Download presentation
Presentation is loading. Please wait.

1
Scott D. Mist PhD, LAc K Jones, C Sherman, F Li, R Bennett, J Fisher OHSU/ORI R21 AR5335061-2 (NIAMS)
.")
2
Fibromyalgia (FM) is diagnosed in 6 to 12 million Americans, primarily women; annual costs exceeding $20 billion Multisymptomatic chronic pain illness with significant physical fitness limitations Average 40 year old FM patient demonstrates physical fitness scores found in a healthy person in their 8th decade Wolfe, 1995, Arth Rheum; Wolfe, 1997, Arth Rheum Jones 2010 J MS Pain; Jones 2009 NA Dis Clin Carson, 2010, Pain
 is diagnosed in 6 to 12 million Americans, primarily women; annual costs exceeding $20 billion Multisymptomatic chronic pain illness with significant physical fitness limitations Average 40 year old FM patient demonstrates physical fitness scores found in a healthy person in their 8th decade Wolfe, 1995, Arth Rheum; Wolfe, 1997, Arth Rheum Jones 2010 J MS Pain; Jones 2009 NA Dis Clin Carson, 2010, Pain")
3
>90 exercise studies in FM have been published to date. Most indicate that higher intensity programs, regardless of mode, result in improved physical fitness, but often worsen pain. Recently, exercise that employs a mind/body component has been found to be effective in FM.

4
Previous research has suggested that Tai chi offers a therapeutic benefit in patients with FM How much are physical fitness variables improved (balance, strength, aerobic conditioning, flexibility)? What is the mechanism(s) of action of pain reduction? What is the optimum frequency, intensity, timing and type/mode? Taggart, 2003, Orthop Nurs Wang, 2010, NE J of Med
 of action of pain reduction. What is the optimum frequency, intensity, timing and type/mode. Taggart, 2003, Orthop Nurs Wang, 2010, NE J of Med.")
5
Single-blind Randomized 12 week trial of 8-form Yang style, group Tai chi Compared to group wellness education Non-academic, community setting

6
Supervised group 8 form Yang style ◦ simplified from 24 form ◦ both static and dynamic Dose: 90 minutes, twice weekly x 12 weeks 15 min warm up 45 min Tai chi training 15 min break 15 min cool-down Progressive based on mastery and Borg PE scale. 1 Interventionist

8
Supervised group education Including diagnostic criteria, pacing, problem solving, diet, sleep, pain management, medications, mental health, wellness and lifestyle management. 3 Interventionist: MD, RD/LD, MSW. Same interventionists and curriculum for all 5 waves. Dose: 90 minutes, twice weekly x 12 weeks.

9
Examiners blinded Medications monitored/not washed out Adherence defined as number of classes attended Enrollment occurred in 5 waves with randomization by computer generated numbers blocking on age Tai chi DVD given to all participants after final data collection Treatment expectations

10
40 years of age or older with FM per 1990 ACR Independent ambulators without assistive devices MD clearance for exercise within past 3 months Willingness for random assignment Willing to keep all treatments/meds steady Absence of dyscognition (>3 Pfeiffer Mental Status) Excluded: Tai chi training within the past 6 months, or exercising > 30 mins/3x weekly for past 3 months Serious medical conditions that might limit their participation Planned elective surgery during study period
 Excluded: Tai chi training within the past 6 months, or exercising > 30 mins/3x weekly for past 3 months Serious medical conditions that might limit their participation Planned elective surgery during study period")
11
Oregon Health & Science University FM database Oregon Research Institute database Local support group Local health care providers Oregon Pain Society in Eugene, OR

12
The primary end point was between group differences in change scores on FM symptom severity and physical function (Fibromyalgia Impact Questionnaire [FIQ] total) at the end of 12 weeks.
![The primary end point was between group differences in change scores on FM symptom severity and physical function (Fibromyalgia Impact Questionnaire [FIQ] total) at the end of 12 weeks.](http://images.slideplayer.com/14/4413256/slides/slide_12.jpg "The primary end point was between group differences in change scores on FM symptom severity and physical function (Fibromyalgia Impact Questionnaire [FIQ] total) at the end of 12 weeks.")
13
The end point was between group differences in change scores on pain at the end of 12 weeks. Pain was measured with Brief Pain Inventory (BPI severity & interference) and VAS FIQ #15.
 and VAS FIQ #15..")
14
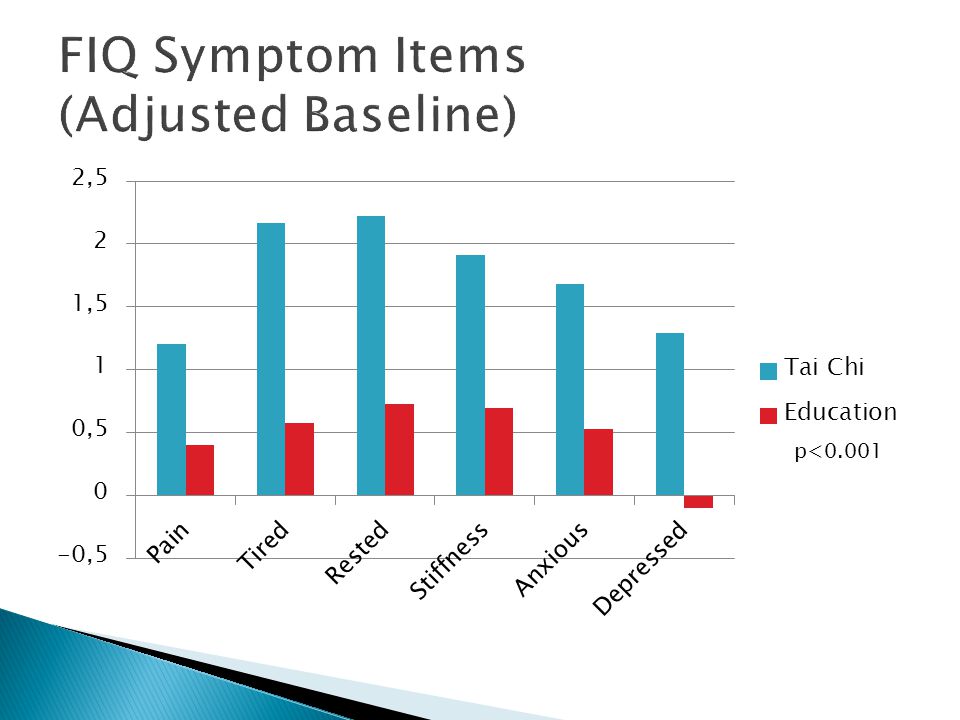
Pittsburg Sleep Quality Index - Global FIQ symptoms FIQ physical function Static balance (stork) Dynamic balance (forward reach) Timed- get up and go Upper body flexibility
 Dynamic balance (forward reach) Timed- get up and go Upper body flexibility")
15
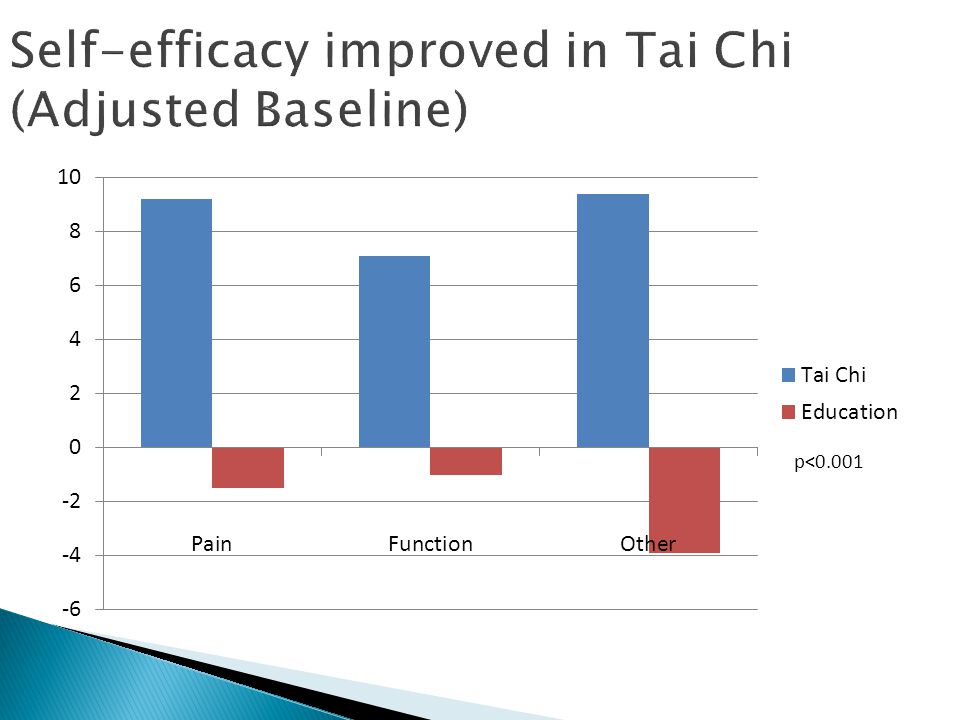
FIQ total and pain outcomes will be mediated by change in ASES (self- efficacy for pain control and symptom control)
")
16
Powered off 4 FM exercise studies and 1 Tai Chi study in older adults without FM Assumption: 80%power to detect 15% between group differences in FIQ Allow for 20% drop out, final n=96 Intent to treat analyses

17
Conditional change score analysis adjusting for centered baseline 1 Similar to two group mean comparison t-test Advantages of method ◦ Less artifact of regression to the mean ◦ Lessen baseline differences if present ◦ Lower Standard Error (More accurate estimate of treatment effect) 1 Aickin M, The Permanente Journal, Spring 2009
 1 Aickin M, The Permanente Journal, Spring 2009")
18
Age: 54 years (range 40.7 – 74.1) 93% female 96% Caucasian Body mass index: 30.5 2+ Rx for FM (non-narcotic analgesics and anti- depressants) Symptomatic 18.4 years Approximately half did not work outside the home despite that fact that 85% had attended or graduated from college FIQ total of 63.9 pain VAS of 7
 93% female 96% Caucasian Body mass index: 30.5 2+ Rx for FM (non-narcotic analgesics and anti- depressants) Symptomatic 18.4 years Approximately half did not work outside the home despite that fact that 85% had attended or graduated from college FIQ total of 63.9 pain VAS of 7")
28
IV: Education Change FIQ Total/FIQ Pain IV: Tai Chi Step 1 p=0.0002 Self Efficacy Change FIQ Total/FIQ Pain Step 2 p=0.0018 Self Efficacy IV: Education Change FIQ Total/FIQ Pain IV: Tai Chi Step 3 p=0.0001 p=0.003 p=0.016

29
12 weeks of supervised group Tai chi improves FM symptoms including pain and fitness Findings were both clinically and statistically significant FIQ, pain and sleep on PSQI Replicated Wang’s Tai Chi study and reproduced improvement in FM symptoms Extending Wang’s work by examining more fitness variables

30
Single blind vs. double blind Optimum length of intervention unknown as improvements were seen at endpoints in both Wang’s and our study Findings may not generalize to men, children or minorities Tai Chi master-intervention or interventionist?

31
Longer study to quantify most efficacious dose Multi-sited trial or multiple interventionists Laboratory based fitness testing for 1RM, postural stability, V0 2 max Laboratory based pain testing such as QST, NFR and neuroimaging

Similar presentations



























. - FM is one of the main causes of Chronic Widespread Pain (CWP).>")
