Download presentation
Presentation is loading. Please wait.

1
Stephen J. Hughes, MD, Nianne VanFleet, RN, Martha Williams, RN Gannett Health Services, Cornell University

2
Describe how to set up a Nurse assessment/dedicated clinician team for rapid assessment/treatment of patients

3
Expectations of patients Selection of team members Development of trust within the team Logistics

4
More rapid assessment/treatment of relatively uncomplicated patients Dedicated clinician available to RNs for consultation Dedicated clinician for review of U/As, etc. Other clinicians not distracted by need to consult with RNs Team-building experience

5
Private/Public Institution – 7 colleges, Graduate School, Law School, Business School, Veterinary School –( Medical School is 250 miles away) ~ 22,000 students, ~ 1/3 graduate and professional “ centrally isolated” – school is in central NYS – significantly-sized cities 60+ miles away Highly stressed - higher expectations for RAPID, HIGHest Quality care
 ~ 22,000 students, ~ 1/3 graduate and professional centrally isolated – school is in central NYS – significantly-sized cities 60+ miles away Highly stressed - higher expectations for RAPID, HIGHest Quality care")
7
~ 27,000 visits with physicians, NPs, PAs ~ 10 FTE MD/DO,NP,PAs ~ 9.5 FTE RNs ~ 22,000 immunizations/Tb testing (RN) ~2000 Travel Clinic (RN) ~ 2400 Allergy Clinic (RN)
 ~2000 Travel Clinic (RN) ~ 2400 Allergy Clinic (RN)")
8
Patients would have appointments with clinicians or alternatively could see an RN for simple URIs, dysuria(women), contraceptive 3 mo. F/U or extensions, Emergency Contraception (“old” days), suture removal, wound care, HIV testing, preliminary visit prior to Fullbright, Peace Corps, other Physicals
, suture removal, wound care, HIV testing, preliminary visit prior to Fullbright, Peace Corps, other Physicals.")
9
Nurses would “spin” seeking clinician consultant Clinicians would be interrupted NP/PAs would compete with RNs for physician consulting time Some clinicians would become “favorites”, some were avoided

10
RN EXAMINING PATIENT RN USING ASSESSMENT SKILLS

19
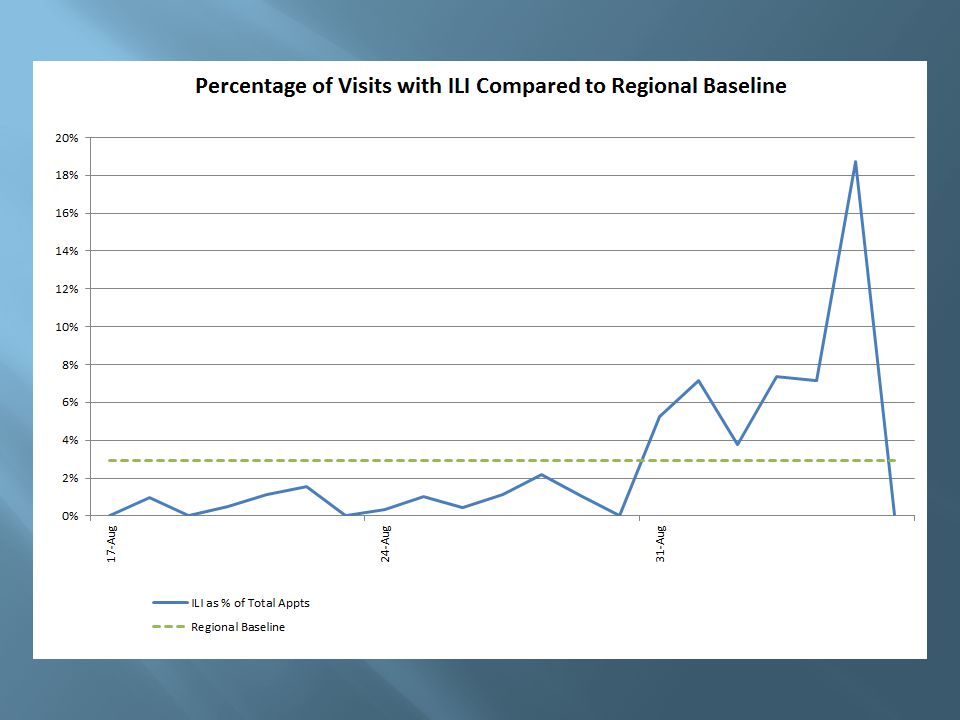
1725 flu/ILI pts seen at Gannett of 1837 1 student death Website information Beefed up phone assessment/ F/U availability – 5178 calls Trial of SPIDER – physician or NP or PA – no patients booked with clinician – as many as 5 RNs with very good assessment skills assigned to floor designated for “respiratory illnesses”

20
ILI threshold was set pretty low by CDC- ultimately “fever or perception of fever” and cough or sore throat. These patients were presented to the Spider clinician by the RN, many were examined by the clinician, including patients with higher-risk medical conditions, who made decisions about home care, medications, CXRs, etc. Telephone follow up was done by nurses, Health Educators, other Health Center staff and campus volunteers

21
Expectations of patients Selection of team members Development of trust within the team Logistics

24
Best diagnostician in the world hanging on a hook in my closet that I can bring out whenever I feel the need. Ability to diagnose my problem by listening to whatever I have to say without doing tests, asking more than three questions, or contradicting anything I have read on ANY website or anything my parents or friends have told me Ability to successfully treat – and completely cure – my problem(s) at essentially no out-of- pocket cost to me – within three days – sooner, if I have an exam, paper or social function coming up in one or two days
 at essentially no out-of- pocket cost to me – within three days – sooner, if I have an exam, paper or social function coming up in one or two days.")
27
A staff dedicated to providing the best care possible given the constraints under which we work Rapid, accurate, minimally invasive assessment of problem Comprehensible explanation of diagnosis and plan Rapid communication of lab tests, x-ray reports, etc. Willingness to work with patients to provide best possible outcome

28
Excellent Assessment Skills Must be willing to expand these skills and add to knowledge of illnesses, treatment options Must be able to adapt to different clinicians’ styles Must be able to communicate well with patients and clinicians

29
Must be comfortable letting go of a certain level of control Must trust the assessment skills of the nurse but be prepared to re-examine patient Must be willing and able to teach nurse about physical exam, disease entities, treatment options Must be comfortable with multi-tasking

30
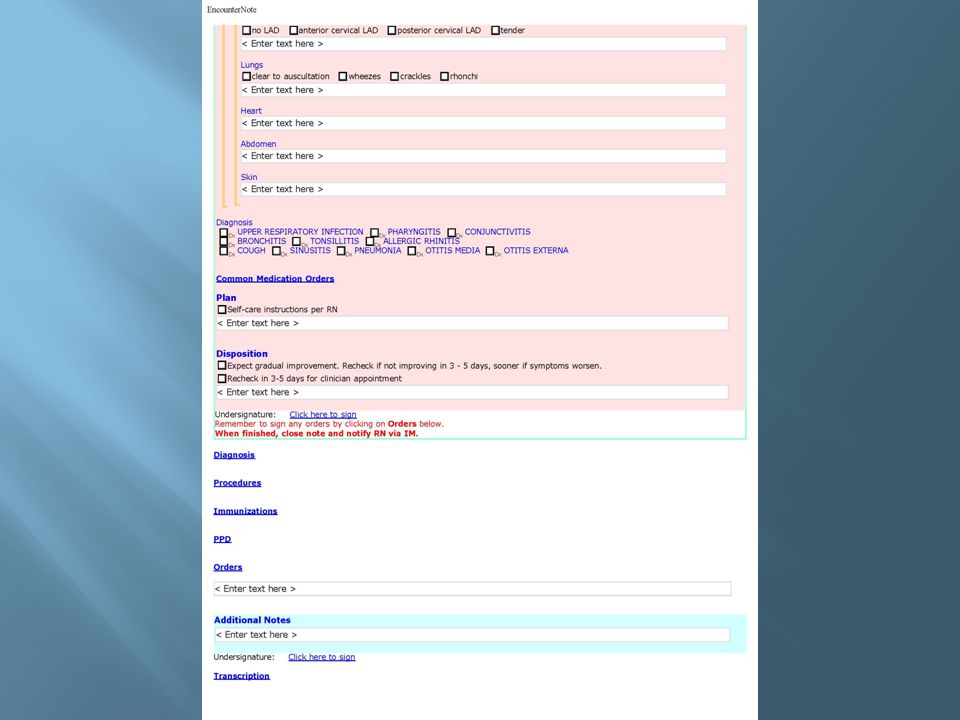
Cornell uses Point and Click EHR – there are ways to “Share” a note or “Send” a note. We can “drop in” a Spider consult section – (custom made by us) – to facilitate documentation. We can order lab tests, x-rays, medications in the EHR. We can Secure Message a nurse to follow up (call or secure message or both) with a patient the next day
 – to facilitate documentation. We can order lab tests, x-rays, medications in the EHR. We can Secure Message a nurse to follow up (call or secure message or both) with a patient the next day.")
31
Allow rapid communication between RNs and clinicians Allow ordering of labs, medications, possibly x-rays – with E-signing by clinician Allow Sharing and/or Sending of notes between nurses/clinicians

34
Pass the paper chart around

35
The Clinician – NP/PA or Physician

36
Swift Proficient Integrated Decisive Effective Resourcing

39
Time Shared experience Communication De-selection of certain members

40
Appropriate space Set expectations for the team Appropriate rules

41
Three types of nurse visits on Level 4: Nurse managed - no consult necessary - nurse completes note Needs Consult - (ex: sinus pain, flu, ear infection, etc.) – shared note between nurse and clinician. (Use the Spider drop in template) Complicated Case -consult with Spider who may request it be moved to an appointment with them if possible or another clinician.
 Complicated Case -consult with Spider who may request it be moved to an appointment with them if possible or another clinician..")
42
All Virtual Dysuria and Contraceptive Only consults Nursing orders for immunizations or a rabies series (for a non-bite type exposure, such as a Bat) Patients with cough/cold/sore throat visit that are seen on Level 6 (this is only done if Level 4 is backed up), the nurse will come to Level 4 to consult with Spider.
 Patients with cough/cold/sore throat visit that are seen on Level 6 (this is only done if Level 4 is backed up), the nurse will come to Level 4 to consult with Spider.")
43
Other types of nurse visits that are scheduled on Level 6 (wound check, suture removal, etc.) that need a consult can be done by the Spider if she is not busy and is available for a consult. Otherwise consult with a Level 6 clinician.

44
The AM Spider will be available for consult from 8:30 - 1:00pm The PM Spider will be available for consult from 1:00 - 5:00pm The Spider should never be scheduled as the late clinician. The Spider should not have meetings or blocks scheduled during their Spider time. The team leader on Level 4 will monitor the Spider’s schedule, if the Spider is not busy, she may schedule non-complicated appointments with the Spider.

45
RNs really appreciated decreased waiting time to consult with a clinician Clinicians who had full schedules of patients really appreciated not being interrupted by consults Able to set RN appointments on a different floor for many pre-bookable issues (contraceptive f/u, wound care, etc.) so patients not “stuck” waiting behind many with sick visits More physician time for consult with NP/PAs Continuing to refine Spider concept
 so patients not stuck waiting behind many with sick visits More physician time for consult with NP/PAs Continuing to refine Spider concept")
46
Know ahead of time what the parameters are Agree on the approach Improves team – morale/spirit Decrease wait time RN satisfaction Patient satisfaction Freed up physicians to do higher level care Clinician satisfaction

47
Can be inefficient, repetitive evaluations, duplication of documentation Can have a disparity of patient loads Often a swamp of labs next day – esp. Strep Cultures ordered during Spider time and sent to NP/PA when not Spider is cumbersome Can have high intensity and complicated visits rather inappropriate for RN visits (due to lack of clinician appointments) Liability / RN scope of practice (NY), evolving protocol, provider liability for RN “curbside” consult One additional layer of triage/evaluation which can extend time in clinic
 Liability / RN scope of practice (NY), evolving protocol, provider liability for RN curbside consult One additional layer of triage/evaluation which can extend time in clinic.")
48
Allows for more rapid assessment/treatment of large numbers of patients in an “outbreak” scenario (e.g. flu, norovirus) Allows for more patients to be seen than you would have available clinician appointments Allows more complicated patients to be seen by the higher level clinicians in a more timely manner
 Allows for more patients to be seen than you would have available clinician appointments Allows more complicated patients to be seen by the higher level clinicians in a more timely manner.")
Similar presentations





















 Partnership for Quality Education (PQE) Collaborative Interprofessional Team Education Initiative (CITE) Carol.>")


 Patient-Centered Medical Home (PCMH) by the National.>")


>")










