Download presentation
Presentation is loading. Please wait.

1
Primary treatment of constipation Explanation of symptoms and education Ensure adequate fluid intake (1500 mls) Adequate, but not excessive, fibre intake (suggested 30gm fibre per day). This should be in a mixture of formats rather than just adding cereal fibre to the diet Increase daily exercise if possible (massage??)
.")
2
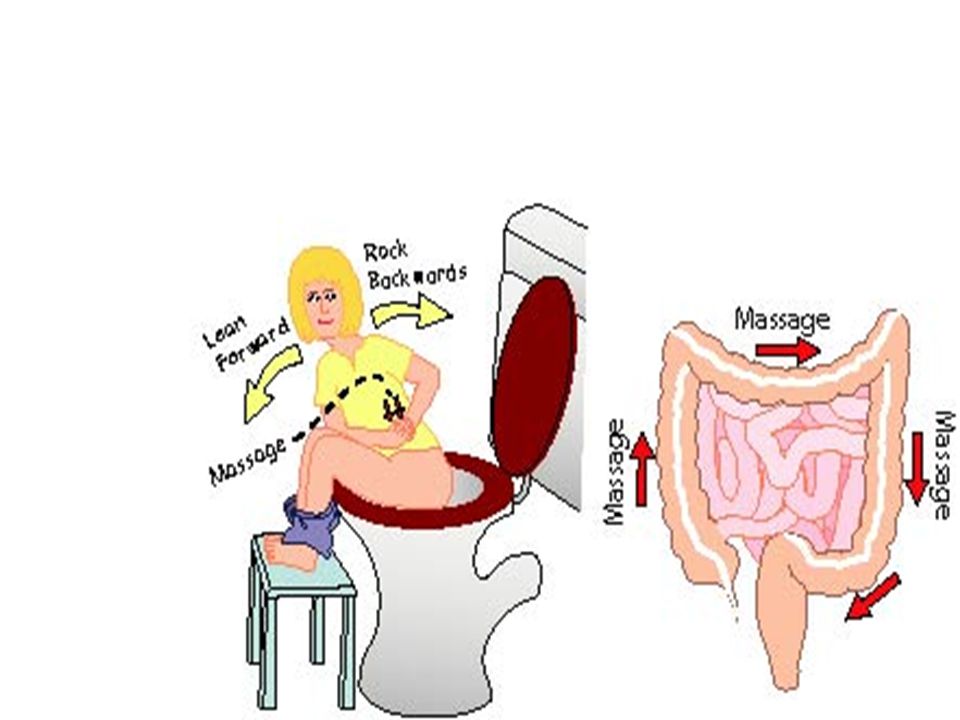
Retraining for chronic constipation - 1 Educate the patient about normal bowel activity Stop all laxatives Eat breakfast and take a warm drink Capitalise on the gastro-colic response by attempting to use the toilet approximately 20-30 minutes after breakfast Sit on toilet with feet raised on a footstool

5
Retraining for chronic constipation - 2 Use abdominal muscles to expel stool, but do not hold breath and strain Review medications and change those likely to cause constipation if possible Glycerin suppositories may help for 1-2 weeks to get a regular bowel habit established, but always review this after 2 weeks.

6
Biofeedback for constipation Show patient paradoxical EAS contraction (EMG): learn to relax Rectal sensation training Abdominal EMG: pushing correctly? No evidence that biofeedback better than verbal training in adults or children May help “sell” the exercises to sceptical patients?

7
Rational use of laxatives Most become less effective with time Some cause abdominal discomfort and bloating Response seems very individual Very limited evidence base Rectal vs. oral? What to try first –Symptoms, past history, what else??

8
Laxatives: non-impacted Address diet, fluid, toilet, exercise, habit Evacuation difficulty – suppository or micro enema Hard stool – bulk laxative Symptoms persist – add stimulant Symptoms persist – try osmotic agent (Emmanuel 2002)
")
9
Impaction Exclude organic disease Non-ambulant: enemas Ambulant: osmotic eg magnesium sulphate or macrogols (Emmanuel 2002)
")
11
When to use manual evacuation? Faecal impaction / loading Incomplete defaecation Inability to defaecate Other bowel emptying failed Neurogenic bowel dysfunction Spinal Cord Injury

13
Anal electrical stimulation Suggested should improve muscle function Strong enough current @ 35Hz : involuntary muscle contraction Used especially when voluntary contraction very weak

14
Anal electrical stimulation: RCT Biofeedback waiting list Recruited, NO ASSESSMENT OR ADVICE OR EXERCISES Randomised (blinded) to 35Hz or 1Hz 8 weeks use at home Manometry, diary, symptom questionnaire before & after Patients’ evaluation after
 to 35Hz or 1Hz 8 weeks use at home Manometry, diary, symptom questionnaire before & after Patients’ evaluation after")
15
Results 90 patients randomised 43 sham (1Hz), 47 active (35 Hz) 70 completed No differences active & sham detected Median rating +2 (-5 to +5 scale) Median satisfaction 5.5/10 Sensitisation may be more important than strenthening?? (Norton et al 2006, DCR Feb)
.")
16
Summary Biofeedback is a tool to help patients learn about bowel function and how to control it Patient teaching and education may be the most important part Biofeedback useful with some patients But you CAN run a good service without fancy equipment

Similar presentations












>")









