Download presentation
Presentation is loading. Please wait.

1
Questions from Week 9 lecture
Exam content Apraxia/Dyspraxia (disturbance/difficulty) Apraxia Model Differentiating Apraxia/Aphasia Prosopagnosia vs. Variant of Prosopagnosia in Semantic dementia
 Apraxia Model. Differentiating Apraxia/Aphasia. Prosopagnosia vs. Variant of Prosopagnosia in Semantic dementia.")
2
LH lesions destroy motor programs stored in inferior parietal lobe:
In most patients ideomotor apraxia is associated with left hemisphere (LH) lesions LH lesions destroy motor programs stored in inferior parietal lobe: Supramarginal or Angular Gyrus Or disconnect the flow of information from motor programs to premotor or motor areas necessary to initiate complex movement When asked to carry out a command with the right hand this pathway is used To carry out a command with the left hand, information must be carried to the right premotor cortex through Corpus Callosum and then conveyed to motor areas Unilateral (left) apraxia follow lesions located anterior Corpus Callosum
 lesions. LH lesions destroy motor programs stored in inferior parietal lobe: Supramarginal or Angular Gyrus. Or disconnect the flow of information from motor programs to premotor or motor areas necessary to initiate complex movement. When asked to carry out a command with the right hand this pathway is used. To carry out a command with the left hand, information must be carried to the right premotor cortex through Corpus Callosum and then conveyed to motor areas. Unilateral (left) apraxia follow lesions located anterior Corpus Callosum.")
3
Prosopagnosia vs Semantic dementia variant of Prosopagnosia
Lesion: Bilateral occipital vs anterior right temporal Deficit: Faces not categorised as familiar (face recognition units function as a memory store); able to identify facial features; retains knowledge if given person’s name vs progressive difficulty with face recognition/and or naming (semantic knowledge about person is lost)
; able to identify facial features; retains knowledge if given person’s name vs progressive difficulty with face recognition/and or naming (semantic knowledge about person is lost)")
4
Aphasia

5
Aphasia is defined as a loss or impairment of language function caused by brain damage (language content, comprehension, reading and writing) Aphasia/Dysphasia (disturbance/difficulty of language) used interchangeably Language is the complex symbolic signal system used by individuals to communicate with each other Language not only involves the content of speech but communication also occurs by reading and writing Language is intertwined into what it is to be human
 used interchangeably. Language is the complex symbolic signal system used by individuals to communicate with each other. Language not only involves the content of speech but communication also occurs by reading and writing. Language is intertwined into what it is to be human.")
6
Language and Speech production: Speech
Speech is the co-ordinated muscle activity required for oral communication Speech is the neural process involved in language Language is the content of speech Dysarthria Dysarthria is the impairment of the processes involved in speech production (tongue, throat, lips) May include subsystems of respiration, phonation, resonance, prosody (pauses, slow rate) and articulation Dysarthria and aphasia can coexist but one is often seen without the other
 May include subsystems of respiration, phonation, resonance, prosody (pauses, slow rate) and articulation. Dysarthria and aphasia can coexist but one is often seen without the other.")
7
Speech apraxia Disruption of motor program which determines the sequence of muscle contractions required to produce individual sounds and words (multisyllabic words e.g. caterpillar) Difficulty in speaking reflects a lesion that prevents execution (voluntary and on command) of the complex sequence of muscle contractions involved in speaking Manifests primarily as errors in articulation of speech and secondarily what are thought to represent compensatory alterations of prosody Prosody refers to the melody, pauses, intonation stresses/accents that enhance and liven speech Some consider speech apraxia to be a variant of Broca’s aphasia rather than a disorder of speech
 Difficulty in speaking reflects a lesion that prevents execution (voluntary and on command) of the complex sequence of muscle contractions involved in speaking. Manifests primarily as errors in articulation of speech and secondarily what are thought to represent compensatory alterations of prosody. Prosody refers to the melody, pauses, intonation stresses/accents that enhance and liven speech. Some consider speech apraxia to be a variant of Broca’s aphasia rather than a disorder of speech.")
8
Aphasia is a disorder of Language
Dysarthria and Speech Apraxia are disorders of (the motor control) of Speech
 of Speech.")
9
Phonemic Paraphasias – speaking a word with an error in letter sound
Aphasia results from a breakdown in the linguistic components/content of language: Phonemic Paraphasias – speaking a word with an error in letter sound Phonology – term applied to sound pattern of language Phoneme is the smallest segment of spoken language (phoneme = ‘k’ in kiss, ‘p’ in pencil). Sounds/phonemes are ordered to produce words Patients may be impaired in their ability to organise letter sounds in sequence which results in phonemic paraphasias (word is distorted with unintentional sound) An error occurs in a letter sound ‘f’ - ork Real word approximations e.g. pipe = “hike, no, pike, no pipe”; snail for stale Neologisms e.g. fencil for pencil, poot for suit Phonemic decoding critical for language comprehension Necessary to distinguish pear from bear, fit from bit
. Sounds/phonemes are ordered to produce words. Patients may be impaired in their ability to organise letter sounds in sequence which results in phonemic paraphasias (word is distorted with unintentional sound) An error occurs in a letter sound ‘f’ - ork. Real word approximations e.g. pipe = hike, no, pike, no pipe ; snail for stale. Neologisms e.g. fencil for pencil, poot for suit. Phonemic decoding critical for language comprehension. Necessary to distinguish pear from bear, fit from bit.")
10
One word, usually related semantically, replaces another
2. Semantic Paraphasias – speaking an incorrect word semantically related to the target word Semantics – meanings of words e.g. mother, aunt; canary is a small yellow bird Breakdown in understanding referential meaning of words – linking sound to meaning One word, usually related semantically, replaces another Results in semantic paraphasias orange for apple, sister for brother, him for her animal for giraffe Unintended and distinct from word-finding/naming difficulty (e.g. “it’s that green thing you eat with fingers” [asparagus])
")
11
3. Agrammatism/Paragrammatism
Syntax – words strung together to form phrases or sentences in a complex way that obeys grammatical rules A loss of syntactic production results in agrammatism: Broca’s Aphasia Speech is simplified, reduction in prepositions (e.g.“on” ) articles (“the”, “a/an”), inflections - ing, verbs, tense, person, plurals The production of sentences with incorrect use of syntactic elements results in paragrammatism Wernicke’s Aphasia Running or increased speech production, with a tendency to acceleration. Content lacks information-conveying nouns and verbs. Phrases do not make sense together because abnormal syntactic inflections produced or due to paraphasias including neologisms Paragrammatism sometimes called “word salad”
 articles ( the , a/an ), inflections - ing, verbs, tense, person, plurals. The production of sentences with incorrect use of syntactic elements results in paragrammatism. Wernicke’s Aphasia. Running or increased speech production, with a tendency to acceleration. Content lacks information-conveying nouns and verbs. Phrases do not make sense together because abnormal syntactic inflections produced or due to paraphasias including neologisms. Paragrammatism sometimes called word salad")
12
Dementias – rarely cause classical aphasic syndromes
Causes of Aphasia: Neuroanatomical location of lesion rather than the aetiology that essentially determines the nature of the language deficit Focal lesions CVA (stroke) usually middle cerebral artery territory infarct or haemorrhages Abrupt onset Aphasia most pronounced at time of onset – or shortly thereafter Recognisable syndromes usually emerge after acute phase Intracranial tumours and other space occupying lesions (SOL) (cerebral abscess) with symptoms worsening as SOL increases Traumatic brain injury Dementias – rarely cause classical aphasic syndromes Alzheimer’s Disease Frontotemporal lobar degeneration: semantic dementia, progressive non-fluent aphasia
 usually middle cerebral artery territory infarct or haemorrhages. Abrupt onset. Aphasia most pronounced at time of onset – or shortly thereafter. Recognisable syndromes usually emerge after acute phase. Intracranial tumours and other space occupying lesions (SOL) (cerebral abscess) with symptoms worsening as SOL increases. Traumatic brain injury. Dementias – rarely cause classical aphasic syndromes. Alzheimer’s Disease. Frontotemporal lobar degeneration: semantic dementia, progressive non-fluent aphasia.")
13
Mutism: Mutism is a complete failure of language or speech output. May be due to Severe aphasia Acute global aphasia: severely impaired comprehension, reading and writing Acute Broca’s aphasia: comprehension relatively normal, writing may be unaffected An articulation (speech) disorder Aphemia (pure word mutism): comprehension, repetition and reading/writing normal Psychiatric condition
 disorder. Aphemia (pure word mutism): comprehension, repetition and reading/writing normal. Psychiatric condition.")
14
Disorders of articulation:
Causes of mutism: CVA (Stroke) Disorders of articulation: CVA (Stroke, Motor neurone disease, poliomyelitis, Lyme disease, Tumour) Degeneration of the basal ganglia (Huntington’s Disease, Parkinson’s Disease) Psychiatric disorders Catatonia in Schizophrenia, Severe depression and PTSD Hysterical aphonia (Psychogenic voice disorder) Elective mutism
 Disorders of articulation: CVA (Stroke, Motor neurone disease, poliomyelitis, Lyme disease, Tumour) Degeneration of the basal ganglia (Huntington’s Disease, Parkinson’s Disease) Psychiatric disorders. Catatonia in Schizophrenia, Severe depression and PTSD. Hysterical aphonia (Psychogenic voice disorder) Elective mutism.")
15
Left hemisphere and language: the left hemisphere is strongly dominant for language in most humans Language is generally located in the left hemisphere Hemisphere Language Dominance Handedness Left Right Bilateral 50-70% 15-19% 15-20% 96% 4%

16
Classical Aphasic syndromes:
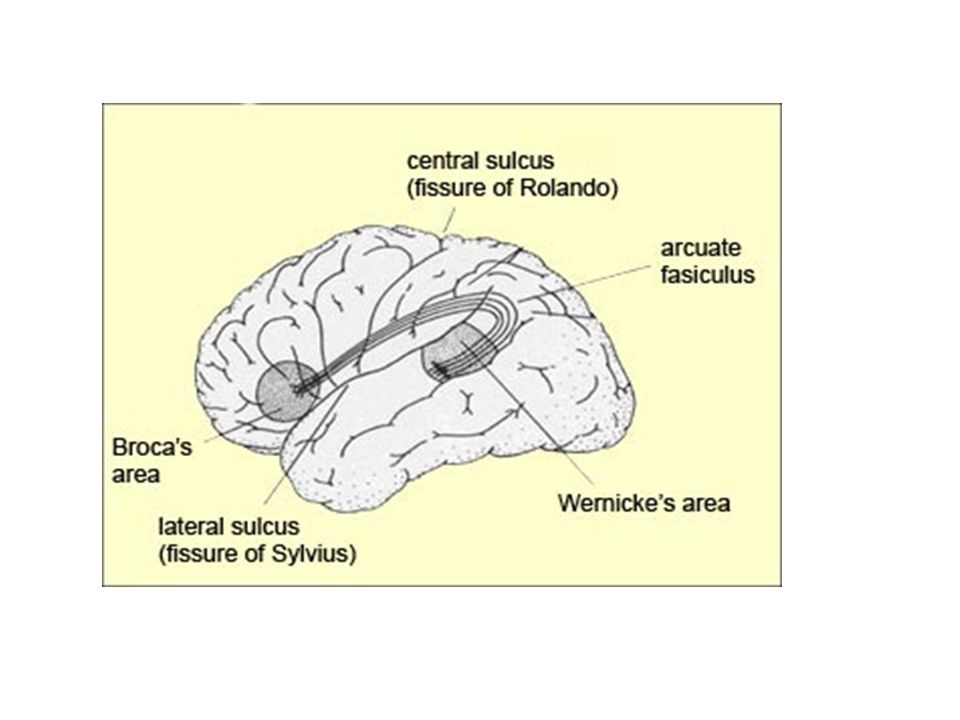
Aphasic syndromes proposed by Lichtheim (1885) drawn from work of Broca and Wernicke Two cortical areas within the dominant (left) hemisphere were identified as having specialised language function Anterior or motor language (Broca’s) area Posterior or sensory language (Wernicke’s) area
 drawn from work of Broca and Wernicke. Two cortical areas within the dominant (left) hemisphere were identified as having specialised language function. Anterior or motor language (Broca’s) area. Posterior or sensory language (Wernicke’s) area.")
17
Anterior or motor language (Broca’s) area
Broca (1861) described a patient “Leborgne” whose language output was non-fluent and limited to the word “tan”. He could understand spoken language, non-verbal communication and could communicate through gestures and facial expression Lesion: center of the lesion was the inferior frontal convolution of left hemisphere Broca related the lesion to the patient’s expressive language dysfunction
 described a patient Leborgne whose language output was non-fluent and limited to the word tan . He could understand spoken language, non-verbal communication and could communicate through gestures and facial expression. Lesion: center of the lesion was the inferior frontal convolution of left hemisphere. Broca related the lesion to the patient’s expressive language dysfunction.")
18
Leborgne’s (Tan’s) brain on autopsy
 brain on autopsy")
19
2. Posterior or sensory language (Wernicke’s) area
Wernicke (1874) described a patient with fluent language output that contained words with sound errors (phonemic paraphasias) and semantic errors, who did not understand spoken language Lesion: posterior part of the superior temporal gyrus Proposed that receptive language processing was localised adjacent to primary “sensory” cortex and expressive language processes was adjacent to primary “motor” cortex.
 described a patient with fluent language output that contained words with sound errors (phonemic paraphasias) and semantic errors, who did not understand spoken language. Lesion: posterior part of the superior temporal gyrus. Proposed that receptive language processing was localised adjacent to primary sensory cortex and expressive language processes was adjacent to primary motor cortex.")
20
Classification of Aphasia Syndromes
Terminology, classification schemes vary Initially dichotomous classification scheme Expressive, non-fluent, motor, anterior or Broca’s aphasia Receptive, fluent, sensory, posterior or Wernicke’s aphasia Lichtheim (1885) developed seven syndromes linked to the lesion sites of Broca and Wernicke: Broca’s aphasia Wernicke’s aphasia Pure motor speech disorder – articulation disorders Pure word deafness – auditory word recognition disorder Transcortical motor aphasia Transcortical sensory aphasia Conduction aphasia
 developed seven syndromes linked to the lesion sites of Broca and Wernicke: Broca’s aphasia. Wernicke’s aphasia. Pure motor speech disorder – articulation disorders. Pure word deafness – auditory word recognition disorder. Transcortical motor aphasia. Transcortical sensory aphasia. Conduction aphasia.")
21
Classification system of lesion based aphasia syndromes
Three additional syndromes described by Benson (1979): Anomic aphasia Global aphasia Isolation of the language zone (Isolated aphasia) Neuroanatomical model developed further by Geschwind (1965) to include the anatomical link between Wernicke’s and Broca’s area – white matter tract “arcuate fasciculus”
: Anomic aphasia. Global aphasia. Isolation of the language zone (Isolated aphasia) Neuroanatomical model developed further by Geschwind (1965) to include the anatomical link between Wernicke’s and Broca’s area – white matter tract arcuate fasciculus")
22
Comprehension Of spoken language: When you hear a word spoken, auditory information is transmitted to the primary auditory cortex and subsequently relayed to Wernicke’s area/inferior parietal lobe in the dominant hemisphere for translation Of written words: Visual impulses transmit to the primary visual cortex in the occipital lobe are relayed to the angular gyrus from which it is sent to Wernicke’s area

23
Expression Following translation the information is passed to Broca’s area via the arcuate fasciculus (subcortical white matter tract) Broca’s area passes information to the primary motor cortex of each hemisphere. Instructions are sent via the motor pathways to the muscles of the speech organs to produce a verbal response

25
Boston Aphasia Classification System
Major Classification System (Benson, 1979) Recognises eight subtypes of aphasia Assess: Boston Diagnostic Aphasia Examination Broca’s Aphasia. Lesion of the expressive speech area Wernicke’s Aphasia. Lesion of the receptive speech area Conduction Aphasia. Disconnection of the expressive and receptive areas Global Aphasia. Extensive lesion involving both expressive and receptive areas
 Recognises eight subtypes of aphasia. Assess: Boston Diagnostic Aphasia Examination. Broca’s Aphasia. Lesion of the expressive speech area. Wernicke’s Aphasia. Lesion of the receptive speech area. Conduction Aphasia. Disconnection of the expressive and receptive areas. Global Aphasia. Extensive lesion involving both expressive and receptive areas.")
26
Boston Aphasia Classification System
5. Transcortical Motor Aphasia 6. Transcortical Sensory Aphasia 7. Isolated Aphasia 8. Anomic Aphasia

27
Boston Aphasia Classification System
Syndromes 1 to 4 Associated with lesion of the central speech areas or their connections Aetiology: Most likely to result from CVA involving one or more of the branches of the middle cerebral artery

28
Boston Aphasia Classification System
Syndromes 5 to 8 Associated with lesions surrounding the central speech areas ‘Watershed’ or ‘Border-zone’ area Aetiology: Infarction between anterior and middle cerebral arteries, and between the middle and posterior cerebral arteries Repetition: Disordered in groups 1 to 4, intact in groups 5 to 8

29
Blood supply: Blue = Anterior Cerebral Artery Pink = Middle Cerebral Artery Yellow = Posterior Cerebral Artery

30
Boston Aphasia Classification System
Each syndrome associated with particular cluster of language symptoms (not all of which need to be present for categorisation) Clusters of certain symptoms have shown discriminant validity between cases of Broca’s, Wernicke’s, conduction and anomic aphasia (Strauss, Sherman & Spreen, 2006) Scale profiles aid in classification but a large range of aphasics patients are not classifiable because they have mixed symptomatology
 Clusters of certain symptoms have shown discriminant validity between cases of Broca’s, Wernicke’s, conduction and anomic aphasia (Strauss, Sherman & Spreen, 2006) Scale profiles aid in classification but a large range of aphasics patients are not classifiable because they have mixed symptomatology.")
31
Some cautions with the lesion based classification systems of aphasia:
1. Level of description of language deficit: Classical syndrome language abnormalities reflect the patients ability to perform entire language tasks (fluent/non-fluent speech, comprehension, repetition, naming) – do not examine the linguistic details of language impairment (phonology, semantics, syntax, prosody). Both Broca’s and Wernicke’s may have problems with expression. 2. Do not cover all patients symptoms: There may be heterogeneity of deficits across patients with the same syndrome (e.g., Broca’s – comprehension of speech may be normal in some, moderately disturbed in others; Benson & Geschwind, 1971) May result in a large number of patients showing mixed rather than pure symptomatology
 – do not examine the linguistic details of language impairment (phonology, semantics, syntax, prosody). Both Broca’s and Wernicke’s may have problems with expression. 2. Do not cover all patients symptoms: There may be heterogeneity of deficits across patients with the same syndrome (e.g., Broca’s – comprehension of speech may be normal in some, moderately disturbed in others; Benson & Geschwind, 1971) May result in a large number of patients showing mixed rather than pure symptomatology.")
32
3. Syndromes may not localise to expected lesion site:
general correlation between lesion site and syndrome classical syndromes are related to lesion sites in cases of rapidly developing lesions e.g., stroke (but not applied to acute and subacute phases of illness) in chronic phase at least 15% of patients have lesions not predictable from their syndromes Broca’s aphasia requires larger lesion to sylvian fissure encompassing much of the left fronto-parietal opercula, insula and white matter in territory upper middle cerebral artery
 in chronic phase at least 15% of patients have lesions not predictable from their syndromes. Broca’s aphasia requires larger lesion to sylvian fissure encompassing much of the left fronto-parietal opercula, insula and white matter in territory upper middle cerebral artery.")
33
Site of damage causing Broca's aphasia
Site of damage causing Broca's aphasia. The areas infarcted in 14 patients, all diagnosed as suffering from Broca's aphasia. All 14 lesions were then superimposed, indicating a focus of damage in the posterior part of the left inferior frontal gyrus. From Kertesz A, Lesk D, McCabe P: Arch Neural 34:590.

34
Site of damage causing Wernicke's aphasia
Site of damage causing Wernicke's aphasia. The areas infarcted in 13 patients, all diagnosed as suffering from Wernicke's aphasia. All 13 lesions were then superimposed, indicating a focus of damage in the posterior part of the left superior temporal gyrus. From Kertesz A, Lesk D, McCabe P: Arch Neurol 34:590.

35
Classifying aphasia syndromes Four aspects of language
1. Fluency Divides syndromes into those associated with anterior (non-fluent) vs posterior (fluent) lesions Non-fluent: slow, laborious, lack of melody/rhythm, poor articulation, shortened phrases, preferred use of verbs and nouns Lesion: anterior to sylvian fissure Fluent: normal rate, preserved rhythm/melody good articulation, normal phrase length Lesion: posterior to sylvian fissure in Wernicke’s area or basal temporal lobe
 vs posterior (fluent) lesions. Non-fluent: slow, laborious, lack of melody/rhythm, poor articulation, shortened phrases, preferred use of verbs and nouns. Lesion: anterior to sylvian fissure. Fluent: normal rate, preserved rhythm/melody good articulation, normal phrase length. Lesion: posterior to sylvian fissure in Wernicke’s area or basal temporal lobe.")
36
2. Repetition Defective repetition:
Lesion: perisylvian area in the territory of the middle cerebral artery, incorporating Broca’s area, insula and Wernicke’s area, and arcuate fasciculus in between them Preserved repetition (cf spontaneous speech): Lesion: sparing of primary language areas (Broca’s and Wernicke’s); lesion is outside of sylvian areas Syndromes associated with sparing of repetition are termed transcortical (transcortical motor or transcortical sensory)
: Lesion: sparing of primary language areas (Broca’s and Wernicke’s); lesion is outside of sylvian areas. Syndromes associated with sparing of repetition are termed transcortical (transcortical motor or transcortical sensory)")
37
Comprehension Deficits on gross examination associated with:
Lesion: Damaged temporal lobe Note** If syntactic comprehension tests are used most dysphasic patients (regardless of site of lesion) will have some comprehension deficit e.g. “Pick up the blue circle OR the red square” (2 step command from the Token Test) “Put the pen on top of the book then give it to me” (3 step command from Western Aphasia Battery)
 will have some comprehension deficit. e.g. Pick up the blue circle OR the red square (2 step command from the Token Test) Put the pen on top of the book then give it to me (3 step command from Western Aphasia Battery)")
38
Naming Ability to name objects, or line drawings is impaired in most aphasic patients to some degree 3 30. harmonica…… (musical instrument) Copied from Boston Naming Test for educational purposes
 Copied from Boston Naming Test for educational purposes.")
39
Broca’s Aphasia Non-fluent speech Impaired repetition Comprehension relatively intact Naming poor – improves with phonemic cues, and multiple choice Speech: - Slow and effortful; phonemic paraphasias Agrammatic and telegrammatic (containing a predominance of content words) Writing: - Misspellings, letter omissions, perseverations, agrammatic sentences - Copying better than to dictation
 Writing: - Misspellings, letter omissions, perseverations, agrammatic sentences. - Copying better than to dictation.")
40
Reading: - Reading aloud poor - Comprehension relatively spared Frequent Associations - Speech apraxia - Dysarthria - Right Hemiplegia (paralysis) or hemiparesis (weakness) – most notable in the arm and face Ideomotor apraxia Neuropathology Extensive damage to fronto-parietal region to area supplied by anterior branch of middle cerebral artery Evolves over time from global aphasia
 or hemiparesis (weakness) – most notable in the arm and face. Ideomotor apraxia. Neuropathology. Extensive damage to fronto-parietal region to area supplied by anterior branch of middle cerebral artery. Evolves over time from global aphasia.")
41
Spontaneous Language: ‘Cookie jar theft’: Boston Diagnostic Aphasia Examination
Copied for educational purposes

42
youtube.com broca’s aphasia

43
2. Wernicke’s Aphasia Fluent speech Repetition poor Comprehension impaired Naming impaired – not aided by phonemic cues or multiple choice Speech: - Content: Word substitutions (phonemic and semantic paraphasias) and combinations, sometimes neologistic jargon Incapable of monitoring own output Sentences meaningless and cannot be understood by others Writing: - Legible – letters formed (rarely have a concomitant hemiplegia) - Content: Aphasic, disjointed, repetitive text, few nouns and verbs
 and combinations, sometimes neologistic jargon. Incapable of monitoring own output. Sentences meaningless and cannot be understood by others. Writing: - Legible – letters formed (rarely have a concomitant hemiplegia) - Content: Aphasic, disjointed, repetitive text, few nouns and verbs.")
44
Reading: Reading aloud and reading comprehension both disturbed (occasional patients may have superior reading ability) Associated deficits: - Often none - Visual field defect - Quadrantanopia may be evident Neuropathology Destruction of Wernicke’s area Damage to superior posterior temporal lobe

46
youtube Wernicke’s aphasia

47
3. Conduction Aphasia Fluent speech paraphasic (mainly phonemic) Repetition highly abnormal – strings of phonemic approximations Comprehension relatively intact Naming often disturbed Speech: Hesitation due to word finding difficulties (dysprodic speech) - Writing: - Spelling poor with omission, reversal and substitution of letters - Words often interchanged and misplaced
 - Writing: - Spelling poor with omission, reversal and substitution of letters. - Words often interchanged and misplaced.")
48
Reading: Reading aloud similar to repetition highly abnormal Silent reading may be good Frequent Associations: - Often none - Hemianesthesia (loss of sensation down one side of the body) - Visual field defects (hemianopia or quadrantanopia) Neuropathology: - Severing of the arcuate fasciculus in classical syndrome - More commonly results supramarginal gyrus lesion - Conduction aphasia often occurs in recovery from Wernicke’s aphasia
 - Visual field defects (hemianopia or quadrantanopia) Neuropathology: - Severing of the arcuate fasciculus in classical syndrome. - More commonly results supramarginal gyrus lesion. - Conduction aphasia often occurs in recovery from Wernicke’s aphasia.")
49
4. Transcortical Aphasias
Early aphasiologists postulated a transcortical pathway linking auditory language and verbal motor centre bypassing meaning – now used descriptively 4a) Transcortical Motor Aphasia Shares many qualities with Broca’s aphasia Non-fluent speech: reduction in the quality and complexity of spontaneous speech (non-fluent) and dysarthric Few paraphasic errors Repetition: preserved Comprehension: very good Writing: similar to spoken output Lesions: dominant frontal lobe anterior and superior to Broca’s area generally due to anterior cerebral artery infarction
 Transcortical Motor Aphasia. Shares many qualities with Broca’s aphasia. Non-fluent speech: reduction in the quality and complexity of spontaneous speech (non-fluent) and dysarthric. Few paraphasic errors. Repetition: preserved. Comprehension: very good. Writing: similar to spoken output. Lesions: dominant frontal lobe anterior and superior to Broca’s area generally due to anterior cerebral artery infarction.")
50
4b) Transcortical Sensory Aphasia
similar to Wernicke’s aphasia Fluent speech: contaminated by semantic paraphasias Comprehension: defective at level of linking sound to meaning Repetition: words and long sentences intact but cannot extract meaning from language Reading and writing: similar to Wernicke’s aphasia (disturbed) Lesion: border zone of parieto-temporal junction
 Lesion: border zone of parieto-temporal junction.")
51
5. Anomic Aphasia - Anomia (the inability to name to confrontation) common to most aphasic patients - When most prominent feature of the aphasia the condition is referred to as anomic aphasia - Common syndrome - Often the end point of recovery from other aphasic conditions Speech - Fluent but empty due to lack of substantive words May be circumlocutory (providing a description of the word) or abrupt cut-offs (trying to find word) in mid sentence Writing: Near Normal Neuropathology:- Non-localising; Acute onset suggests lesion temporo-parietal area
 or abrupt cut-offs (trying to find word) in mid sentence. Writing: Near Normal. Neuropathology:- Non-localising; Acute onset suggests lesion temporo-parietal area.")
52
6. Global (total) Aphasia
All major language functions seriously disturbed Neuropathology: Typically extensive left hemisphere damage Syndrome has been reported even in cases where Wernicke’s area is spared May result from subcortical syndromes which functionally isolate Broca’s area

53
7. Isolation (mixed-transcortical) Aphasia
- Rare - Intact repetition in association with marked reduction of spontaneous speech and poor comprehension - Voluntary aspects of language lost (spontaneous speech, initiation of speech) - Resembles global aphasia except for preservation of repetition Neuropathology: Anterior and posterior parts of watershed area
 - Resembles global aphasia except for preservation of repetition. Neuropathology: Anterior and posterior parts of watershed area.")
54
Tests of Language: Spontaneous language: Confrontation naming:
Open questions (Western Aphasia Battery) How are you? Have you been here before? Tell me a little about whyy ou are here? Complex picture description: ‘cookie jar theft’ picture from Boston Diagnostic Aphasia Examination Confrontation naming: line-drawings (Boston Naming Test)
 How are you Have you been here before Tell me a little about whyy ou are here Complex picture description: ‘cookie jar theft’ picture from Boston Diagnostic Aphasia Examination. Confrontation naming: line-drawings (Boston Naming Test)")
55
Word-picture matching tests:
Comprehension: Increasingly syntactically complex commands one step, two step, three step commands Token Test, Western Aphasia Battery) Word-picture matching tests: single-word (semantic) comprehension (Peabody Picture Vocabulary Test) Aphasia batteries: Boston Diagnostic Aphasia Examination Western Aphasia Battery Psycholinguistic Assessment of Language Processing in Aphasia (PALPA)
 Word-picture matching tests: single-word (semantic) comprehension (Peabody Picture Vocabulary Test) Aphasia batteries: Boston Diagnostic Aphasia Examination. Western Aphasia Battery. Psycholinguistic Assessment of Language Processing in Aphasia (PALPA)")
Similar presentations



 Ling 411 – 05.>")



>")











