Download presentation
Presentation is loading. Please wait.

1
VAGINAL BLEEDING Dr. Paul Chang March 31, 2015

2
OUTLINE Normal menstrual cycle Definitions Approach Pre-Menopausal AUB
Post-Menopausal AUB Early Pregnancy Related bleeding (First trimester)
")
3
Differentials that I will not cover
Trauma Bowel Neonatal, Pediatric causes Antepartum causes

4
Abnormal Uterine Bleeding
In the absence of pregnancy… Affects 11-13% of reproductive age women(up to 30% according to SOGC) 24% in women aged 36-40 Women generally present for care because the amount, timing, or other characteristics of the bleeding have changed from their individual norm
 24% in women aged Women generally present for care because the amount, timing, or other characteristics of the bleeding have changed from their individual norm.")
5
Regulation of Menstrual Bleeding
In the endometrial lining, rising levels of estradiol produced by the follicles stimulate proliferative growth of epithelial and stromal elements. The endometrium thickens and becomes rich in progesterone receptors. Once the LH surges, the ovum is released, and the follicle collapses to become the corpus luteum. The corpus luteum lasts for approximately 10 days and produces large amounts of progesterone. Under the progestagenic influence, the endometrium enters the secretory phase. Endometrial growth stops, and the stroma becomes more compact and stable.

6
Regulation of Menstrual Bleeding
If the egg is not fertilized, the corpus luteum degenerates and no longer produces progesterone, the estrogen level decreases, the top layers of the lining break down and are shed, and menstrual bleeding occurs

7
Normal Dimensions of Menses
Frequency of menses Every days Regularity of menses from cycle-to-cycle +/- 2 to 20 days Heaviness of flow 5-80mL per month (avg 35mL) Duration of flow 4-8 days
 Duration of flow. 4-8 days.")
8
Definitions Menorrhagia: menstrual periods with abnormally heavy or prolonged bleeding (>80mL per month) Oligomenorrhea: cycle length > 35 days Polymenorrhea: cyclic length > 24 days Metrorrhagia: irregular intervals with normal or reduced volume and duration of flow Menometrorrhagia: irregular intervals with excessive volume and duration of flow Postmenopausal bleeding: bleeding that occurs more than 12 months after the last menstrual cycle

9
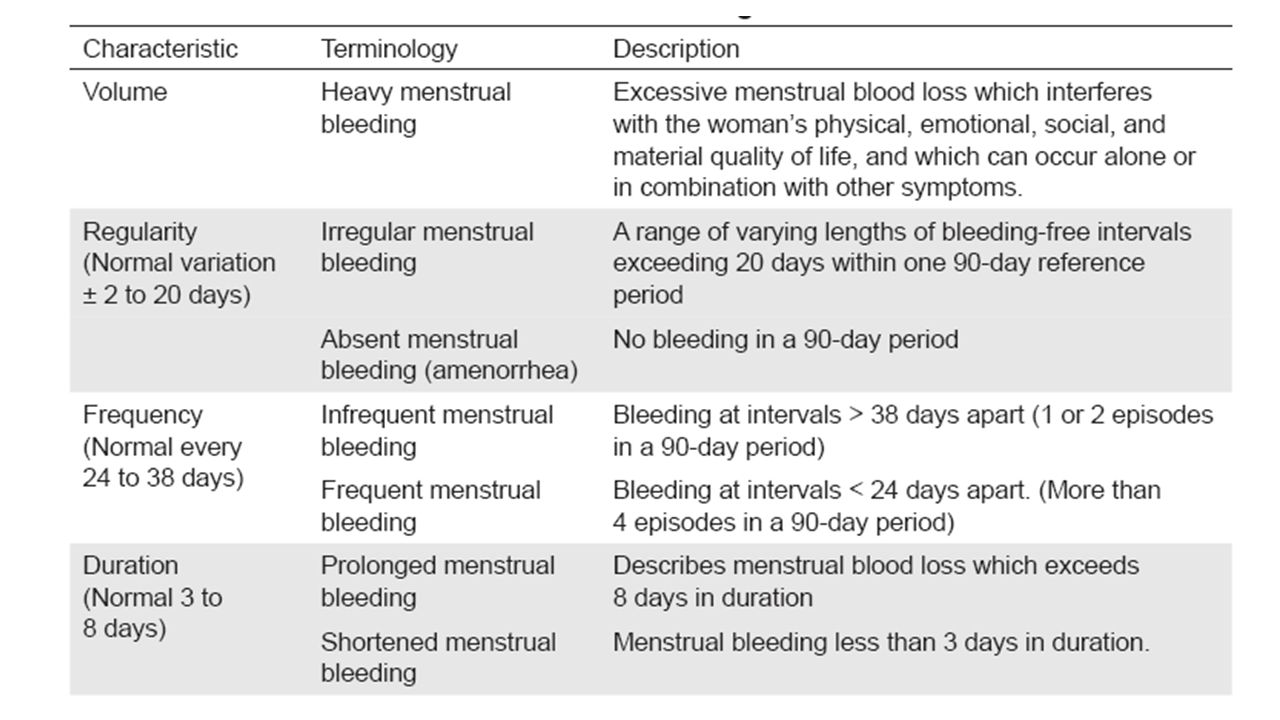
FIGO Menstrual Disorders Working Group 2012
Suggested new nomenclature for Abnormal Uterine Bleeding (AUB) Goal: Simplify Eliminate terminology such as menorrhagia, metrorrhaiga, and dysfunction uterine bleeding Terminology for AUB Volume Regularity Frequency Duration Other International Federation of Gynecology and Obstetrics
 Goal: Simplify. Eliminate terminology such as menorrhagia, metrorrhaiga, and dysfunction uterine bleeding. Terminology for AUB. Volume. Regularity. Frequency. Duration. Other. International Federation of Gynecology and Obstetrics.")
13
PALM side refers to structural causes that could be evaluated and diagnosed on imaging and/or biopsy. The COEIN side allows consideration of underlying medical disturbances

14
Menstrual History Age of menarche Volume Regularity Frequency Duration
Associated symptoms: Pain, Mittelschmerz, premenstrual symptoms

15
Bleeding History Timing in relationship to menses Other Locations:
Onset Quantity Pictorial blood assessment chart Severity How many pads? Runs down legs? Interfering with school, work? Symptomatic Black outs SOB Palpitations Timing in relationship to menses Other Locations: Teeth Bruising Hemorrhage/transfusion hx Associated symptoms: vaginal discharge or odour pelvic pain or pressure

17
Approach

18
History Menstrual History Bleeding History OB History Family History
Inherited coagulation disorders PCOS Endometrial or colon cancers Meds including herbs Anticoagulants Antidepressants (SSRIs and tricyclics) Hormonal contraceptives Tamoxifen Antipsychotics (first generation and risperidone) Corticosteroids Herbs: gensing, chasteberry, danshen
 Hormonal contraceptives. Tamoxifen. Antipsychotics (first generation and risperidone) Corticosteroids. Herbs: gensing, chasteberry, danshen.")
19
Physical Exam Vitals, weight, BMI Signs of anemia
Conjunctivae Hb 95 Hand Crease Hb 75 Ocular Bruits Hb 55 Signs of bleeding disorder Petechiae, Ecchymoses, swollen joints Thyroid exam Gyn exam (bimanual and speculum)
")
20
Investigations CBC bHCG Ferritin INR, PTT TSH Blood group and type
vWF screen when indicated (factor VIII, vWF antigen, vWF functional assay) Pap smear and cervical cultures when indicated Pelvic ultrasound/ saline infusion ultrasound Endometrial biopsy D&C Hysteroscopy
 Pap smear and cervical cultures when indicated. Pelvic ultrasound/ saline infusion ultrasound. Endometrial biopsy. D&C. Hysteroscopy.")
21
Saline Infusion Ultrasound
Sonohysterogram Hysterosonogram

22
Saline Infusion Ultrasound

23
Acute Management ABCs Vitals Estimate stage of shock
IV, foley, pulse oximeter, O2 Bolus 1-2L of RL or NS Ultrasound Group and type & bHCG Call for help If pregnant, remember to assess the gestation (FHR), Rhogam if appropriate
, Rhogam if appropriate.")
24
DDx By Age 13-18 Hypothalamic-Pituitary-Ovarian access immature
Hormonal contraceptives Pregnancy Pelvic infection Coagulopathies

25
DDx By Age 19-39 Pregnancy Polyp Leiomyoma Anovulation (PCOS)
Hormonal contraceptives Endometrial hyperplasia/cancer

26
DDx By Age 40 and over Anovulatory bleeding Endometrial Hyperplasia
Endometrial Cancer Vaginal atrophy Use of anti-coagulants Rarely leiomyoma

27
Medical Therapies NSAIDs Antifibrinolytics (Tranexamic Acid)
Combined Hormonal Contraceptives Cyclical progestins for anovulatory bleeding Continous high dose progestins Depo medroxyprogesterone acetate Levonorgestrel IUD GnRHa

28
High Yield Diagnosis & Its Management

29
Endometrial Polyps Overgrowth of cells in the lining of the uterus (endometrium) leads to the formation of uterine polyps, also known as endometrial polyps Menstrual characteristic: Intermenstrual spotting Hysteroscopic resection
 leads to the formation of uterine polyps, also known as endometrial polyps. Menstrual characteristic: Intermenstrual spotting. Hysteroscopic resection.")
30
Adenomyosis Hormonal contraceptives NSAIDs Dienogest (Visanne©)
Endometrial tissue, which normally lines the uterus, exists within and grows into the muscular wall of the uterus Often asymptomatic Menstrual characteristic: Heavy, prolonged periods Dysmenorrhea Dyspareunia Inter-menstrual bleeding O/E: Enlarged uterus Hormonal contraceptives NSAIDs Dienogest (Visanne©) Mirena© GnRHa Hysterectomy
 Mirena© GnRHa. Hysterectomy.")
31
Adenomyosis

32
Fibroids Monoclonal non-cancerous growth of the myometrium
As many as 3 out of 4 women have uterine fibroids sometime during their lives Often asymptomatic Menstrual characteristic: Heavy prolonged periods U/S: bulky uterus Hormonal contraceptives (*personally do not recommend) NSAIDs Tranexamic acid SPRMs (Fibristil©) Mirena© GnRHa Myomectomy Uterine artery embolization mrHIFU Hysterectomy
 NSAIDs. Tranexamic acid. SPRMs (Fibristil©) Mirena© GnRHa. Myomectomy. Uterine artery embolization. mrHIFU. Hysterectomy.")
33
Fibroids

34
Fibristil© Ulipristal acetate
Selective Progesterone Receptor Modulator

35
Von Willebrand Disease
Most cases are autosomal dominant inherited disorders. Most severe form is autosomal recessive. May be acquired Most common inherited bleeding disorder The prevalence of vWD is about 1 in 100 individuals. However the majority of these people do not have symptoms. The prevalence of clinically significant cases is 1 per 10,000 Menstrual characteristic: Heavy volume is more prevalent (57-93% vs. 10% in normal controls) Special tests: vWF screen (factor VIII, vWF antigen, cWF functional assay) Medical Management: OCP Depo-Provera Mirena GnRHa Tranexamic Acid DDAVP* Replacement therapy (Humate-P, platelets, cryoppte, FFP) Surgical Management: Endometrial Ablation Contraindications: NSAIDs
 Special tests: vWF screen (factor VIII, vWF antigen, cWF functional assay) Medical Management: OCP. Depo-Provera. Mirena. GnRHa. Tranexamic Acid. DDAVP* Replacement therapy (Humate-P, platelets, cryoppte, FFP) Surgical Management: Endometrial Ablation. Contraindications: NSAIDs.")
36
Anovulatory Most common: PCOS Hypothalamic hypogonadism
Premature ovarian failure Menstrual characteristic: Irregular with variable frequency and duration Hormonal contraceptives Cyclical progestins

37
Iatrogenic: Breakthrough Bleeding
Non-menstrual bleeding while on hormonal contraceptives The low dose of oestrogen in modern contraceptive pills is insufficient to maintain endometrial integrity and the opposing effect of progestogen promotes atrophy of glands and stroma. The resulting endometrium is thin, fragile and prone to bleeding Menstrual characteristic: Light and intermenstrual Reassurance: continue CHC for up to 3 months Change to a more estrogenic CHC Consider vaginal ring Refer to Dr. Nayot’s talk

38
Endometrial NSAIDs Hormonal contraceptives Progestins Mirena©
AUB can occur in women with normal ovulatory function, and without coagulopathies because of abnormalities that reside in the endometrium: Abnormal prostaglandin synthesis Prostaglandin receptor upregulation Increased fibrinolytic activity Increased tissue plasminogen activity NSAIDs Hormonal contraceptives Progestins Mirena© Tranexamic acid SPRMs (Fibristil©) GnRHa Endometrial ablation Hysterectomy
 GnRHa. Endometrial ablation. Hysterectomy.")
39
Early Pregnancy Remember to give Rhogam if mom is Rh-ve (unless certain that of paternity and that he is also Rh-ve) <12 wk GA, 120mcg IM 12 wks and higher, 300mcg IM DO NOT FORGET: Follow bHCG to zero if non-viable

40
Abortion Expectant Misoprostol D&C

41
Ectopic Send to hospital MTX Laparoscopic surgery

42
Molar Pregnancy Suction D&C Oxytocin during curettage MTX
In a complete molar pregnancy, all of the fertilized egg's chromosomes come from the father. Shortly after fertilization, the chromosomes from the mother's egg are lost or inactivated and the father's chromosomes are duplicated. The egg may have had an inactive nucleus or no nucleus. In a partial or incomplete molar pregnancy, the mother's chromosomes remain but the father provides two sets of chromosomes. As a result, the embryo has 69 chromosomes instead of 46. This can happen when the father's chromosomes are duplicated or if two sperm fertilize a single egg.

43
Endometrial Hyperplasia
Risk factors: Nulliparity Late menopause Obesity Smoking Anovulation (PCOS) Unopposed estrogen Tamoxifen Endometrial biopsy or D&C Pelvic ultrasound (≤4mm is low risk) Hysteroscopy
 Unopposed estrogen. Tamoxifen. Endometrial biopsy or D&C. Pelvic ultrasound (≤4mm is low risk) Hysteroscopy.")
44
Endometrial Hyperplasia
WHO Progression to Cancer Simple Hyperplasia 1% Complex Hyperplasia 3% Atypical Simplex Hyperplasia 8% Atypical Complex Hyperplasia 29% Medical Management Progesterone therapy Provera 10mg 14 days per month (x 3 months) Megace Mirena Clomid (SERM) Surgical Management: Hysterectomy
 Megace. Mirena. Clomid (SERM) Surgical Management: Hysterectomy.")
45
Endometrial cancer Most common gynecologic cancer in North America
Avg age for endometrial ca is 61 5-30% of cases occur in premenopause HPNCC have a lifetime risk for endometrial ca of 40-60% Refer to Gynecologic Oncologist

46
Summary Rule out pregnancy PALM COEIN (I = iatrogenic and infectious)
History (menstrual, bleeding) Physical Investigations Acute management On-going therapies Refer if appropriate Read the question. Breathe. You can do it!
 Physical. Investigations. Acute management. On-going therapies. Refer if appropriate. Read the question. Breathe. You can do it!")
47
Thank You

Similar presentations


















 2014.>")


.>")
