Download presentation
Presentation is loading. Please wait.

1
‘Doctor, my 5 year old is constipated’
Dr. Sadananda

2
Constipation Difficulty or delay in passage of stool
< 3 per week/less often than normal may be associated with pain / discomfort stools not necessarily hard rectum usually full

3
‘Soiling’ Often referred to as ‘constipation with overflow’
inappropriate passage of stool in underwear associated with chronic constipation faeces often loose and ‘smelly’ involuntary action over which child has no control

4
Encopresis Term first used in 1926 to suggest similarity with ‘enuresis’ for wetting Inappropriate passage of normal stool Stool passed in pants or deposited ‘elsewhere’ (where it can be found!) Normal bowel sensation Often associated with other behavioural problems
 Normal bowel sensation. Often associated with other behavioural problems.")
5
Causes of constipation in childhood
‘Holding on’ - often initiated by passage of large / painful stool delay in passage of normal stool anal fissure group ‘A’ hemolytic streptococcal anal infection toilet phobias / fears Child sexual abuse

6
Causes of constipation (continued)
Functional faecal retention -usually associated with soiling follows from ‘holding on’ unless managed appropriately symptoms of increasing faecal loading - soiling/irritability/abdo pain/anorexia symptoms resolve on passage of stool May require long term treatment and follow up

7
Causes of constipation (contd)
Hypothyroidism Polyuria causing dehydration in DM, Diab insipidus Lead poisoning Cows milk intolerance

8
Constipation – environmental issues
School toilets! Toilet cold/dark Toilets dirty Uncomfortable Lack of privacy Lack of toilet paper inaccessible

9
Constipation – psychological factors
Fear / anxiety Precipitating family stress Learned behaviour ? Coercive potty training ‘Cry’ for help

10
Assessing constipation
‘Red flag’ symptoms include: > 48 hours before passing meconium as a neonate Abdominal distension esp if failing to thrive Infrequent small or ribbon stools Constant leaking especially if linked with urinary leaking too Failed management with appropriate standard intervention (with compliance)
")
11
General health profile
Check for: daytime urinary problems nocturnal enuresis appetite / fibre intake fluid intake - how much milk? any medical problems any current medication

12
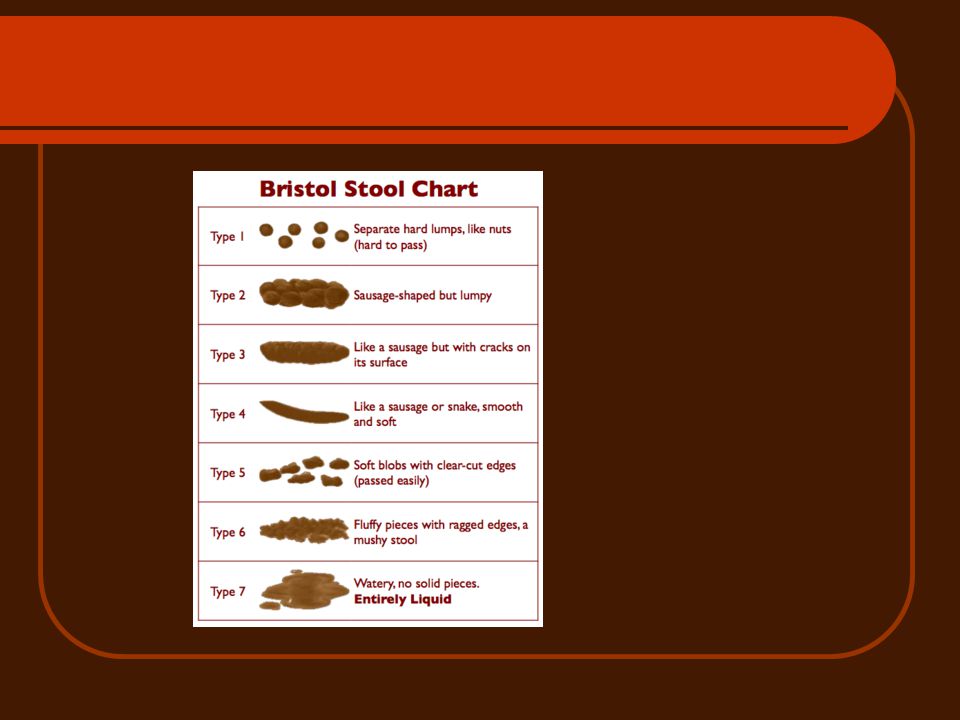
Bowel profile Check passage of meconium description of stools
- frequency - consistency - size - any pain /discomfort/blood/mucus may utilise ‘Bristol Stool Form Chart’ developed by Heaton use of toilet / potty any previous treatments /interventions

14
Toilet training profile
Age toilet training commenced age acquired bladder control age acquired bowel control (if appropriate ) any significant changes / problems / events occurring at this time
 any significant changes / problems / events occurring at this time.")
15
Constipation and soiling – Management Overview
Education Evacuation Maintenance

16
Constipation - management
Demystification – child and family need to be aware of: Normal variation in bowel habits Protracted course of treatment Relapses common Long term laxatives often required -only to be stopped on advice Symptoms may get worse initially

17
Treatment of constipation
consistent scheduled toileting positive reinforcement diet / fluid adjustment oral laxatives Suppositories/enemas only as very last resort and if tolerated by child

18
How much fluid? ‘ensure adequate fluid intake’
e.g. 4 year old weighing 16 kg - needs 85ml/kg = 1360 ml aim for 6-8 cups throughout the day encourage water based drinks

19
How much fibre ? There are no ‘DRA’ for fibre for children
the daily recommended intake is the amount required to produce a soft stool suggested daily intake is ‘age +5g fibre

20
Evacuation Traditionally softened stools first using osmotic laxative e.g. lactulose/docusate Then introduced stimulant e.g. senna Added Sodium picosulphate or similar if poor result Enema or EUA if above failed Poor compliance and protracted treatment time

21
Evacuation - Single step Approach
Movicol Paediatric Plain -majority of children can undergo single line treatment with appropriate dose titration. Children find enemas very distressing and should only be given to children as a very last resort

22
Disimpaction Movicol Paediatric Plain :2-4years 2-8 sachets, 5-11 years 4-12 sachets – to start with minimum number of sachets for age and increase every other day until evacuation complete (usually within 7 days). Sachets can be taken in divided doses but total daily dose should be taken within 12 hours. Movicol: Adult dose 8 sachets per day for 3 days
. Sachets can be taken in divided doses but total daily dose should be taken within 12 hours. Movicol: Adult dose 8 sachets per day for 3 days.")
23
Laxative Dosage Lactulose: <1 year, 2.5ml bd; 1-5 years 5ml bd; 5-10 years 10ml bd; adult 15 ml bd Docusate (oral solution): 6 months to 2 years 12.5 mg tds; 2-12 years 12.5 – 25 mg tds; adult up to 500 mg/day in divided doses Senna (syrup): 2-6 years 2.5 – 5ml in morning, over 6 years 5-10 ml; adult ml usually at bedtime. Movicol Paediatric Plain: 2-6 years 1-4 sachets, 7-11 years 2-4 sachets per day (titrate dose as necessary) Movicol: adults 1-3 sachets per day
: 6 months to 2 years 12.5 mg tds; 2-12 years 12.5 – 25 mg tds; adult up to 500 mg/day in divided doses. Senna (syrup): 2-6 years 2.5 – 5ml in morning, over 6 years 5-10 ml; adult ml usually at bedtime. Movicol Paediatric Plain: 2-6 years 1-4 sachets, 7-11 years 2-4 sachets per day (titrate dose as necessary) Movicol: adults 1-3 sachets per day.")
24
Maintenance Use adequate doses to pass stool one every 1-2 days
May need to use a combination of stool softener/bulking agent and bowel stimulant (e.g. lactulose and senna) or Movicol Paediatric Plain Will need at least 6 months treatment and often much longer to learn/re-learn bowel habit
 or Movicol Paediatric Plain. Will need at least 6 months treatment and often much longer to learn/re-learn bowel habit.")
25
Finishing treatment Gradual reduction
Reduce bowel stimulant (if using) first Treat early if relapse
 first. Treat early if relapse.")
26
Managing soiling and encopresis

27
Assessing the soiling problem
Is the child soiling because of: Delayed bowel control Overflow soiling with underlying constipation Encopresis

28
Soiling profile Age at onset of soiling duration of soiling
frequency of soiling description of soiling - consistency - volume

29
Behaviour / school profile
general behaviour at home and school any reported problems associated with the toilets any reported bullying

30
Child’s feelings What are child’s feelings about using the toilet - at home and school? does child willfully ‘hold on’ to stool? what are child’s feelings about the soiling? what does the child think is the cause of the soiling?

31
Family feelings How do parents view soiling?
How do they manage when it happens? What do they do when it doesn’t happen?

32
Treatment -’whole child’ approach
Families often perceive the main problem is the ‘soiling’ constipation secondary issue emphasis needs to be made on poos in the toilet NOT clean pants engaging the child to sit on the toilet and perform often most difficult part of treatment

33
Medication Need to treat any underlying constipation first
Fine tune treatment to avoid constipation, but prevent diarrhoea Maintain for at least 6 months Then consider cautious dose reduction Advice family appropriately if relapse occurs Short term goals, positive reinforcements

34
Summary History- fluid/ fibre intake, environmental issues, r/o red flags, any soiling/ encopresis Examination Management – education, evacuation, maintenance

Similar presentations
















 Adequate, but not excessive, fibre intake.>")

 By Mohammad Adnan.>")
