Download presentation
Presentation is loading. Please wait.

1
Seminar Difficult Airway: Assessment and Management Algorithms
Presenter : Anil Agarwal Date : March 19, 2007

2
Difficult Airway: Definitions
A clinical situation in which a conventionally trained anaesthesiologist experiences difficulty with mask ventilation, difficulty with tracheal intubation or both Difficult airway: spectrum Difficult : spontaneous/mask ventilation laryngoscopy tracheal intubation Ref. Anesthesiology, May 2003

3
Definitions (Contd.) Difficult mask ventilation: A clinical situation when either, It is not possible for unassisted anaesthesiologist to maintain the SpO2 > 90% using 100% O2 and positive pressure mask ventilation in a patient whose SpO2 was > 90% before the anaesthetic intervention or It is not possible for the unassisted anaesthesiologist to prevent or reverse signs of inadequate ventilation during mask ventilation

4
Definitions (Contd.) Difficult laryngoscopy
It is not possibe to see any portion of the vocal cords after multiple attempts at conventional laryngoscopy (3, ASA) Difficult tracheal intubation A clinical situation in which intubation requires more than three attempts or ten minutes using conventional laryngoscopic techniques
 Difficult tracheal intubation. A clinical situation in which intubation requires more than three attempts or ten minutes using conventional laryngoscopic techniques.")
5
Definitions (Contd.) Optimal attempt at laryngoscopy – can be defined as Performance by a reasonably experienced laryngoscopist The use of the optimal sniffing position The use of OELM One change in length/type of blade

8
Assessment of Difficult Airway
History General physical examination Specific tests for assessment Difficult mask ventilation Difficult laryngoscopy Difficult surgical airway access Radiologic assessment

9
History Congenital airway difficulties: e.g. Pierre Robin, Klippel-Feil, Down’s syndromes Acquired Rheumatoid arthritis, Acromegaly, Benign and malignant tumors of tongue, larynx etc. Iatrogenic Oral/pharyngeal radiotherapy, Laryngeal/tracheal surgery, TMJ surgery Reported previous anaesthetic problems Dental damage, Emergency tracheostomy, Med-alerts, databases, previous records

10
General Examination Adverse anatomical features: e.g. small mouth, receding chin, high arched palate, large tongue, morbid obesity Mechanical limitation: reduced mouth opening, post-radiotherapy fibrosis, poor cervical spine movement Poor dentition: Prominent/loose teeth Orthopaedic/neurosurgical/orthodontic equipment Patency of the nasal passage

11
Specific Tests Basic categories
Evaluation of tongue size relative to pharynx Mandibular space Mobility of the joints TMJ Neck mobility

12
Inter-incisor Gap Inter-incisor distance with maximal mouth opening
Minimum acceptable value > 4 cm Significance : Positive results: Easy insertion of a 3 cm deep flange of the laryngoscope blade < 3 cm: difficult laryngoscopy < 2 cm: difficult LMA insertion Affected by TMJ and upper cervical spine mobility

13
Mandibular Protrusion Test
Class A: able to protrude the lower incisors anterior to the upper incisors Class B: lower incisors just reach the margin of upper incisors Class C: lower incisors cannot reach the margin of upper incisors Significance Class B and C: difficult laryngoscopy

16
Upper Lip Bite Test Class I: Lower incisors can bite the upper lip above vermilion line Class II: can bite the upper lip below vermilion line Class III: can not bite the upper lip Significance Assessment of mandibular movement and dental architecture Less inter observer variability Ref. Anesthesia & Analgesia, 2003

17
Mallampati Test Patient in sitting position
Maximal mouth opening in neutral position Maximal tongue protrusion without arching No phonation Class I: faucial pillars, soft palate, uvula visible Class II: faucial pillars, soft palate visible Class III: only soft palate visible Somsoon-Young’s modification Class IV: soft palate not visible

18
Significance of MMP Score
Class III or IV: signifies that the angle between the base of tongue and laryngeal inlet is more acute and not conducive for easy laryngoscopy Limitations Poor interobserver reliability Limited accuracy Good predictor in pregnancy, obesity, acromegaly Anesthesia & Analgesia, February 2006

19
Correlation between MMP score and laryngoscopy grade
MMP class Cormack and Lehane grade Grade 1 Grade 2 Grade 3 Grade 4 Class I (73%) 59% 14% - Class II (19%) 5.7% 6.7% 4.7% 1.9% Class III & IV (8%) 0.5% 5% 2.5% Airway Management, Jonathan Benumof
 59% 14% - Class II (19%) 5.7% 6.7% 4.7% 1.9% Class III & IV (8%) 0.5% 5% 2.5% Airway Management, Jonathan Benumof.")
20
Class Zero Mallampati Visualisation of any part of epiglottis during MMP test Associated with easy laryngoscopy Ref. Ezri et al, Anesthesia and Analgesia, 2001 Contrasting View Class zero MMP: difficult airway possible large epiglottis hinder laryngoscopic view as well as ventilation Ref. V. Grover, Canadian Journ Anesth, 2005

21
Evaluation of Mandibular Space
Thyromental distance (Patil test) Distance from the tip of thyroid cartilage to the tip of mandible Neck fully extended Minimal acceptable value – 6.5 cm Significance Negative result – the larynx is reasonably anterior to the base of tongue
 Distance from the tip of thyroid cartilage to the tip of mandible. Neck fully extended. Minimal acceptable value – 6.5 cm. Significance. Negative result – the larynx is reasonably anterior to the base of tongue.")
22
Thyromental Distance Limitations Little reliability in prediction
Variation according to height, ethnicity Modification to improve the accuracy Ratio of height to thyromental distance (RHTMD) Useful bedside screening test RHTMD < 25 or 23.5 – very sensitive predictor of difficult laryngoscopy Anesthesiology, May 2005
 Useful bedside screening test. RHTMD < 25 or 23.5 – very sensitive predictor of difficult laryngoscopy. Anesthesiology, May")
23
Sternomental Distance (Savva Test)
Distance from the upper border of the manubrium to the tip of mandible, neck fully extended, mouth closed Minimal acceptable value – 12.5 cm

24
Evaluation of Neck Mobility
Clinical methods Patient is asked to hold the head erect, facing directly to the front maximal head extension angle traversed by the occlusal surface of upper teeth Grade I : > 35° Grade II : 22-34° Grade III : 12-21° Grade IV : < 12°

25
Neck Mobility: Clinical Assessment
Flexing the head on the neck immobilize the lower cervical spine full head extension angle traversed by the vertex or forehead Significance Angle > 90° Specific test for atlanto-occipital joint extension

26
Neck mobility (contd.) Placing one finger on the patient’s chin One finger on the occipital protuberance Result Finger on chin higher than one on occiput normal cervical spine mobility Level fingers moderate limitation Finger on the chin lower than the second severe limitation

27
Combination of Predictors
Wilson Score 5 factors Weight, upper cervical spine mobility, jaw movement, receding mandible, buck teeth Each factor: score 0-2 Total score > 2 predicts 75% of difficult intubations

28
“LEMON” Assessment L - Look externally (facial trauma, large incisors,
beard, large tongue) E - Evaluate rule inter incisor gap hyomental distance 2 - hyoid to thyroid distance M - MMP score O - Obstruction (epiglottitis, quinsy) N - Neck mobility Ron and Walls’ Emergency Airway Management
 E - Evaluate rule. 3 - inter incisor gap. 3 - hyomental distance. 2 - hyoid to thyroid distance. M - MMP score. O - Obstruction (epiglottitis, quinsy) N - Neck mobility. Ron and Walls’ Emergency Airway Management.")
29
Cormack-Lehane Grading of Laryngoscopy
Grade 1: Full exposure of glottis (anterior + posterior commissure) Grade 2: Anterior commissure not visualised Grade 3: epiglottis only Grade 4: Visualization of only soft palate
 Grade 2: Anterior commissure not visualised. Grade 3: epiglottis only. Grade 4: Visualization of only soft palate.")
30
Cook’s Modification of Laryngoscopy Grade
Cormack-Lehane grade 2 & 3 2a : Posterior part of glottis visible 2b : Only arytenoids visible 3a : Epiglottis visible, can be lifted 3b : Epiglottis visible, but fixed Easy: Grade 1 and 2a Restricted: Grade 2b and 3a Difficult: Grade 3b and 4 Ref. Cook et al, Anaesthesia, 1999

31
Predictors of Difficult Mask Ventilation
Age > 55 years BMI > 26 kg/m2 History of snoring Beard Edentulous Langeron et al, Anesthesiology, November 2006

32
Predictors of Problems with Back-Up Techniques
LMA Insertion Mouth opening < 2 cm Intraoral/pharyngeal masses (e.g. lingual tonsils) Direct Tracheal Access Gross obesity Goitre Deviated trachea Previous radiotherapy Surgical collar
 Direct Tracheal Access. Gross obesity. Goitre. Deviated trachea. Previous radiotherapy. Surgical collar.")
33
Specific Tests for Assessment: Statistical significance
Predicted difficult airway Truly difficult airway Yes No TP FP FN TN

34
Statistical significance (Contd.)
Sensitivity = TP / TP + FN Specificity = TN/TN+FP Positive predictive value = TP/TP+FP Negative predictive value = TN/TN+FN

35
Statistical Significance of Bedside Predictors
Diagnostic test Sensitivity Specificity MMP class 49% 86% TMD 20% 94% Sternomental distance 62% 82% Mouth opening 22% 97% Wilson risk score 46% 89% MMP + TMD 56%

36
Radiographic Predictors
X-Ray neck (lateral view) : Atlanto-occipital gap C1-C2 gap Posterior depth of mandible- distance between the bony alveolar margin just behind 3rd molar tooth and lower border of mandible. Tracheal compression
 : Atlanto-occipital gap. C1-C2 gap. Posterior depth of mandible- distance between the bony alveolar margin just behind 3rd molar tooth and lower border of mandible. Tracheal compression.")
38
Radiologic Predictors
CT Scan: Tumors of floor of mouth, pharynx, larynx Cervical spine trauma, inflammation Mediastinal mass Helical CT (3D-reconstruction): Exact location and degree of airway compression
: Exact location and degree of airway compression.")
39
Difficult airway : specific subgroups
Pediatrics Obstetrics Obesity Systemic diseases with airway implications, e.g. rheumatoid arthritis, diabetes, ankylosing spondylitis.

40
Pediatric difficult airway
History: Past difficult intubation Airway problems associated with feeding Syndromes related to pediatric difficult airway Stridor

42
Pediatric difficult airway
Mouth opening Size of tongue Palate- narrow, high arched, cleft Schwartz-hyoid maneuver – A-P distance from middle of inside of mentum to hyoid measured: >1.5cm. (neonates), >3cm.(children). Frederic Berry’s Anesthesia for difficult pediatric patients
, >3cm.(children). Frederic Berry’s Anesthesia for difficult pediatric patients.")
43
Difficult obstetric airway: predictors
MMP Class 3 or 4 Edema of tongue, supraglottic and glottic areas; (history of rapid weight gain,pre-clampsia, change in voice) Large breasts, full dentition Mucosal congestion of nose, pharynx,etc.
 Large breasts, full dentition. Mucosal congestion of nose, pharynx,etc.")
44
Difficult airway :obesity
Difficult spontaneous ventilation in obstructive sleep apnea BMI >26 – predicts difficult mask ventilation Difficult intubation predictors- MMP Score >3 Neck circumference > 16 inches

45
Systemic Diseases : Airway Ramifications
Rheumatoid Arthritis: TMJ arthritis ( inter incisor gap, MMP score ) Cricoarytenoid arthritis (dysarthria, stridor,hoarseness ) Cervical spine mobility – ankylosis, atlanto-axial instability.
 Cricoarytenoid arthritis (dysarthria, stridor,hoarseness ) Cervical spine mobility – ankylosis, atlanto-axial instability.")
47
Diabetes mellitus: stiff joint syndrome
Palm print : Patient’s fingers and palms painted with blue ink and pressed firmly against a white paper Grade 1- all phalangeal areas visible Grade 2- deficient interphalangeal areas of 4th and 5th digits Grade 3- deficient interphalangeal areas of 2nd to 5th digits Grade 4- only tips seen. Prayer sign.

48
Difficult airway: neurosurgical perspective
Diseases of the cervical spine Trauma Pituitary disease, e.g. acromegaly Ref. Dr. Umamaheswara Rao, Indian J. Anaesth. 2005

49
Diseases of the Cervical Spine
Limited neck mobility Congenital Klippel-Feil syndrome Acquired Rheumatoid arthritis Ankylosing spondylitis Cervical spine instability Congenital Down’s syndrome CVJ anomalies Mucopolysaccharidosis Trauma

50
Klippel-Feil Syndrome
Clinical triad Cervical vertebral fusion Short neck Low-set hairline Increase likelihood of airway obstruction Cause: associated anomalies e.g. CNS Cervicomedulary junction involvement Arnold-chiari malformation Ref. Airway Management by Jonathan Benumof

51
Down’s Syndrome Atlanto-axial instability Macroglossia Sleep apnea
Associated multisystem anomalies Subglottic stenosis Hypotonia

52
CVJ Anomalies Affect the skeleton and neuraxis at the junction of cranium and cervical spine Clinical manifestations Short neck Pain and stiffness of neck Transient attacks of vertigo/unconsciousness Limb weakness Respiratory abnormalities Ref. Journal of Neurosurgical Anesthesiology, 2006

53
Assessment: Chronic Diseases of Cervical Spine
History Trauma Weakness/numbness of hands Preferred pillow height and sleeping position Clinical examination Neck posture Neck mobility Unstable cervical spine Inspection and palpation of the midline alignment of the hyoid, thyroid and spinous processes Loss of normal cervical lordosis

54
Cervical Spine Trauma: Assessment
Incidence in blunt trauma: 0.9 – 3% History Clinical examination Radiologic assessment NEXUS Criteria Low risk trauma patient No midline cervical tenderness No focal neurologic deficit Alert No intoxication No painful, distracting injury Ref. Hoffman et al, NEJM, 2000

55
Radiologic Assessment
Suspicion of CSI 3-view cervical spine X-rays Lateral A-P Open-mouth odontoid views Cervical spine CT scan Findings Fracture spine Marked prevertebral edema Malalignment Ref.: Harris et al, Spine, 2006

56
Radiologic Assessment (Cond.)
MRI Best technique to ascertain the integrity of cervical soft tissues for potential instability Recommended in patients with prolonged (> 72 hrs) depressed mental status However, MR imaging is not superior to multidetector row CT scan in detecting unstable cervical spine injuries in obtunded patients with blunt trauma Ref.: G. Hogan et al, Radiology, 2005
 depressed mental status. However, MR imaging is not superior to multidetector row CT scan in detecting unstable cervical spine injuries in obtunded patients with blunt trauma. Ref.: G. Hogan et al, Radiology,")
57
Acromegaly: Airway Implications
Macroglossia, thickened pharyngeal and laryngeal soft tissues, obstructive sleep apnea Grades of airway involvement Grade 1: No involvement Grade 2: Nasal and pharyngeal mucosa hypertrophy Grade 3: Glottic involvement e.g. glottic stenosis/ vocal cord paresis Grade 4: Grade (2+3) Ref. British Journal of Anaesthesia, 2000
 Ref. British Journal of Anaesthesia,")
58
Australian Incident Monitoring Study (AIMS)
Most useful aid- GEB, introducer 3 most common contributing factors Obesity Limited neck mobility Limited mouth opening Most common complications Desaturation Esophageal intubation Inadequate preoperative assessment was the most common remediable cause

59
Guidelines vs Protocols
Guidelines- good clinical practice general recommendations deriving from a systematic analysis of available literature, resources that allow for individual interpretation. Protocols- based on definitive clinical evidence that mandates adherence to specific recommendations.

60
ASA task force on management of DA (Anesthesiology May 03;98)
Explicit descriptions of DA Difficult face mask ventilation Difficult laryngoscopy Difficult tracheal intubation Failed intubation Purpose- facilitate mx. of DA, ↓adverse outcomes Focus on anaesthesia care All locations, all ages

61
ASA task force on management of DA
Basic preparation Inform Ascertain help Preoxygenation Supplemental oxygenation throughout Portable storage unit Rigid laryngoscope blades ETTs ETT guides LMAs FFOI equips RI Em NI a/w vent Em invasive a/w Exhaled CO2 detector

62
ASA task force on management of DA
Strategy depending on Anticipated surgery Patient condition Skill & preference of anaesthesiologist 4 basic problems 3 basic management choices Primary approach Alternative approach Exhaled CO2 to confirm tracheal intubation

64
LMA in ASA DA algorithm

65
ASA task force on management of DA
Strategy for extubation of DA Awake? Adverse impacts on ventilation Further A/w management plan Guide for reintubation Follow up

66
Limitations of ASA guidelines
Open ended, wide choice of techniques Emphasis on prediction of difficult airway No stratification of available a/w devices No expression of strength of recommendation

67
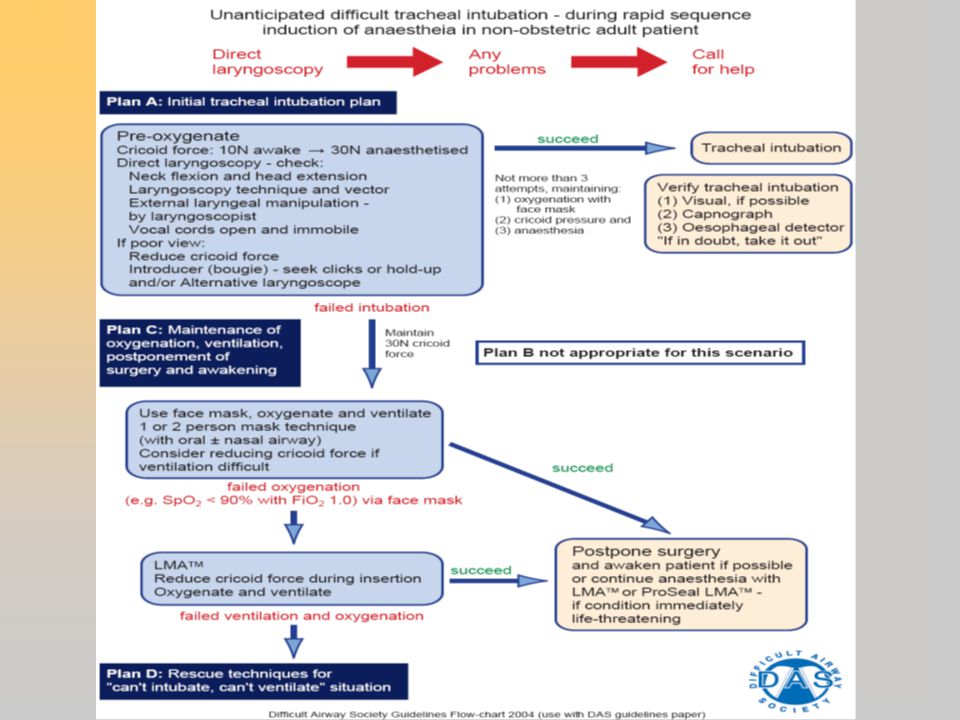
DAS guidelines (Anaesthesia.2004.59)
Management of un-anticipated difficult intubation in an adult non-obstetric patient Paediatric, obstetric patients & patients with upper a/w obstruction excluded Flow charts based on series of plans Careful planning with backup plans Maintenance of oxygenation takes priority Seek the best assistance available

71
SIAARTI guidelines (Minerva Anesthesiol 2005;71:617-57)
Doesn’t apply to paediatric patients Defines strength of expressed recommendation Defines difficult a/w control, ventilation, intubation & laryngoscopy Difficulty prediction (severe/borderline) Devices managament Mandatory Other devices, available upon request Other mentions
 Devices managament. Mandatory. Other devices, available upon request. Other mentions.")
72
SIAARTI guidelines (Planning in unpredicted difficult a/w)
Correct position Alternative options (blade/stylet/introducer/ magill’s) Oxygenation is mandatory Urgency/ emergency of procedure Elective sx Deferrable urgent sx Emergent sx
 Oxygenation is mandatory. Urgency/ emergency of procedure. Elective sx. Deferrable urgent sx. Emergent sx.")
73
SIAARTI guidelines (Planning in unpredicted difficult a/w)
Immediate withdrawal in CL – IIIe & IV Preliminary knowledge of alternative devices, training in FOI Blind intubation via extraglottic devices not recommended in emergency/ after repeated attempts Use of fiberscope in emergency situations is not recommended

74
SIAARTI guidelines (Planning in predicted difficult a/w)
Strategy depends upon Surgery deferrability Risk of vomiting Skill of anaesthesist Available instrumentation Patient cooperation Grade of predicted difficulty

75
SIAARTI guidelines (Planning in predicted difficult a/w)
Predicted severe DA Maintain consciousness, spont. Breathing 1st choice – awake FOI Surgery under RA not recommended Intubation under direct vision Retrograde intubation as an alternative to FOI

76
SIAARTI guidelines (Planning in predicted difficult a/w)
Predicted severe DA Anaesthesia can be induced Preoxygenation & ventilability evaluation Laryngoscopy grading influences further choice CVCI 1st choice- cricothyrotomy Surgeons intervention as an exception

77
DA in paediatric patients (SIAARTI guidelines, Minerva Anesthesiol 2006;72:723-48)
Important anatomic & physiologic differences Lack of cooperation Intuabtion using sedoanalgesia/ GA+ topical LA Preoxygenation mandatory Maintain spontaneous breathing, check FM ventilability

78
DA in paediatric patients (SIAARTI guidelines)
Strategy depending on laryngoscopy view Post comm→ change blade/stylet/introducer Epiglottis only → introducer Limited view of epiglottis → FOI No laryngeal structure → FOI Blind intubation not recommended CVCI Early use of LMA/EGA Crocothyrotomy, TTJV

79
Failed intubation in obstetrics
Incidence- 1 in 300 to 1 in 750 Original description by Tunstall (Anaesthesia 1976;31:850) DAS guidelines may readily be extrapolated to pregnant patients Editorial, Int J Obs Anesth Jan2007;16
 DAS guidelines may readily be extrapolated to pregnant patients. Editorial, Int J Obs Anesth Jan2007;16.")
80
Failed intubation in obstetrics (IJOA Jan2007;16:173)
")
81
Airway management in trauma
Challenges

82
Airway management in trauma
Scientific evidence RSI MILS Tracheal tube introducer for routine use Selection of laryngoscope blades (Mac/McCoy) LMA as a temporary adjunct (Emerg Med J 2006;23:3-11)
 LMA as a temporary adjunct. (Emerg Med J 2006;23:3-11)")
83
Airway management in trauma
RSI involves 4 experienced personnel AMPLE history (ATLS course manual 1997) Allergies Medication Past medical history time of Last meal Events leading to OET is the technique of choice No definition of safe cx spine ovement Equipment option depend on operator experience & skill
 Allergies. Medication. Past medical history. time of Last meal. Events leading to. OET is the technique of choice. No definition of safe cx spine ovement. Equipment option depend on operator experience & skill.")
84
Airway management in trauma (Emerg Med J 2006;23:3-11)
")
85
Cervical Spine Injury: Management Options
Manual in-line stabilization Airway interventions requiring less neck movement Jaw-thrust (ventilation) Adjunctive device ILMA, combitube Cricothyrotomy Least movement (0.1 mm) with fibre optic nasal intubation Ref.: Brimacombe et al. Anesth Analg 2000
 Adjunctive device ILMA, combitube. Cricothyrotomy. Least movement (0.1 mm) with fibre optic nasal intubation. Ref.: Brimacombe et al. Anesth Analg")
86
Influence of laryngoscope blade
No difference between Macintosh and Miller blades McCoy laryngoscope Angulated tip Improves visualisation with less force, in neutral position Ref.: Anaesthesia, 1999 Bullard laryngoscope Rigid fibreoptic laryngoscope Alignment of axes not required Ref.: Hastings et al. Anesthsiology, 1995

87
Management Options (Contd.)
Flexible fibre optic bronchoscopy Advantages Minimal cervical movement required Ability to perform post intubation neurologic assessment Most appropriate technique for intubation in patients with CSI still debated No clinical outcome data to suggest better neurologic outcome with any single technique Ref.: Crosby et al, Anesthesiology, 2006)
")
88
Airway Management: Acromegaly
Large face-masks, long-bladed laryngoscopes Grade 3 or 4 Fibreoptic intubation Tracheostomy Ref. British Journ Anaesth, 2000 Secondary intubation techniques Intubating LMA Ref.: J Neurosurg Anesthesiol, 2004 Gum-elastic bougie Ref. J Neurosurg Anesthesiol, 2006

89
Tracheal Extubation in the Difficult Airway
Risk factors: Difficult reintubation History of previous difficult intubation Airway edema due to surgical manipulation or volume resuscitation Morbid obesity Burns or smoke inhalation Immobilized/unstable cervical spine Ref.: A. Rudra et al. Indian J Anaesth, 2006

90
Difficult Airway: Extubation Strategies
ASA Recommendations Relative merits of awake extubation versus extubation before return of consciousness Evaluation of factors that may impair ventilation after extubation Formulation of airway management plan if there is inadequate ventilation after extubation Ref.: ASA Practice Guidelines, Anesthesiology, 2003

91
Extubation strategies
Cuff leak test Performed in a spontaneously ventilating patient at risk of obstruction after extubation Circuit disconnected occlusion of ETT end and deflation of cuff ability to breath around the ETT Ref.: Fisher et al, Anaesthesia, 1992

92
Extubation Strategies
Conventional awake extubation Extubation in a deep plane of anaesthesia followed by placement of LMA to decrease the risk of laryngospasm Ref.: Brimacombe et al, Anaesthesiology, 1996 Extubation over a fibreoptic bronchoscope Ref.: Cooper et al, Anesth Clin North America, 1995 Endotracheal ventilation and exchange catheters e.g. Cook’s airway exchange catheter Tracheal tube exchanger Ref.: A. Rudra et al, IJA, 2006

93
Thank You

Similar presentations





























 ภาควิชาวิสัญญีวิทยา วิทยาลัยแพทยศาสตร์ กรุงเทพมหานครและวชิรพยาบาล.>")