Download presentation
Presentation is loading. Please wait.

1
Ocular Motility II Kenn Freedman M.D.

2
Supranuclear Cranial Nerves Extra-ocular Muscles

3
Older woman with diabetes suffered sudden onset of Right IIIrd nerve palsy, left elevation defect and left sided weakness

4
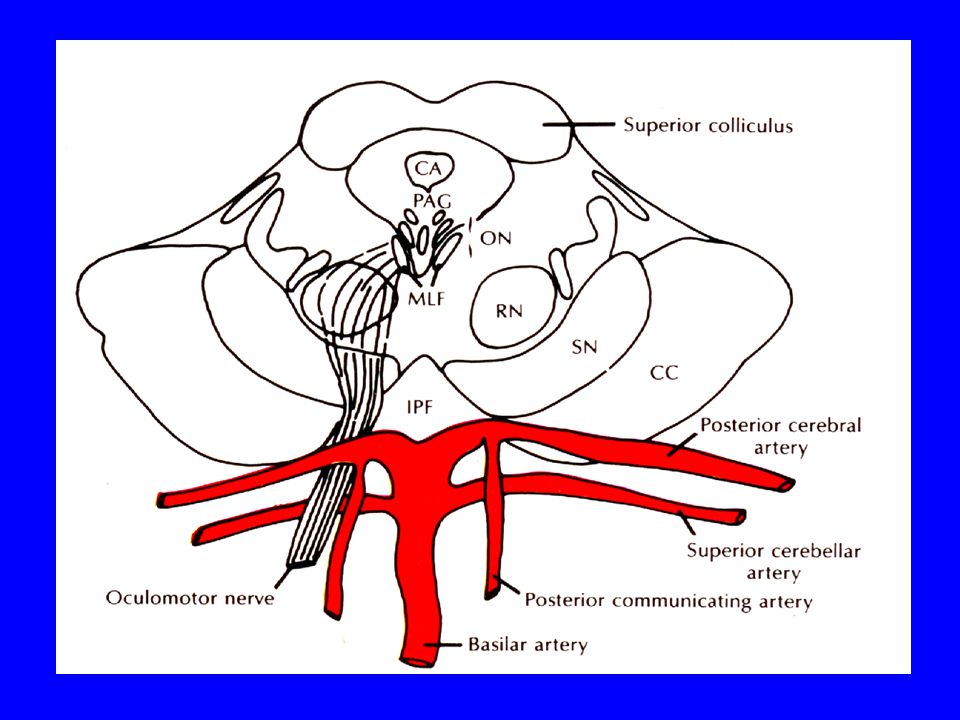
Oculomotor Nerve Complex Nucleus in Midbrain Exits interpeduncular space passing several vessels including PCA Cavernous sinus Superior Orbital Fissure Superior and Inferior Divisions Superior: Levator and SR Inferior: MR, IR, IO

6
Left IIIrd Nerve palsy

7
Third Nerve Palsy Aneurysm Microvascular – DM, HTN, heart disease Trauma Neoplasm Syphilis Other, Undetermined

8
Third Nerve Palsy

9
Third nerve palsy Microvascular

10
Young woman presented with left sided headache and drooping of her eyelid

11
Patient could not move her eye up, down or toward her nose, but she could abduct. Her pupil on the left was much larger than the right.

12
PCA Aneurysm

13
Bilateral Ptosis with poor movement except abduction

14
Nuclear IIIrd nerve palsy

15
Brainstem Syndromes Weber’s - ipsalateral pupil involved IIIrd - contalateral hemiplegia - fasicle of IIIrd Nerve where traverses cerebral peduncle Benedikt’s – ipsalateral pupil involved IIIrd - contralateral limb intention tremor, hypokinesia and ataxia - Fasicle of IIIrd nerve as it traverses the red nucleus

16
Management of Third Nerve Palsy When to do neuro-imaging and/or arteriogram? Important factors: PAIN, PUPIL, PROGRESSION Other Possible testing: CBC, ESR, BS

17
In general You get imaging on PUPIL INVOLVED Third nerve palsies

18
Relative Pupil Sparing 0.5mm <Anisocoria < 2mm (Larger pupil still RTL) Out of 24 patients: 10 - had compressive lesions! 10 - “infarction” 4 - other Neurology 2001; 56: 797

19
Imaging Options MRI MRA – no contrast Cerebral Arteriogram – some risk

20
Management Isolated Third Nerve Palsy If patient is diabetic/ hypertensive and the pupil is not involved and they do not have too much pain*, then it would be reasonable to follow them up without imaging studies, depending on your comfort level. You should see some resolution of a microvascular palsy in at least two months.

21
Aberrant Regeneration One of many possible findings due to misdirection of axon fibers as healing occurs 1.Lid retraction on downgaze 2.Lid elevation or pupil constriction with attempted adduction 3.Globe retraction with attempted upgaze or downgaze 4.Others also possible

22
Aberrant Regeneration

23
Lid Lag on Downgaze Congenital Ptosis -Levator Maldevelopment Graves Ophthalmopathy Surgery, Trauma Aberrant Regeneration of 3 rd -pseudo von Graefe’s phenomenum

24
Primary Aberrant Regeneration? Motility problems like those described above without an acute third nerve palsy preceding them. Suggestive of a cavernous sinus mass

25
Trochlear Nerve Superior Oblique Long course of nerve from posterior midbrain to orbit Midbrain

26
Fourth Nerve Palsy Note head tilt

27
4 th Nerve Palsy Diplopia –usually vertical Sometimes Cyclo-diplopia Head tilt and/or turn Diplopia can worse or better on downgaze Findings can evolve over time

28
Fourth Nerve Palsy Hypertropia Overaction of Ipsalateral Inferior Oblique Muscle Underaction of SO not often obvious Excyclotorsion Incommitant

29
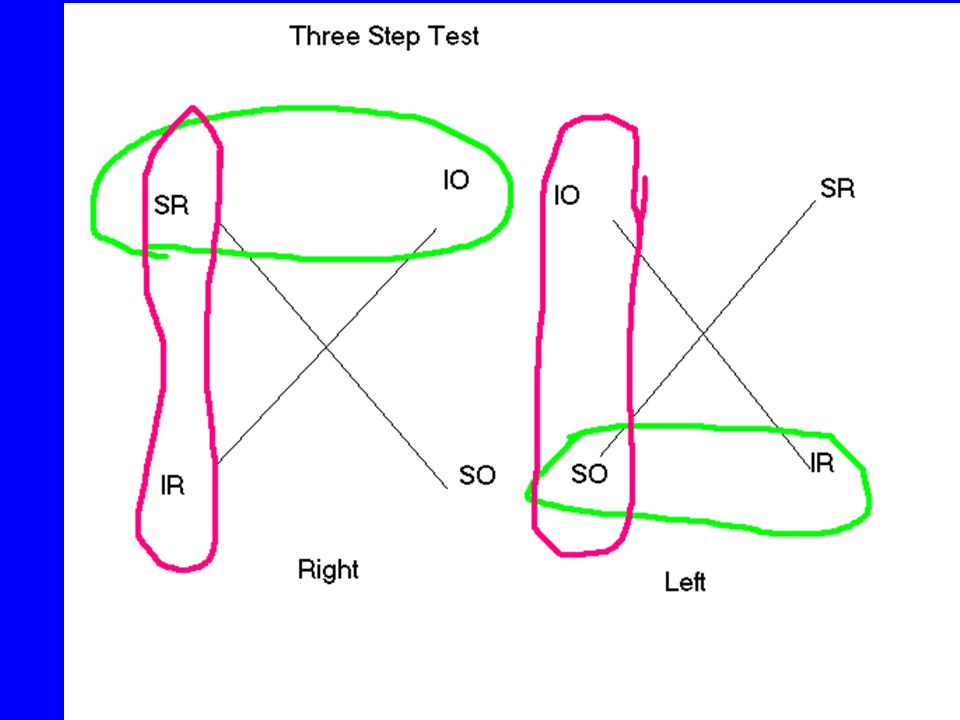
Fourth Cranial Nerve Palsy Incommitance Hypertropia Hypertropia worse on contraleral gaze Hypertropia worse on ipsalateral head tilt E.g. “ right – left - right” or “left - right – left”

30
Right- Left- Right 2 RHT 7 RHT 18 RHT 15 RHT 3 RHT

31
Three Step Test is only valid for Neurologic and not mechanical muscle problems Assumes only one paretic muscle

34
Think in terms of a paretic muscle

40
DX: Left SO palsy

41
Excylotorsion With red maddox rod over Right and white over Left Shows a right excylcotorsion consistent with a right SO palsy

42
Fourth Nerve Palsy Congenital* Traumatic Microvascular Neoplasm Aneurysm – not common Other * Congenital – often decompensate later in life with “sudden” onset of diplopia, will have large vertical fusional amplitudes

43
Fourth Nerve Palsy (Traumatic) Upshoot in adduction characteristic of Overaction of left inferior oblique
 Upshoot in adduction characteristic of Overaction of left inferior oblique")
44
Upshoot in Adduction Most Commonly IOOA DVD Duane’s Syndrome

45
Right Fourth Nerve Palsy

46
Bilateral Fourth Nerve Palsy Alternating Hypertropia e.g. LHT in right gaze RHT in left gaze Large Excyclotorsion >10-15 degrees V pattern

47
Vertical Misalignment Fourth Nerve Palsy Graves Disease Post-operative muscle problem Skew Deviation Third Nerve Palsy – inferior or superior division Brown’s Syndrome Other Orbital Disease Plus More

48
Management of Isolated Fourth Nerve Palsy Usually no work up necessary as most cases are traumatic or congenital. If no history of trauma or signs of congenital palsy then : Does patient have vasculopathic risk factors? Yes: Observe No: Medical evaluation, maybe image

49
Abduction Deficit New onset diplopia Patient asked to look To the left

50
Abduction Deficit Sixth Cranial Nerve Palsy Graves Ophthalmopathy Myasthenia Gravis Orbital – tumor, inflammatory Duane’s Syndrome Type I Medial Wall Fracture Past LR recession More!

51
What’s this abduction deficit due to?

52
Patient had R+R OS for Exotropia, why does she have decreased abduction?

53
Agenesis of sixth nerve nucleus and, with abberent innervation of the Lateral Rectus muscle by branches third cranial nerve, hence multiple motility problems can be seen Duane’s Type I Type II Type III Duane’s Syndrome

54
For Example Duane’s Type I loss of abduction, often esotropic (no diplopia) variable loss of adduction narrowing of fissure on attempted abduction upshoot or downshoot in attempted adduction possible
 variable loss of adduction narrowing of fissure on attempted abduction upshoot or downshoot in attempted adduction possible")
55
Sixth Nerve Palsy Microvascular Neoplastic (Posterior Fossa, Orbit, Cavernous sinus, etc) Trauma Increased Intracranial Pressure Aneurysm Post-viral and post-immunization Other – MS, Syphilis, PML Undetermined
 Trauma Increased Intracranial Pressure Aneurysm Post-viral and post-immunization Other – MS, Syphilis, PML Undetermined")
56
Sixth Nerve Palsies in Children*: 1. Tumors 45% 2. Increased ICP (15%) non-tumor 3. Traumatic 12% 4. Congenital 11% 5. Inflammatory 7% 6. Miscellaneous 5% ( post-immunization, post-viral) 7. Idiopathic 5% * JPOS; 1999; 36: 305
 non-tumor 3. Traumatic 12% 4. Congenital 11% 5. Inflammatory 7% 6. Miscellaneous 5% ( post-immunization, post-viral) 7. Idiopathic 5% * JPOS; 1999; 36: 305.")
57
Brainstem Syndromes with Sixth Cranial Nerve Palsy Foville’s Syndrome* - - lesion in region of sixth nerve nucleus - ipsalateral gaze palsy, facial palsy, loss of taste, Horner’s Syndrome, facial anesthesia, deafness Millard-Gubler Syndrome – Sixth and contralateral hemiparesis

58
Primary Closing Lids Looking Left What’s Wrong? Where is at least one lesion? Pontine CVA?

59
Pontine CVA

60
Insert MRI scan of Eutenaurer

61
Total Ophthalmoplegia, loss of vision and ptosis OD Cavernous sinus tumor probable meningioma

62
Multiple Cranial Nerve Palsies (3,4,6, etc) Superior Orbital Fissure Syndrome Suspect Orbital Inflammatory Process –pseudotumor, and cellulitis (think fungal) Cavernous SinusThrombosis Orbital or Cavernous sinus tumor Vascular: AV fistulas or aneurysms Invasive Periorbital Skin Cancers with perinerual spread GCA Diabetic Other: HZO, Mucocele, Wernicke’s encephalopathy, Guillain-Barre or Miller Fisher Syndromes
 Superior Orbital Fissure Syndrome Suspect Orbital Inflammatory Process –pseudotumor, and cellulitis (think fungal) Cavernous SinusThrombosis Orbital or Cavernous sinus tumor Vascular: AV fistulas or aneurysms Invasive Periorbital Skin Cancers with perinerual spread GCA Diabetic Other: HZO, Mucocele, Wernicke’s encephalopathy, Guillain-Barre or Miller Fisher Syndromes")
63
Cranial Nerve Palsy History DM, HTN, CV disease Neurologic disease Shunting procedures Pain Age

64
Cranial Nerve Palsy Exam Standard Eye Exam, but also include: Exophthalmetry Checking other cranial nerve function (5,7,8) – COMPANY THEY KEEP
 – COMPANY THEY KEEP")
65
Cranial Nerve Palsy Major Considerations Microvascular Trauma Neoplastic Aneurysm Congenital Other: GCA, Sarcoid Consider: MS and Myasthenia

66
General Approach to CN Palsies Other Localizing signs Pupils Pain Progression FOLLOW-UP, microvascular palsies resolve usually in about 2 months

67
Matching Millard-Gubler Weber’s Miller Fisher Duanes Benedikt’s III IV VI Multiple CN

Similar presentations









 in Drake et al.>")
















