21 (hCG).")
13
Lower levels of inhibin A and pro-alpha C during the luteal phase after triggering oocyte maturation with GnRH agonist versus hCG Nevo et al. 2003 Mechanism of OHSS prevention?

14
Luteal phase Nevo et al, 2003 Natural cycle day 7-9= 75 pg/ml vs. 18 Natural cycle day 7-9= 750 pg/ml vs. 184

15
SUMMARY The lower levels of luteal steroidal and nonsteroidal hormones reflect luteolysis, and may explain the mechanism of OHSS prevention by GnRH-a. Pregnancy post agonist trigger does not rescue the CL!!! Nevo et al, 2003

16
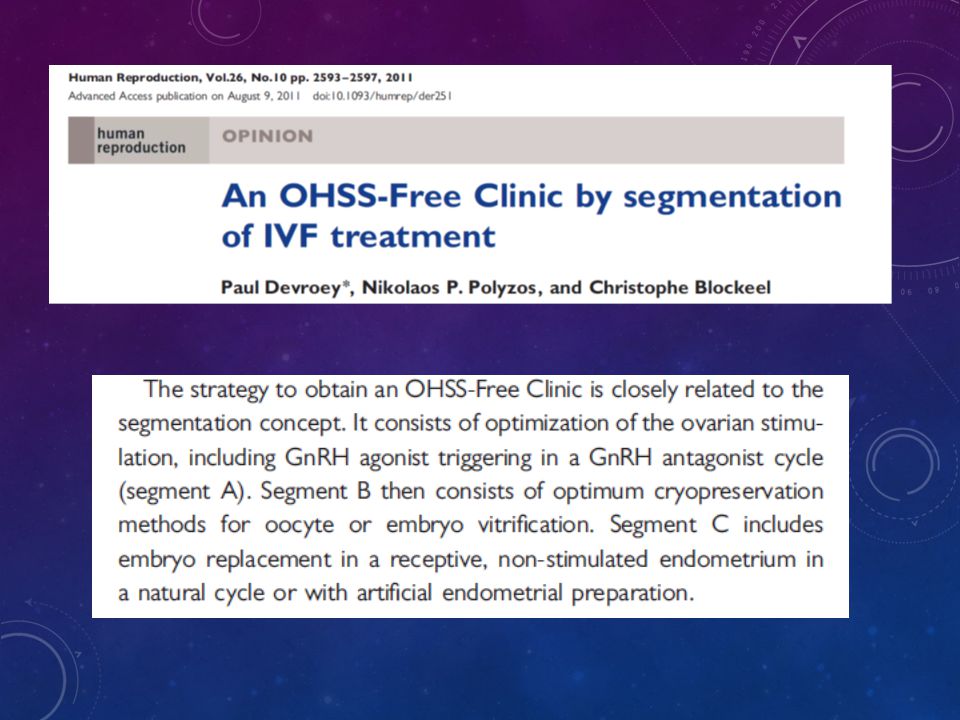
A safe and OHSS-free clinical environment

17
FAILURES? OHSS prevention by GnRH agonist triggering of final oocyte maturation in a GnRH antagonist protocol in combination with freeze-all strategy: a prospective multicenter study Conclusions: “…a single case of a severe early onset OHSS occurred” – E 2 trigger day=47,877 pmol/L – 13 oocytes – The patient was hospitalized on day of OPU, with abdominal distension, drastically enlarged ovaries (right and left ovarian volume 363 cm 2 and 261 cm 2, respectively), and lower abdominal pain. She received low molecular weight heparin, cabergoline (0.5 mg/d), and IV infusion therapy, including albumin. Griesinger G, et al. Fertil Steril 2011;95:2029–2033
, and lower abdominal pain. She received low molecular weight heparin, cabergoline (0.5 mg/d), and IV infusion therapy, including albumin. Griesinger G, et al. Fertil Steril 2011;95:2029–2033.")
18
FAILURES? (CNT’D) – “drastic decrease of hemoglobin levels to 4.9 mmol/L” (8 grams/dL) patient received blood transfusion 2 days post OPU. – Hematocrit: 41 trigger day, 37 OPU day, ‘,<35’ post blood transfusion. – 3–4 days post trigger 3.9 litres of “blood-stained ascites which was indicative of a subacute intraperitoneal hemorrhage”.
 – drastic decrease of hemoglobin levels to 4.9 mmol/L (8 grams/dL) patient received blood transfusion 2 days post OPU. – Hematocrit: 41 trigger day, 37 OPU day, ‘,<35’ post blood transfusion. – 3–4 days post trigger 3.9 litres of blood-stained ascites which was indicative of a subacute intraperitoneal hemorrhage ..")
19
PREGNANCY RATE POST AGONIST TRIGGER We showed that agonist trigger causes quick and irreversible luteolysis. Therefore, the right luteal support is crucial. The evolution of post agonist luteal support.

20
LUTEAL PHASE – NON-SUPPLEMENTED Beckers et al (2003) – very low pregnancy rate.
 – very low pregnancy rate.")
21
LUTEAL PHASE – CONVENTIONAL SUPPORT Not good enough!

22
LUTEAL PHASE – MODIFIED SUPPORT We are getting there!

23
Engmann et al, 2008 LUTEAL PHASE: INTENSIVE E+P OHSS high-risk patients

26
ALL FREEZE ADVANTAGES No OHSS Better endometrium in thaw cycles. Less ectopic pregnancies in thaw cycles. Comparable, or even better, clinical outcome in thaw cycles. Better obstetric outcome? Fresh transfer post agonist trigger requires daily IM injections of progesterone in oil.

27
“… 42% of those who received hCG reported subjective complaints (mostly abdominal discomfort), whereas this percentage was 0% in those who received GnRH agonist to trigger ovulation. Cerrillo et al, 2009 …AND WHEN OHSS IS NOT THE MAIN ISSUE?...

28
HCG DOES NOT IMITATE PHYSIOLOGY! LH surge goes together with FSH surge. Is FSH surge redundant? Gonen et al 1990

29
DUAL ROLE OF HCG TRIGGER Final oocyte maturation. Early luteal phase stimulation. Same dose for both functions? hCG

30
Gonadotropin-releasing hormone agonist versus HCG for oocyte triggering in antagonist assisted reproductive technology cycles. 11/2010 Totally different approaches to luteal support, no common ground for comparison. Agonist triggering is not the issue, individualized luteal support is!

31
Plain language summary: “We recommend that GnRH agonist as a final oocyte maturation trigger should be not used”. 1985: In view of the poor reproductive outcomes following IVF we believe there is no indication for further research with IVF for the treatment of infertile couples…

32
FURTHER RESEARCH Agonist trigger in “empty follicle syndrome” Agonist trigger in “egg factor” infertility Agonist trigger in repeated IVF failure cases. Immature eggs post hCG in face of adequate follicular size on trigger day. hCG-based, P-free luteal support post agonist trigger

33
NON OHSS-HIGH-RISK PATIENTS: SIDE BENEFITS Agonist trigger: more MII oocytes compared with hCG trigger 1-4 Potential benefit of FSH surge: 5-9 Promotes LH receptor formation in luteinizing granulosa cells Promotes nuclear maturation (i.e. resumption of meiosis) Promotes cumulus expansion 1. Humaidan P, et al. Reprod Biomed Online 2005;11:679–684 2. Humaidan P, et al. Human Reprod 2009;24:2389–2394 3. Imoedemhe DA, et al. Fertil Steril 1991;55:328–332 4. Oktay K, et al. Reprod Biomed Online 2010;20:783–788 5. Eppig JJ. Nature 1979;281:483–484 6. Strickland and Beers. J Biol Chem 1976;251:5694–5702 7. Yding Andersen C. Reprod Biomed Online 2002;5:232–239 8. Yding Andersen C, et al. Mol Hum Reprod 1999;5:726–731 9. Zelinski-Wooten MB, et al. Human Reprod 1995;10:1658–1666
 Promotes cumulus expansion 1. Humaidan P, et al. Reprod Biomed Online 2005;11:679– Humaidan P, et al. Human Reprod 2009;24:2389– Imoedemhe DA, et al. Fertil Steril 1991;55:328– Oktay K, et al. Reprod Biomed Online 2010;20:783– Eppig JJ. Nature 1979;281:483– Strickland and Beers. J Biol Chem 1976;251:5694– Yding Andersen C. Reprod Biomed Online 2002;5:232– Yding Andersen C, et al. Mol Hum Reprod 1999;5:726– Zelinski-Wooten MB, et al. Human Reprod 1995;10:1658–1666.")
34
THE ADVANTAGE FOR THE ‘NORMAL RESPONDER’ Kol S, et al. Human Reprod 2011;26:2874–2877 FSH/hMG Antagonist Agonist trigger 36 hours OPU 1500 IU hCG 4 days 1500 IU hCG ET

35
Stimulation characteristics and embryology data Stimulation (days)9.3 ± 2.0 GnRH antagonist (days)3.8 ± 0.9 FSH (units)2443 ± 925 E 2 day of trigger (pmol/L)3764 ± 1227 P day of trigger (nmol/L)2.4 ± 1.65 LH day of trigger (IU/L)1.9 ± 1.3 Oocytes retrieved6.7 ± 2.5 Embryos obtained3.6 ± 1.7 Embryos transferred2.9 ± 0.9 Embryos frozen0.8 ± 1.5 Beta hCG (IU/L)152 ± 86 E 2 (day of pregnancy test, pmol/L)6607 ± 3789 P (day of pregnancy test, nmol/L)182 ± 50 Values are mean ± SD Reproductive outcomes Positive hCG/cycle, n (%)11/15 (73) Clinical ongoing pregnancy, n (%)7/15 (47) Early pregnancy loss, n (%)4/11 (36) Kol S, et al. Human Reprod 2011;26:2874–2877

36
WHAT DO PRACTITIONERS SAY? Among the five most downloaded papers

37
SURVEY RESULTS: Triggering of ovulation with GnRH-a in ART: Worldwide feedback on an emerging new option with great potential TAKE HOME MESSAGE “The results of this survey indicate that GnRH trigger is widely used worldwide and therefore has become part of the standard of care today. Hence, doctors are entitled to prescribe it just as patients may ask that this option is considered in their case.”

38
“Agonist triggering is viewed as one of the major advances in ovarian stimulation, with the potential to eliminate OHSS…”

39
OutIn “long agonist” protocolsAntagonist-based protocols hCG triggerAgonist trigger Progesterone-based luteal supportLH activity-based luteal support ~1% severe OHSSTotal OHSS elimination Painful P injections or leaky, messy vaginal P. Patient friendly luteal phase Revolution in the making

40
Thank you

Similar presentations









 Is It Safe? Mustafa Uğur Zekai Tahir Burak Women’s Health Education and Research Hospital, Ankara, Turkey.>")





 Director, IVF Center, HKSH Specialist.>")



