Download presentation
Presentation is loading. Please wait.

1
Teaching Case of the Week Dr. W. A. Ciccotelli Sept 14, 2005

2
The Patient 82 y M Past Hx Low grade B cell lymphoma Pancytopenia/transfusion dependent Interstitial lung dz HTN Ex-smoker

3
The Patient Meds Amlodipine Prednisone (taperingx 4 mos) NKDA 2-4x EtOH/wk
 NKDA 2-4x EtOH/wk")
4
The Case Referred to ID for peri-orbital cellulitis 3 day Hx of progressive R eye swelling R frontal headache Reactive clear discharge FB sensation No fever/chills No other ocular symptoms Vision ok On cefotaxime 36 hrs

5
The Case Afebrile, VSS Peri-orbital cellulitis R eye proptosis, mild ptosis, chemosis Loss of EOM R eye CNs normal otherwise Visual acuity normal

6
The Case WBC 4.9, Hgb 99, plts 54, grans 1.7 Lytes N Cr 123 TSH 1.1 Panculture neg CXR: unchanged chronic interstitial pattern

7
The Case CT scan head R pre-septal edema Minimal proptosis R eye R Maxillary & ethmoidal sinusitis R nasal septum deviation No bony lesions No retro-orbital masses ENT consulted

9
The Case Not responding on Cefotaxime Febrile New diplopia Worsening peri-orbital cellulitis

10
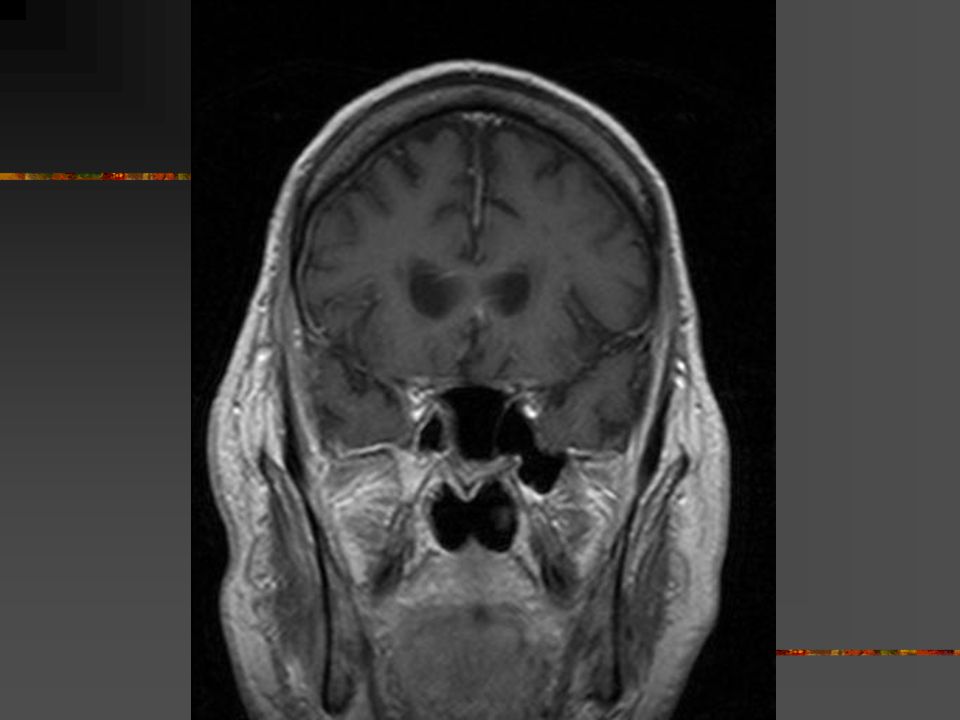
The Case Abx changed to Clinda/Cipro MRI head Small fluid collection lat. R eye ?abscess Maxillary & ethmoid sinusitis (L & R) Meninges inflammatory changes in R middle cranial fossa No cavernous vein thrombosis Nasal culture: commensal flora
 Meninges inflammatory changes in R middle cranial fossa No cavernous vein thrombosis Nasal culture: commensal flora.")
13
The Case Now really bad! Delirious Febrile Clonus in lower ext. R Facial droop

14
The Case Urgent ethmoidectomy necrotic sinus painless procedure LP aseptic meningitis ANCAs neg Lipo Ampho B started 5 mg/kg/day

15
The Case Repeat MRI Early cerebritis R temporal operculum Ongoing inflammatory changes of all sinuses Inflammatory changes around R orbit, masticator space, cavernous sinus

18
Case Resolution Further CNS deterioration Sinus Bx Broad ribbon like non-septate fungal filament on microscopy ZN & PAS stains confirm non-septate hyphae Dx of Rhinocerebral zygomycosis Lipo Ampho B to 10 mg/kg/day Family withdrew care given degree of surgery needed

19
Zygomycosis Mucorales order Ubiquitous in environment Thick walled non-septate hyphae with right angle branching Rare & mimics other invasive mould infections Inherent resistance to antifungal agents Angioinvasive disease

20
Zygomycosis Multiple clinical forms Cutaneous Pulmonary Gastrointestinal Rhinocerebral Sino-orbital Disseminated Direct inoculation, inhalation, ingestion of spores

21
Zygomycosis Immunocompromised state hallmarks DM ketoacidosis Neutropenia Chemotherapy BMT patients Lymphoma/leukemia Trauma with exposure to contaminated soil

22
Zygomycosis Dx is difficult & delayed Poor recovery from culture Non specific presentation Not on everyone’s DDx Mimics other invasive molds (Aspergillus) Dx generally made with invasive testing for histopathological sampling Dx commonly made at autopsy Yet increasingly problematic in Heme-Onc patients over 1990s
 Dx generally made with invasive testing for histopathological sampling Dx commonly made at autopsy Yet increasingly problematic in Heme-Onc patients over 1990s")
23
Zygomycosis Treatment is multifaceted Immune reconstitution Aggressive surgical debridement Ampho B Prayer Posaconazole as oral alternative Despite this still highly fatal (mortality 50- 80%)
")
24
Zygomycosis Prognosis is poor Late Dx Not able to recover immune system Disseminated Death usually from hemorrhage Best prognosis Limited disease Early surgery Non Heme-Onc patients

25
Zygomycosis Tip offs Right patient population (esp neutropenia) Unexplained thrombosis Necrotic eschar Unexplained hemorrhage Common clinical situations Culture neg despite real disease Not responsing to reasonable Abx
 Unexplained thrombosis Necrotic eschar Unexplained hemorrhage Common clinical situations Culture neg despite real disease Not responsing to reasonable Abx")
Similar presentations







 Intracranial (15-20%) Bony (5-10%) Radiography – Computed tomography (CT) best for.>")
 – herpes simplex virus Murakami (1996) 11/14.>")













>")
