Download presentation
Presentation is loading. Please wait.

1
Buffer Solutions May Compromise Cardiac Resuscitation by Reducing Coronary Perfusion Pressure JAMA. 1991;226:2121-2126 Kette, Weil, Gazmuri Chicago, IL Objective: to investigate effects of hypertonic buffer solutions on coronary perfusion pressure and resuscibility during experimental closed-chest cardiac resuscitation Design: Randomized, placebo controlled Setting:Mammailian research lab, 44 domestic pigs

2
Buffer Solutions May Compromise Cardiac Resuscitation by Reducing Coronary Perfusion Pressure Interventions: Cardiac arrest was induced by ventricular fibrillation in mechanically ventilated pigs anesthetized with pentobarbital sodium. Precordial compression was started at third minute of untreated VF and maintained for an interval of 8 minutes. A hypertonic solution of sodium bicarbonate, Carbicarb, or sodium chloride or an isotonic solution of sodium chloride was infused into the right atrium over a 1-minute interval starting at the sixth minute of VF. Restoration of spontaneous circulation was attempted by DC transthoracic countershock after 11 minutes of VF Main Outcomes Measures: Plasma osmolality, CPP and cardiac resuscibility

3
Results: Infusion of hypertonic buffer and sodium chloride solutions increased plasma osmolality from an average of 280 to 330 mOsm/kg. This was accompanied by a significant decrease in the aortic pressures and CPPs generated during precordial compression. No such changes occurred after infusion of isotonic sodium chloride. Restoration of spontaneous circulation, as in earlier studies, was contigent on the levels of CPP proir to attempted defibrillation. Accordingly, none of the 13 animals in which CPP declined to less than 10 mm Hg after infusion of hypertonic solutions were successfully resuscitated. This contrasted with nine animals that received isotonic sodium chloride and served as controls. Coronary perfusion pressure consistently exceeded 10 mm Hg in these control animals, and spontaneous circulation was restored in each instance.

4
Buffer Solutions May Compromise Cardiac Resuscitation by Reducing Coronary Perfusion Pressure Conclusion: Hypertonic solutions and specifically buffer solutions administered in the absence of vasopressor agents may adversely affect cardiac resuscitation efforts by reducing CPP below critical thresholds.

7
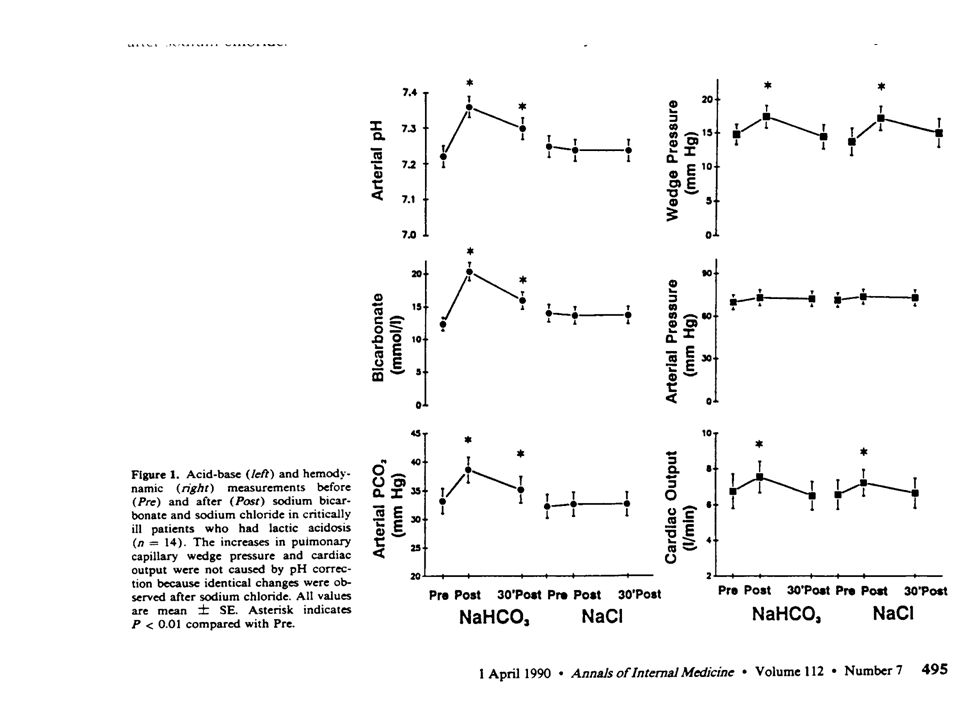
Bicarbonate Does Not Improve Hemodynamics in Critically Ill Patients Who Have Lactic Acidosis Annals of Internal Medicine. 1990;112:492-498. Cooper,Walley British Columbia, Canada Objective: To determine whether correction of acidemia using bicarbonate improves hemodynamics in patients who have lactic acidosis Design: Prospective, randomized, crossover, blinded Setting: ICU tertiary hospital Patients: 14 with metabolic acidosis, all with PA catheters, 13 on catecholamines

8
Bicarbonate Does Not Improve Hemodynamics in Critically Ill Patients Who Have Lactic Acidosis Measurements and Main Results: – Sodium bicarbonate increased arterial pH, HCO 3 -, PaCO 2 and decreased plasma ionized calcium. –NaHCO 3 and NaCl both transiently increased PCWP and CO. –MAP was unchanged. –Hemodynamic responses to NaCO 3 and NaCl were the same

9
Bicarbonate Does Not Improve Hemodynamics in Critically Ill Patients Who Have Lactic Acidosis Conclusions: Correction of acidemia using sodium bicarbonate does not improve hemodynamics in critically ill patients who have metabolic acidosis and increased blood lactate or the cardiovascular response to infused catecholamines in these patients. Sodium bicarbonate decreases plasma ionized calcium and increases P a CO2.

13
Effects of Bicarbonate Therapy on hemodynamics and tissue oxygenation in patients with lactic acidosis Critical Care Medicine 1991;19:1352-1356 Mathieu, Neviere Lille, France Objective: To determine whether correction of acidemia using bicarbonate improves hemodynamics variables and tissue oxygenation in patients with lactic acidosis Design: Prospective, randomized, blinded, cross- over Patients: 10 with metabolic acidosis, increased lactate, no severe renal failure

14
Effects of Bicarbonate Therapy on hemodynamics and tissue oxygenation in patients with lactic acidosis Method: NaHCO 3 (1 mmol/kg) or equal volume of NaCl was injected IV at the beginning of two successive 1-hr study periods. Arterial and venous blood gas measurements, plasma electrolytes, osmolality, lactate, 2,3-DPG, oxygen hemoglobin affinity, hemodynamics, oxygen delivery and oxygen consumption measurements were obtained before and repeatedly during the study period after injection of NaHCO 3 and NaCl.

15
Effects of Bicarbonate Therapy on hemodynamics and tissue oxygenation in patients with lactic acidosis Measurements and Main Results: –NaHCO3 increased arterial and venous pH, serum bicarbonate, PaCO 2, PvCO 2 –Hemodynamic responses were similar –Tissue oxygenation was not modified –No changes in serum Na, osmolality, arterial and venous lactate, red cell 2,3-DPG, hemoglobin affinity for O 2 observed

16
Effects of Bicarbonate Therapy on hemodynamics and Tissue Oxygenation in Patients With Lactic Acidosis Conclusion: Administration of sodium bicarbonate did not improve hemodynamic variables in patients with lactic acidosis, but did not worsen tissue oxygenation.

Similar presentations






















 concentration. More H + = more acidic = lower.>")
