Download presentation
Presentation is loading. Please wait.

1
Hammering Skills in Assessment of the Elderly: Falls and Cognition— Who to Screen, How to Treat? John M Carment, MD, FACP ACP OK Chapter Scientific Meeting September 26, 2014

2
Disclosure I have no financial relationships with any entity producing, marketing, re-selling, or distributing health care goods or services consumed by, or used on, patients. John Carment, MD, FACP john-carment@ouhsc.edu Assistant Professor of Geriatrics NE Region Clinical Director, OHAI

4
Objectives Utilize case scenarios for examining best practice with respect to falls and dementia Recognize the risk factors for falls Implement evidence-based interventions to reduce falls Discuss clinically efficient means of addressing cognitive impairment in elders

5
Case 1 76-year-old woman with is seen for her semi-annual visit wrote “increased forgetfulness” on the line for her concerns today You note that the ROS checkbox for “falls in the last year” is checked PMHx: Osteoporosis, HTN and OA left knee Meds: Lisinopril, alendronate, metoprolol and acetaminophen

6
Which statement has the best supporting evidence for a clinical practice guideline? A. Adults aged > 75 yrs should be screened for dementia biannually B. Adults who fall should be screened for osteoporosis C. The MMSE should be administered annually to geriatric patients D. Adults aged> 70 should be screened for falls annually

7
Which guideline is best? A. Dementia screen biannually B. Osteoporosis screen in fallers C. Annual MMSE D. Annual fall screen

8
USPSTF does not support generalized dementia screening Brief screening measures have only fair specificity Current treatments are symptomatic with modest effect Unclear whether benefit outweighs harm www.ahrq.gov/clinic/uspstf/uspsdeme.htm

9
Case 1 Discussion The Medicare Annual Wellness Visit does require “screening” for cognition Does not require use of a specific instrument MMSE score alone does not diagnose dementia Screening criteria for osteoporosis is not inclusive of those older adults who have falls

10
USPSTF recommends annual screening for falls Ask all patients > 70 years old about falls and balance or gait difficulties annually Observe patients walking and getting into/out of a chair Further assessment for all those with two or more falls or balance/gait impairment AGS, BGS, AAOS Panel on Falls Prevention. J Am Geriatr Soc 2010.

11
Case 2 88-year-old male is seen for several recent falls after discharge from a skilled nursing facility. He had been hospitalized the previous month for pneumonia. PMHx: Parkinson’s disease, BPH, OA bil knees Meds: Carbidopa/levodopa, tamsulosin, and hydrocodone/acetaminophen.

12
Which risk factor most strongly predicts future falls? A. Cognitive impairment B. Lower extremity weakness C. Use of assistive device D. Visual impairment

13
Which risk factor is highest for falls ? A. Cognitive impairment B. Lower extremity weakness C. Use of assistive device D. Visual impairment

14
Risk Factors Across Multiple Observational Studies Lower extremity weakness (RR 4.4) Balance & gait impairment (RR 2.9) Use of assistive device (RR 2.6) Visual impairment (RR 2.5) Tinetti ME, NEJM 2003; 348:42-49. Arthritis (RR 2.4) Depressive symptoms (RR 2.2) Cognitive impairment (RR 1.9) Use of four or more medications Age > 80 yrs AGS, BGS, AAOS Panel on Falls Prevention. J Am Geriatr Soc 2001; 49:664-72.
 Depressive symptoms (RR 2.2) Cognitive impairment (RR 1.9) Use of four or more medications Age > 80 yrs AGS, BGS, AAOS Panel on Falls Prevention. J Am Geriatr Soc 2001; 49:")
15
USPSTF focus on 4 factors Age History of falls History of mobility problems Poor performance on the timed Get Up and Go Test http://www.uspreventiveservicestaskforce.org/uspstf11/fallsprevention/

16
Timed “ Up and Go ” Test Simple test of observing a person stand up from a chair (without use of arms), walk 10 feet, turn around, walk back, and sit down again. Normal person takes < 10 seconds when timed > 16 seconds is considered positive > 20 seconds are at risk of falls outside their homes Sensitivity 54-87%; Specificity 74-87% for falls Posiadlo et al, J Am Geriatr Soc. 1991; 39:142-148

17
RCT evidence best supports which treatment option(s) to reduce fall risk? A. Referral for PT or exercise therapy B. Prescribing vitamin D C. Adaptation or modification of the home environment D. All of the above

18
RCT evidence-based treatment to reduce fall risk ? A. PT referral / Exercise therapy B. Vit D Rx C. Home environment modifications D. All of above

19
Interventions Proven in RCTs Muscle-strengthening and balance re- training Treatment with Vitamin D Even if levels are normal Home hazard evaluation Tai Chi Gradual withdrawal of psychotropic meds Multidisciplinary geriatric assessment Cochrane Database Syst Review 2009

20
Evidence-based programs, such as: o Chronic Disease Self Management Program o REACH (Resources for Enhancing Alzheimer’s Caregiver Health) o Eat Better, Move More o Tai Chi: Moving for Better Balance o Diabetes Self Management Program Annual themes, such as: o Medication Management o Physical Activity o Diabetes o Healthy Brain, Healthy Mind Education Center Activity Education Center Activity
 o Eat Better, Move More o Tai Chi: Moving for Better Balance o Diabetes Self Management Program Annual themes, such as: o Medication Management o Physical Activity o Diabetes o Healthy Brain, Healthy Mind Education Center Activity Education Center Activity")
21
USPSTF recommends “Grade B” Provide intervention consisting of exercise or physical therapy and/or vitamin D supplementation. Group classes, at-home physiotherapy Vit D median dose 800 IU/day, median duration 12 months http://www.uspreventiveservicestaskforce.org/uspstf11/fallsprevention/

22
USPSTF recommends against “Grade C” In-depth multifactorial risk assessment and comprehensive management to prevent falls for all community-dwelling adults aged 65 years and older Small benefit is found, but not applicable to heterogeneous population of all older persons. http://www.uspreventiveservicestaskforce.org/uspstf11/fallsprevention/

23
Most effective components Most effective components of a multifactorial risk assessment and comprehensive management approach Evaluation of balance and mobility Vision assessment Orthostatic blood pressure measurement Review of medications Home environment assessment AGS, BGS, AAOS Panel on Falls Prevention. J Am Geriatr Soc 2010.

24
Case 3 An 81-year-old female is seen for increasing memory loss and difficulty managing changes in her warfarin dosing. The anticoagulation nurse was concerned as she is increasing out of therapeutic range. PMHx: Afib, depression, urge incontinence, osteoporosis Meds: Warfarin alternating 2.5 mg and 5 mg,atenolol, oxybutnin, sertraline, raloxifene

25
What is the most efficient approach to evaluate her cognitive status ? A. Folstein Mini-Mental Status Examination B. Montreal Cognitive Assessment C. St. Louis Univ Mental Status (SLUMS) Exam D. Collateral historian to determine functional independence with IADLs
 Exam D. Collateral historian to determine functional independence with IADLs.")
26
Most efficient approach? A. MMSE B. MOCA C. SLUMS D. Collateral Hx for IADLs

27
DSM-V Criteria for Dementia Significant cognitive impairment in at least one of the following: Learning and memory Complex attention Language Perception-motor function Executive function Social cognition DSM-V. 1 st ed. American Psychiatric Assoc. 2013.

28
DSM-V Criteria for Dementia Acquired and decline from previous level Must interfere with independence in everyday activities Not delirium or better accounted for by a different mental disorder DSM-V. 1 st ed. American Psychiatric Assoc. 2013.

29
Clinical Evaluation for Dementia Critical to have a knowledgeable informant Explore IADLs (medication managment, driving, finances, shopping) as early indicators of functional loss
 as early indicators of functional loss")
30
Clinical Evaluation for Dementia Abnormal cognitive test scores alone do not diagnose dementia Mild cognitive impairment No benefit from cognition-enhancing medications unless fulfills criteria for dementia

31
Efficient Evaluation for Dementia Take clinical history on first visit, perform cognitive testing and physical exam at following visit MMSE or Mini-Cog if suspect dementia based in multiple IADL impairment Prefer MOCA, SLUMS, or neuropsychological testing if daily function is mostly preserved

32
Montreal Cognitive Assessment (MOCA) Validated tool sensitive for detecting MCI Condensed neuropsychological testing Requires 10-15 min to administer Limited for visually/hearing impaired persons Freely available in 31 languages at www.mocatest.org Nasreddine et al. J Am Geriatr Soc. 2005; 53: 695-99

35
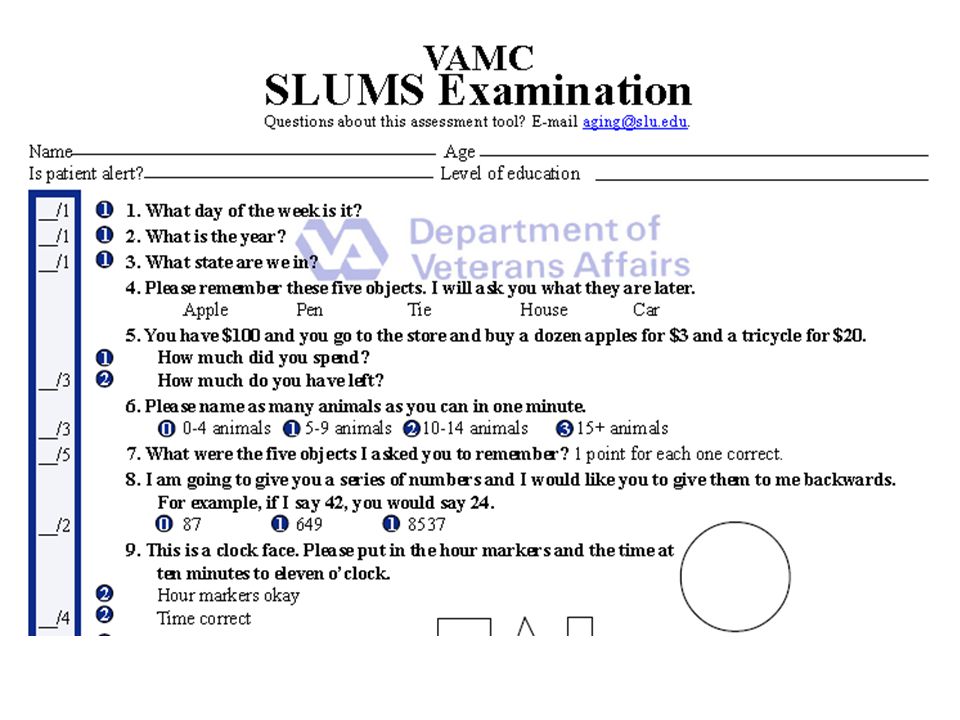
St. Louis Univ Mental Status Exam (SLUMS) 30-point battery similar format to MMSE Enhanced immediate/delayed recall, animal naming, attention, numeric calculation, recall of facts from a paragraph Sensitivity and specificity for dementia were equal to MMSE in a pilot study of 702 veterans Tariq SH et al. Am J Geriatr Psych. 2006; 19: 600-10
 30-point battery similar format to MMSE Enhanced immediate/delayed recall, animal naming, attention, numeric calculation, recall of facts from a paragraph Sensitivity and specificity for dementia were equal to MMSE in a pilot study of 702 veterans Tariq SH et al. Am J Geriatr Psych. 2006; 19:")
38
Visual or dexterity limitations Blessed Memory Test "John Brown, 42 Market Street, Chicago, Illinois" and One-minute animal fluency (normal > 11) Combination has similar sensitivity and specificity to the MMSE for dementia
 Combination has similar sensitivity and specificity to the MMSE for dementia")
39
Conclusions Screen annually for falls, don’t screen for dementia Add the following to your toolbox Timed “Get up and go” test PT/Exercise + Vitamin D +/- Home Safety Eval Know your local resources for seniors Use IADL impairment to guide cognitive screen test selection

40
Questions John Carment, MD, FACP john-carment@ouhsc.edu

Similar presentations










 Richard M. Dubinsky, MD; Anthony C. Stein, PhD; and Kelly Lyons,>")

 Training Program>")



: The Role of Cognitive Assessment in Improving Health Outcomes Dr. William Mansbach October 25, 2011.>")






