Download presentation
Presentation is loading. Please wait.

1
Infertility He-Feng Huang Women’s Hospital, School of Medicine, Zhejiang University

2
Where we come from?

4
Infertility Definition: The inability to achieve pregnancy after regular unprotected intercourse for a period of 1 year. Primary infertility: never conceived within 1 year Secondary infertility: after a previous pregnancy, unable to conceive again within a 1 year period.

5
Etiology Female factors Male factors Female and male factors

6
Female Factor Ovulatory disorders Tubal factors Uterine factors Cervical factors Vulval and vaginal factors

7
Ovulatory disorders Hypothalamic dysfunction Pituitary dysfunction Ovarian factor Others Hypothalamic-pituitary- ovary axis

8
Hypothalamic dysfunction Psychological factors: Stress, Disturbance, Anorexia derived from mental stimulus Chronic consumptive diseases: Tuberculosis, Severe malnutrition, Anorexia nervosa

9
Pituitary dysfunction Pituitary tumors: Pituitary adenoma Pituitary lesions: Empty sella syndrome Sheehan’s Syndrome

10
Ovarian factors PCOS LUFS POF Ovary insensitivity syndrome Congenital abnormality Surgery or X-ray Ovarian endometriosis Ovarian tumor

11
PCOS Symptom Menses disturbance and infertility hirsutism, acne, obesity ( BMI ≥ 25 ) Diagnosis ( 1 ) irregular menses or anovulation ( 2 ) experimental or clinical hyperandrogenism ( 3 ) polycystic ovarian morphology observed by ultrasound Accord with 2 points of the three. Follow-up for whole life

12
Others Thyroid disorder Adrenal dysfunction

13
Tubal factors Inflammation Surgery of ectopic pregnancy Tubal ovarian effusion Ectopic pregnancy Tubal blockage, hydrosalpinx (HSG )
")
14
Tubal ligation Tubal abnormality Tubal factors Tubal ligation Tuberculosis fallopian tube

15
Increase of tubal factors STD Repeated intro-uterine manipulation Repeated drug abortion

16
Uterine factors Uterine developmental abnormality Congenital absence of the uterus Uterine malformation Endometrial abnormality Endometrial tuberculosis Asherman syndrome Uterine tumor

17
Uterine developmental abnormality

18
Intrauterine adhesions fibroid

19
Male factors Semen abnormality Oligospremia, Aspermia, Asthenospermia Sperm transport abnormality Endocrine disorders Sexual dysfunction Immunological factors

21
Male and female factors Psychological factors Subfertility Immunological factors

22
Classification

23
Investigation and Diagnosis Male investigation History: general health, medications, lifestyle and reproductive health General examination Specific examination : abnormality of genitals seminal analysis

24
Volume ≥ 2.0ml PH 7.2~7.5 Density ≥ 20×10 /ml Count ≥ 40×10 /every ejaculation ≥ 50% sperm progressive motility (grade a+b) or ≥ 25% sperm rapid progressive motility (grade a) Grade a: rapid progressive motility Grade b: slow progressive motility Morphology ≥ 15% Survive rate ≥ 58% WBC ≤ 1×10 6 6 6 Normal Seminal analysis ( Fourth/Fifth version ) Volume ≥ 1.5ml PH 7.2~7.5 Density ≥ 15×10 /ml Count ≥ 39×10 /every ejaculation ≥ 32% sperm progressive motility (grade a+b) Grade a: rapid progressive motility Grade b: slow progressive motility Morphology ≥ 4% Survive rate ≥ 50% WBC ≤ 1×10 6 6 6 Fourth versionFifth version
 or ≥ 25% sperm rapid progressive motility (grade a) Grade a: rapid progressive motility Grade b: slow progressive motility Morphology ≥ 15% Survive rate ≥ 58% WBC ≤ 1× Normal Seminal analysis ( Fourth/Fifth version ) Volume ≥ 1.5ml PH 7.2~7.5 Density ≥ 15×10 /ml Count ≥ 39×10 /every ejaculation ≥ 32% sperm progressive motility (grade a+b) Grade a: rapid progressive motility Grade b: slow progressive motility Morphology ≥ 4% Survive rate ≥ 50% WBC ≤ 1× Fourth versionFifth version")
25
Female Investigation History General examination Specific examination Others

26
Specific examination Ovarian examination Ovulation monitor Luteal function Ovarian reserve

27
Ovarian function Ovulation monitor 1 、 Basic body temperature 2 、 Cervical mucus 3 、 Vaginal cytological test 4 、 Ultrasound monitor 5 、 Serum or urinary LH peak 6 、 Serum E 2 and P levels 7 、 Endometrial biopsy 8 、 Laparoscopy

28
Follicular development and ovulation

29
Biphasic basal body temperature

30
monophasic basal body temperature

31
Low estrogenHigh estrogen

32
Cervical mucus

33
Fern crystallization

34
Proliferative endometriumSecretory endometrium

36
Luteal function 1 、 BBT 2 、 Endometrial biopsy 3 、 Serum E2 and P levels

37
Ovarian reserve 1 、 Age 2 、 Antral follicle count (AFC) 3 、 Basic FSH 、 E2 4 、 CC stimulating test 5 、 GnRH-a stimulating test 6 、 AMH 、 Inhibin B
 3 、 Basic FSH 、 E2 4 、 CC stimulating test 5 、 GnRH-a stimulating test 6 、 AMH 、 Inhibin B")
38
Tubal investigation Hydrotubation Hysterosalpinography (HSG) Laparoscopy Hysterosalpingography by Ultrasound
 Laparoscopy Hysterosalpingography by Ultrasound")
39
Hydrotubation

40
HSG normal figure

41
Laparoscopy : methylene blue liquid

42
Postcoital test Cervical hostility Hysteroscope Laparoscopy

43
Postcoital test

44
Cervical hostility Hysteroscope Laparoscopy

45
Cervical hostility

46
Postcoital test Cervical hostility Hysteroscope Laparoscopy

47
Endometriosis ( Endometriosis ( Laparoscopy)
")
48
Treatment of infertility 1.Treatment of genitals organic disease 2.Induction of ovulation 3.Luteal support 4. Improvement of cervical mucus 5.Treatment of tubal inflammation 6.ART

49
1. Genitals organic disease Genital malformations Genital inflammation Uterine Myoma Endometriosis ----Etiology combined treatment: Infection control, Surgery

50
2.Tubal infertility Fallopian tube obstraction: Fallopian tube glue loose solution operation Salpingostomy Tubo-uterine implantation Tubal anastomosis Fallopian tubes were partial unobstructed: Liquid instillation Physical therapy Traditional Chinese Medicine

51
3. Asherman syndrome Principle of Management: Separate adhesions Prevention of adhesion recurrence Promote endometrium repair Methods Hysteroscope management of intrauterine adhesion Estrogen promote endometrium regeneration Intrauterine device (IUD)
.")
52
1.Reproduction-related disease 2.Induction of ovulation 3.Luteal support 4.Improvement of cervical mucus 5.Treatment of tubal inflammation 6.ART

53
Drugs for ovulation induction CC HMG FSH: u-FSH, FSH-HP, r-FSH HCG GnRH ( LHRH ) GnRH analog : GnRH agonist GnRH antagonist bromocriptine
 GnRH analog : GnRH agonist GnRH antagonist bromocriptine")
54
The first R-GN ( Gonal- F+Lhadi+Ovidrel=FSH+LH+HCG ) IVFbaby—Sebastian ( 1997.5.7 )
 IVFbaby—Sebastian ( )")
55
1.Reproduction-related disease 2.Induction of ovulation 3.Luteal support 4. Improvement of cervical mucus 5.Treatment of tubal inflammation 6.ART

56
1.Reproduction-related disease 2.Induction of ovulation 3.Luteal support 4. Improvement of cervical mucus 5.Treatment of tubal inflammation 6.ART

57
1.Reproduction-related disease 2.Induction of ovulation 3.Luteal support 4. Improvement of cervical mucus 5.Treatment of tubal inflammation 6.ART

58
1.Reproduction-related disease 2.Induction of ovulation 3.Luteal support 4. Improvement of cervical mucus 5.treatment of tubal inflammation 6.ART

59
Summary: Infertility-treatment Azoospermia Genetic disease After surgery Assisted Reproductive Technologies (ART) Unexplained Causes Treatment Anovulation Induction of ovulation Tubal factor Tuboplasty Anatomic factor Microsurgery Immunologic Medication or surgery Immune inhibition
 Unexplained Causes Treatment Anovulation Induction of ovulation Tubal factor Tuboplasty Anatomic factor Microsurgery Immunologic Medication or surgery Immune inhibition")
60
ART Assisted Reproductive technology AID or AIH Artificial insemination IVF-ET In vitro fertilization-embryo transfer

61
AIH or AID AIH (artificial insemination with husband sperm) IUI (Intrauterine insemination ) IVI (Intravaginal insemination) ICI (Intracervical insemination) ITI (Intratubal insemination) IPI (Intraperitoneal insemination) IFI (Intrafollicle insemination) AID (artificial insemination by donor)
 IUI (Intrauterine insemination ) IVI (Intravaginal insemination) ICI (Intracervical insemination) ITI (Intratubal insemination) IPI (Intraperitoneal insemination) IFI (Intrafollicle insemination) AID (artificial insemination by donor)")
62
IVF-ET Indication Tubal infertility Endometriosis IUI failure Unexplained infertility Immunological infertility Oligospermia

63
IVF-ET

65
Other technology derived from IVF Crypreservation of embryos Oocyte donation and embryo donation Surrogate mother GIFT (Gamete intrafallopian transfer) ZIFT (Zygote intrafallopian transfer) ICSI PGD
 ZIFT (Zygote intrafallopian transfer) ICSI PGD")
66
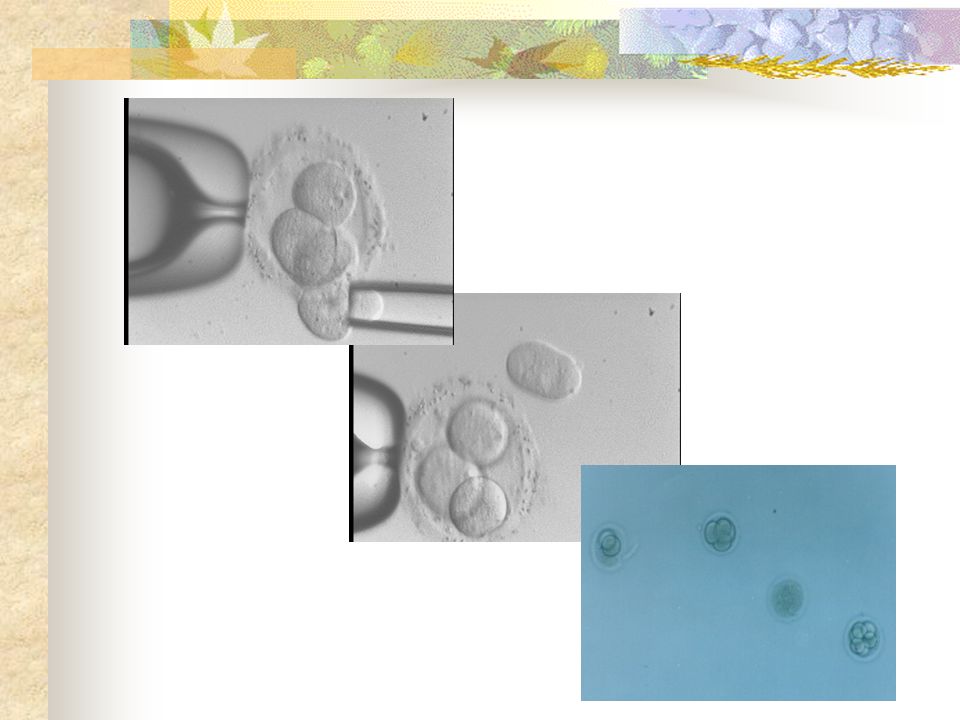
ICSI (Intracytoplasmic sperm injection)
")
68
PGD Preimplantation genetic diagnosis

69
PGD indication ★ X-linked chromosome disease ★ Chromosome abnormality (number/structure) ★ Monogenic diseases PGS: Preimplantation genetic screen Advanced age History of habitual abortion Failure of IVF for several times
 ★ Monogenic diseases PGS: Preimplantation genetic screen Advanced age History of habitual abortion Failure of IVF for several times")
70
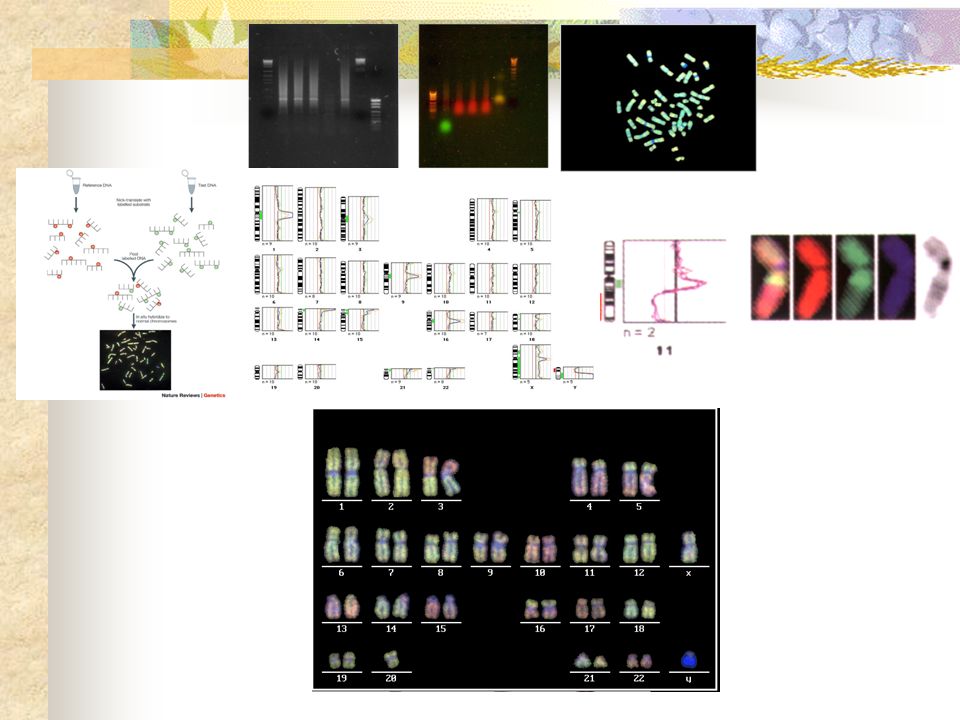
PGD technique Blastomere Biopsy FISH Single cell PCR Interphase nuclear conversion Whole genomic amplification,WGA Comparative genomic hybridization, CGH

71
PGD

73
14 三体 正常 14 三体, 13 单体 Robertsonian translocation ( 13q14q )
")
74
X-linked agammaglobulinemia

76
IVF-ET protocol Patients preparation COH Oocyte retrieval In vitro fertilization Embryo trasfer Luteal support Follow up

78
Complication of ART OHSS Ectopic pregnancy and abortion Multiple pregnancy - multiple pregnancy reduction

79
Transvaginal ultrasound-guided selective fetal reduction

80
In vitro maturation (IVM) Immature oocytes Mature oocytes embryos
 Immature oocytes Mature oocytes embryos")
81
Ethic of ART (Chinese government) The government does not support nor approve the practice of human clones Forbid performing ART for single woman Forbid Manufacturing Oocytes Forbid commercial trial of zygotes and embryos Forbid multiple pregnancy dominated ART Forbid gender selected ART without medical indication Forbid surrogate motherhood
 The government does not support nor approve the practice of human clones Forbid performing ART for single woman Forbid Manufacturing Oocytes Forbid commercial trial of zygotes and embryos Forbid multiple pregnancy dominated ART Forbid gender selected ART without medical indication Forbid surrogate motherhood")
82
Ethic of ART Challenge the course of natural reproduction Danger of inbreeding Commercial trial of zygotes and embryos Uncertainty of parenthood Risk of oocyte donation Controversy between clone and traditional family formation Clone criminality Challenge of the definition of “human” ART related regulations and laws

Similar presentations








 Fertility –Ability.>")



>")
 AIH (artificial insemination by husband) AID (artificial insemination by donor) IUI (intrauterine.>")












 Intercourse (Timed)4 (Follicle Monitoring) 1 IUI6 ---do---- CC6 ---do---- CC+IUI8 2 FSH / HMG7.7 CC / FSH /IUI9-12.>")