Download presentation
Presentation is loading. Please wait.

1
Common Tropical Infections Siriluck Anunnatsiri, MD Infectious Disease & Tropical Medicine Department of Medicine Khon Kaen University

2
Tropical Infections: Definition Infectious diseases that either occur uniquely or more commonly in tropical and subtropical regions, are either more widespread in the tropics or more difficult to prevent or control.

3
Tropical and Subtropical Regions 23 0 35 0

4
Common Tropical Infectious Diseases in Thailand Leptospirosis Rickettsioses: Scrub typhus Murine typhus Melioidosis Enteric fever Typhoid fever Paratyphoid fever Nontyphoidal salmonellosis Tuberculosis Malaria Dengue infection Helminthic infection Infective diarrhea

5
Leptospirosis The most widespread zoonosis in the world Situation in Thailand สำนักระบาดวิทยา กรมควบคุมโรค กระทรวงสาธารณสุข

6
Pathogenic Leptospira spp. Lancet Infect Dis 2003; 3: 758 88% 7.5% 2.5% 1% each

7
Saprophytic Leptospira species SpeciesSerovarReference strain Serogroup Genomospecies 3hollandWaz Holland (P438) Holland L. biflexapatocPatoc ISemaranga L. wolbachiicodiceCDC Lancet Infect Dis 2003; 3: 758

8
Reservoir hosts of common leptospiral serovar Lancet Infect Dis 2003; 3: 758

9
Risk factors for exposure to leptospires Occupational groups Farmers, ranchers, abattoir workers, trappers, veterinarians, loggers, sewer workers, rice-field workers, military personnel Recreational activities Freshwater swimming, canoeing, kayaking, trail biking, hunting Household environment Pet dogs, domesticated livestock, rainwater catchment systems, rodent infestation

10
Pathogenesis Route of transmission: Abrasion & cuts in skin Mucous membrane/Conjunctiva Intact skin after prolong immersion in water Inhalation of aerosol/water Ingestion Toxin production: LPS Hemolysin Cytotoxin Outer envelope: Antiphagocytic component Outer membrane protein: Interstitial nephritis Immune complex mediated inflammation: Interstitial nephritis Vasculitis

11
Clinical manifestations Anicteric leptospirosisIcteric leptospirosis Weil’s syndrome (Incubation period 2-20 days) Fever Leptospiremic phase 3-7 days Immune phase 0-30 days Leptospiremic phase 3-7 days Immune phase 0-30 days Associated symptoms Myalgia Headache Nausea, Vomiting Abdominal pain Conjunctival suffusion Meningitis Uveitis Rash Jaundice Hemorrhage Acute renal failure Myocarditis Hemorrhagic pneumonitis Meningoencephalitis Hypotension Leptospires present in Blood CSF Urine
 Fever Leptospiremic phase 3-7 days Immune phase 0-30 days Leptospiremic phase 3-7 days Immune phase 0-30 days Associated symptoms Myalgia Headache Nausea, Vomiting Abdominal pain Conjunctival suffusion Meningitis Uveitis Rash Jaundice Hemorrhage Acute renal failure Myocarditis Hemorrhagic pneumonitis Meningoencephalitis Hypotension Leptospires present in Blood CSF Urine")
12
Clinical manifestations Lancet Infect Dis 2003; 3: 758

13
Laboratory diagnosis Culture Antibody detection Screening test MSAT, IHA, IFA, LA, ELISA, LEPTO dipstick Confirmation test Microscopic agglutination test Antigen detection Polymerase chain reaction (PCR) Pathology
 Pathology")
14
Treatment Mild form Doxycycline Amoxicillin Erythromycin Moderate-to-severe form Penicillin G Doxycycline Ceftriaxone Supportive & Symptomatic Treatment Antimicrobial therapy

15
Prevention Protective clothing, rodent control, preventing recreation exposure Chemoprophylaxis Doxycycline 200 mg once a week Vaccine Animal Human – 2 developing vaccines but no license vaccine approval in human use

16
Rickettsioses Scrub typhus Orientia tsutsugamushi Vector: Trombiculid mite (chigger): Leptothrombidium spp. Murine typhus Rickettsia typhi Vector: Xenopsylla cheopsis Spotted fever rickettsioses R. helvetica, R. honei, R. felis, R. conorii Vectors: Ticks www.eco-pestcontrol.com

17
Distribution of scrub typhus in Asia Redrawn from Harwood and James (1979)
")
19
Life cycle of murine typhus

20
Pathogenesis of rickettsioses Vector bites and feeds and regurgitate bacteria into skin bite site. Bacteria are carried via lymphatics/small blood vessels to general circulation where they invade endothelial cells (primary target) Spread to contiguous endothelial cells, smooth muscle cells, and phagocytes http://pathmicro.med.sc.edu/mayer/ricketsia.htm Spread via the microcirculation and invade all organ systems Vasculitis resulting in local thrombus formation and end organ damage.
 Spread to contiguous endothelial cells, smooth muscle cells, and phagocytes Spread via the microcirculation and invade all organ systems Vasculitis resulting in local thrombus formation and end organ damage..")
21
Clinical presentations Fever Myalgia Headache Nausea/vomiting Abdominal pain Diarrhea Conjunctival suffusion / subconjunctival hemorrhage Lymphadenopathy Rash Hepatomegaly Splenomegaly Jaundice Altered consciousness Seizure Hypotension

22
Clinical presentations

23
Laboratory diagnosis Culture Antibody detection Weil-Felix test: OX-K for scrub typhus OX-19 for murine typhus Latex agglutination test, dot-blot ELISA Confirmation tests: IFA, IIP Polymerase chain reaction (PCR) Pathology
 Pathology")
24
Treatment Scrub typhus Doxycycline Chloramphenicol Rifampicin Azithromycin Murine typhus Doxycycline Chloramphenicol

25
Melioidosis Burkholderia pseudomallei Risk factors Diabetes mellitus Thalassemia Preexisting renal diseases Chronic liver diseases Immunosuppressive use Transmission Direct inoculation Inhalation Ingestion, sexual contact (rare)
")
26
Worldwide distribution of melioidosis

27
Melioidosis: Clinical classification Disseminated septicemic melioidosis Non-disseminated septicemic melioidosis Multifocal localized melioidosis Localized melioidosis Probable melioidosis Subclinical melioidosis

28
Clinical presentations of melioidosis Clinical presentations % of patients in: Royal Darwin Hospital; n=252 Infectious Diseases Association of Thailand; n=686 Srinagarind Hospital; n=100 Pneumonia584549 Bacteremia465759 Hepatosplenic abscess 6952 Skin&soft tissue infection 171623 Genitourinary tract infection 19713 Bone&joint infection 4527 Neurological melioidosis 43NR Pericardial effusion 13NR

29
Clinical presentations Lancet 2003; 361: 1720

30
Laboratory diagnosis Culture – Gold standard Antibody detection IHA,ELISA, immunochromatographic test, dot immunoassay, Gold-blot immunoassay Antigen detection ELISA, latex agglutination, IFA Polymerase chain reaction

31
Treatment Acute phase Ceftazidime + co- trimoxazole Cefoperazone/sulbactam + co-trimoxazole Imipenem/Meropenem Co-amoxiclav Maintenance phase Co-trimoxazole + doxycycline Co-amoxiclav Ciprofloxacin + azithromycin At least 10-14 daysAt least 20 weeks

32
Enteric fever Typhoid fever Salmonella Typhi Paratyphoid fever Salmonella Paratyphi A, B, and C สำนักระบาดวิทยา กรมควบคุมโรค กระทรวงสาธารณสุข

33
Pathogenesis www.netterimages.com

34
Symptoms of enteric fever SymptomsTyphoid fever (%)Paratyphoid fever (%) Fever89-10092-100 Headache43-9060-100 Nausea23-3633-58 Vomiting24-3522-45 Abdominal cramp 8-5229-92 Diarrhea30-5717-68 Constipation10-792-29 Cough11-3610-68
Paratyphoid fever (%) Fever Headache Nausea Vomiting Abdominal cramp Diarrhea Constipation Cough")
35
Signs of enteric fever SymptomsTyphoid fever (%)Paratyphoid fever (%) Abdominal tenderness 33-846-29 Splenomegaly23-650-74 Hepatomegaly15-5216-32 Relative bradycardia 17-5011-100 Rose spots2-460-3 Rales & rhonchi 8-842-87 Epitaxis1-212-13 Meningism1-120-3
Paratyphoid fever (%) Abdominal tenderness Splenomegaly Hepatomegaly Relative bradycardia Rose spots Rales & rhonchi Epitaxis Meningism")
37
Laboratory diagnosis Culture – Gold standard: Blood, BM, duodenal string test Antibody detection Widal test – poor sensitivity & specificity Rapid serological diagnostic test Lancet 2005; 366: 754

38
Drug resistance S. Typhi 1990-2004 Lancet 2005; 366: 752

39
Treatment Lancet 2005; 366: 755

40
Prevention Lancet 2005; 366: 757 Safe water & food, personal hygiene, appropriate sanitation Vaccination Vi polysaccharide vaccine, Ty21a vaccine, Vi conjugate vaccine

41
Malaria 4 human Plasmodium sp. pathogens P. falciparumP. vivax P. ovaleP. malariae Vector: Anopheles sp. สำนักระบาดวิทยา กรมควบคุมโรค กระทรวงสาธารณสุข

43
Malaria: Life Cycle http://www.cdc.gov

44
Clinical outcome of malarial infection Nature 2002; 415: 673-679.

45
Pathogenesis of P. falciparum Nature 2002; 415: 673-679.

46
Uncomplicated malaria Signs and symptoms of malaria: non-specific Fever Chills Headache Myalgia Sore throat Anorexia Anemia Hepatosplenomegaly

47
WHO criteria for severe malaria Cerebral malaria Impaired of consciousness (GCS <11) Severe anemia (Hct <20% or Hb <7 g/dl) Hypoglycemia (BS <40 mg/dl) Metabolic acidosis (HCO 3 <15 mmol/L) Acute renal failure (Cr >3 mg/dl and urine output <400 ml/day) Acute pulmonary edema and ARDS Shock Abnormal bleeding Jaundice (TB >2.5 mg/dl) Hemoglobinuria Hyperparasitemia ( infection rate >5%) WHO. Trans R Soc Trop Med Hyg 2000; 94 (Suppl).
..")
48
Laboratory diagnosis Thick and thin film blood smear – Gold standard Antigen detection by rapid dipstick immunochromatographic assays Histidine-rich protein-2: P. falciparum Parasite-specific LDH: All Plasmodium spp. PCR technique

49
Plasmodium falciparum

50
Plasmodium vivax

51
Plasmodium malariae

52
Plasmodium ovale

54
Antimalarial treatment: Uncomplicated falciparum malaria or mixed infection DrugsDosesDuration (days) Artemether (20) – lumefantrine (120) <15 kg: 1 tab BID 16-25 kg: 2 tabs BID 26-35 kg: 3 tabs BID >35 kg: 4 tabs BID 3 Atovaquone (250) – proguanil (100) 20 mg/kg/day 8 mg/kg/day 3 Quinine SO 4 + Tetracycline or Doxycycline Clindamycin 10 mg/kg TID 4 mg/kg QID 2 mg/kg BID 5 mg/kg TID 7 Artesunate + Mefloquine 4 mg/kg/day 15 mg/kg 10 mg/kg 3 2 nd day of Rx 3 rd day of Rx
 Artemether (20) – lumefantrine (120) <15 kg: 1 tab BID kg: 2 tabs BID kg: 3 tabs BID >35 kg: 4 tabs BID 3 Atovaquone (250) – proguanil (100) 20 mg/kg/day 8 mg/kg/day 3 Quinine SO 4 + Tetracycline or Doxycycline Clindamycin 10 mg/kg TID 4 mg/kg QID 2 mg/kg BID 5 mg/kg TID 7 Artesunate + Mefloquine 4 mg/kg/day 15 mg/kg 10 mg/kg 3 2 nd day of Rx 3 rd day of Rx")
55
Antimalarial treatment: Severe malaria or Uncomplicated malaria with parasitemia >4% IRBC Artesunate i.v. 2.4 mg/kg at hour 0 and 12 followed by 2.4 mg/kg daily until oral medication is tolerated. Continue oral drug 2 mg/kg daily until day 7, adding 2 nd agent as for quinine (below) Quinine HCl i.v. 20 mg/kg given over 4 hours, then 10 mg/kg every 8 hours. A second drug, e.g. doxycycline, tetramycin, or clindamycin for 7 days; or atovaquone + proguanil for 3 days, should be added when the patient can tolerate oral medication.
 Quinine HCl i.v. 20 mg/kg given over 4 hours, then 10 mg/kg every 8 hours. A second drug, e.g. doxycycline, tetramycin, or clindamycin for 7 days; or atovaquone + proguanil for 3 days, should be added when the patient can tolerate oral medication..")
56
Antimalarial treatment: Non-falciparum malaria Chloroquine 600 mg base at hour 0 followed by 300 mg base at hour 6, 2 nd day, and 3 rd day of treatment + Primaquine (for P. vivax and P. ovale only) 0.3-0.6 mg base/kg daily for 14 days
 mg base/kg daily for 14 days.")
57
Prevention Vector control Insecticide spraying Larva control Personal protection Insecticide-treated bednets Insect repellents Wearing appropriate clothing Antimalarial chemoprophylaxis “Stand-by” emergency treatment

Similar presentations



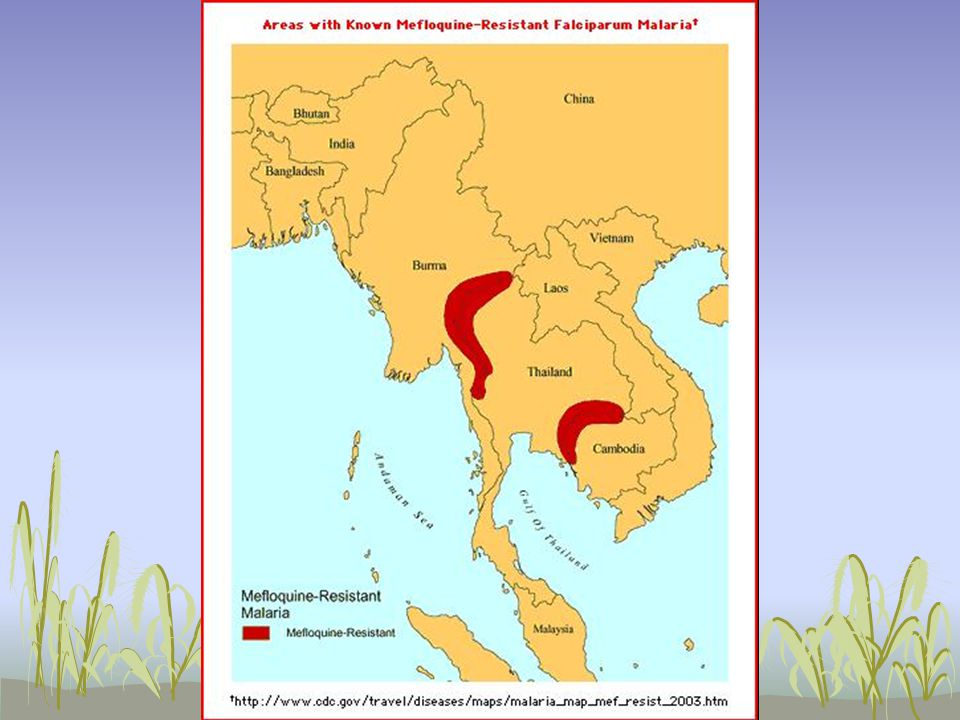













 Symptoms and Diagnosis Treatment Preventive measures Where malaria occurs in the world.>")






