Download presentation
Presentation is loading. Please wait.

2
Ergonomics Interventions: What Works… And How? As Seen By: Richard Wells Research Team: Wells RP 1,2, Cole DC 2, 3,, Norman RW 1, Frazer MB 1, Theberge N. 1,5, Kerr MS 2,4 (1) Department of Kinesiology, University of Waterloo, Waterloo, ON, Canada, (2) Institute for Work and Health, Toronto, ON, Canada, (3) Department of Public Health Sciences, University of Toronto, Toronto, ON, Canada, (4) School of Nursing, Faculty of Health Sciences, University of Western Ontario, London, ON, Canada (5) Department of Sociology, University of Waterloo, Waterloo, ON, Canada,
 Department of Kinesiology, University of Waterloo, Waterloo, ON, Canada, (2) Institute for Work and Health, Toronto, ON, Canada, (3) Department of Public Health Sciences, University of Toronto, Toronto, ON, Canada, (4) School of Nursing, Faculty of Health Sciences, University of Western Ontario, London, ON, Canada (5) Department of Sociology, University of Waterloo, Waterloo, ON, Canada,.")
3
Story #1 XXX, a metal furniture manufacturing company, established an ergonomics program that cut lost workdays from work-related musculoskeletal disorders from 176 in 1991 to 0 in 1997. Ergonomic changes increased productivity 25%. Source: CTD News

4
How are we to interpret this story? What exactly was changed? Were there no co-interventions? Did these change(s) improve the musculoskeletal symptoms Did these change(s) reduce exposures substantially? Are the change(s) and success generalizeable?
 improve the musculoskeletal symptoms Did these change(s) reduce exposures substantially. Are the change(s) and success generalizeable .")
5
Story #2 : Ergonomics Intervention in a Small Company A small company had two low back compensation ”cases” in a department with heavy lifting within one year. Powered lifting assists were introduced as an engineering intervention. One year later no reduction in the costs associated with back claims was found. Conclusion: The intervention was a failure… The original conclusion was not correct Feedback from supervisors and workers determined that: people in the were not familiar with the use of the lift assists and didn’t use them. breakdowns meant that they were not available much of the time. These process measures indicated that both the intensity of the intervention and compliance were low. A review of the specifications of the lift assists and in efficacy tests (in the laboratory), the assists reduced low back loads for the weights of interest. Upon review of the cost data it was determined that most of the costs were due to an injury which occurred in the previous year. Cost data were also deemed to be unstable due to the small size of the company and the limited follow up time
, the assists reduced low back loads for the weights of interest. Upon review of the cost data it was determined that most of the costs were due to an injury which occurred in the previous year. Cost data were also deemed to be unstable due to the small size of the company and the limited follow up time.")
6
The Need for “Evidence” Workplace parties have faced conflicting messages: The validity of workplace-based evaluations of ergonomic interventions has been questioned in both scientific and public forums due to: research design quantitative vs qualitative methods inadequate reporting of uncontrolled co-interventions and limited consideration of them in analysis and interpretation poor descriptions of populations, exposures and interventions inadequate accounting for the timing or impact of interventions. inadequate accounting of outcomes But what is good evidence?

7
Evidence?

8
Evidence?

9
Evidence?

10
Evidence? Review of 35 Health Promotion Intervention Studies Heamy & Goetzel. Am J Health Promot 1997; 11:290-307 (adopted from TS Kristensen, EPICOH 2001, Copenhagen) Slide courtesy of Hilkka Riihimäki Results Design NEncouragingMixedDiscouraging No comparison11100 % 0 % 0 % group Non-randomized16 56 %31 %13 % comparison group Randomized 922 %56 %22 % comparison group
 Slide courtesy of Hilkka Riihimäki Results Design NEncouragingMixedDiscouraging No comparison11100 % 0 % 0 % group Non-randomized16 56 %31 %13 % comparison group Randomized 922 %56 %22 % comparison group.")
11
Point of View Interventions Health Outcomes Interventions OR Health Work Disability Cost Avoidance Production Exposure Culture Work as a complex, open system

12
How Can We Do Better? Maximise the change in exposure, using, as appropriate: Best science on risk factors and mechanisms Macro ergonomic perspective Production system level interventions Participatory change processes Evaluate a range of leading to lagging indicators to assess critical modifiers and road blocks and to improve

13
Approach for Evaluation of an Ergonomics Intervention for Reducing WMSD 0: Societal, Medico-legal, business and compensation climate 1: Management/ workforce attitudes to changing the work environment 2: Workplace changes 3: Change in exposure 4: Changes in Pain/Discomfort/ Symptoms 5: Reporting of Pain and Discomfort 6: Disability at Work 7: Costs of Disability LAGGING LEADING Cole, Wells et al., Methodological issues in evaluating workplace interventions to reduce work- related musculoskeletal disorders through mechanical exposure reduction, IWH Working Paper #190. 2003

14
Story #3: An Example of an Intervention An automotive parts company had concerns about increasing back and shoulder problems on a line. Automotive Tier 1 supplier of molded foam assemblies for impact protection Process involves extracting, cleaning and re-waxing molds (tools) moving around a closed track (conveyance system) then trimming, inspecting and packing the parts Parts mass up to 1kg
 moving around a closed track (conveyance system) then trimming, inspecting and packing the parts Parts mass up to 1kg.")
15
Design: Quasi-Experimental; Non-Randomized Control Groups 1999 2000 2001 2002 2003 2004 Auto: Foam Plant A1 Plant A2 Plant B Plant C Plant D Courier: Plant E Plant F Manufacturing: Plant G Plant H InterventionFollow-up Control Follow-up Intervention Follow-up Control Follow-up } } } } InterventionFollow-up ControlFollow-up Intervention Follow-up Control Follow-up WSIB 98-0008WSIB 01-041?HealNET Pre I Legend Evaluation Questionnaire Field Measures Intervention Control

16
Evaluation of Ergonomic Interventions Targeting Exposure for Reducing WMSD LEADING 0: Societal, Medico-legal, business and compensation climate 1: Management/ workforce attitudes to changing the work environment 2: Workplace changes 3: Change in exposure 4: Changes in Pain/Discomfort 5: Reporting of Pain and Discomfort 6: Disability at Work 7: Costs of Disability Conditions Pathway and Modifiers Measures Corporate OH+S policy, culture and practice Management/labour relations LAGGING

17
Evaluation of the Case Study Within one province, these factors are similar evaluation not performed These companies are self- selecting and wish to change evaluation not performed

18
Evaluation of Ergonomic Interventions Targeting Exposure for Reducing WMSD LEADING LAGGING 0: Societal, Medico-legal, business and compensation climate 1: Management/ workforce attitudes to changing the work environment 2: Workplace changes 3: Change in exposure 4: Changes in Pain/Discomfort 5: Reporting of Pain and Discomfort 6: Disability at Work 7: Costs of Disability Conditions Pathway and Modifiers Measures Type of changes Engineering Administrative Personal/ behavioral modifiers Number of changes Resources Commitment to change Management competence

19
Evaluation of the Case Study Handle cutout on boxes New trim tools Aluminum scrapers EZ Lift-assist devices Wire scrap racks Sit/stand stools Hammer stamp Vacuum de-mould device Green rack lid holder Box flap holder Blower to break seal Air pop-its Divider racks Redesigned counter table New trim tables New packing racks Ergonomics Change board Upper body support Changes to line layout Feedback board Improved wax The team implemented a total of 21 changes during the 9 month project:

20
Evaluation of Ergonomic Interventions Targeting Exposure for Reducing WMSD LEADING LAGGING 0: Societal, Medico-legal, business and compensation climate 1: Management/ workforce attitudes to changing the work environment 2: Workplace changes 3: Change in exposure 4: Changes in Pain/Discomfort 5: Reporting of Pain and Discomfort 6: Disability at Work 7: Costs of Disability Conditions Pathway and Modifiers Measures Individual and system level exposure: self report observation technical measures Type Intensity Compliance Ergonomic quality of interventions

21
Evaluation of the Case Study Mechanical exposure had been lowered when evaluated at a change specific level.

22
Evaluation of the Case Study Mechanical exposure had been lowered when evaluated at a change specific level. New Trim Tools Evaluation Results: Worker Ratings of Effort Across Trim Tools 0 1 2 3 4 5 6 7 8 9 10 ShoulderElbow to Hand Exertion Scale Contest Winner Green Handle No Handle Time Required to Complete Trimming Task 0 2 4 6 8 10 12 14 16 18 Green HandleContest WinnerNo Handle Time (min.) High Effort Low Effort Better Worse Better Worse Worker felt the tools with handles were easier on shoulders/arms. Increased Forearm ‘Muscle Recovery Time’ for tools with handles. Task was completed faster using Trim tools with handles. Lower (better) muscle activity for tools with handles (curve further left). 'Recovery Time' of Wrist Muscles 0 1 2 3 4 5 6 7 8 9 Wrist ExtensorWrist Flexor Gaptime (secs/min.) Contest Winner Green Handle No Handle # EMG gaps in forearm muscles Extensors Flexors Contest Winner Runner-up Previous
 High Effort Low Effort Better Worse Better Worse Worker felt the tools with handles were easier on shoulders/arms. Increased Forearm ‘Muscle Recovery Time’ for tools with handles. Task was completed faster using Trim tools with handles. Lower (better) muscle activity for tools with handles (curve further left). Recovery Time of Wrist Muscles Wrist ExtensorWrist Flexor Gaptime (secs/min.) Contest Winner Green Handle No Handle # EMG gaps in forearm muscles Extensors Flexors Contest Winner Runner-up Previous.")
23
Evaluation of the Case Study Mechanical exposure had been lowered when evaluated at a change specific level.

24
Evaluation of the Case Study: Evaluation of Change Intensity Time-weighted impact evaluation of the Packing Protocol change with relative APDF 0.5 values for the dominant trapezius as the dependent measure. In each case the original methods were assigned a relative value of 100%. Laing, 2002

25
Evaluation of the Case Study: Evaluation of Change Intensity Impact evaluation of the platform change with on LBPRI. LBPRI = Low Back Pain Reporting Index, Norman et al., 1998, Kerr et al, 2001, Laing, 2002

26
Evaluation of Ergonomic Interventions Targeting Exposure for Reducing WMSD LEADING LAGGING 0: Societal, Medico-legal, business and compensation climate 1: Management/ workforce attitudes to changing the work environment 2: Workplace changes 3: Change in exposure 4: Changes in Pain/Discomfort 5: Reporting of Pain and Discomfort 6: Disability at Work 7: Costs of Disability Conditions Pathway and Modifiers Measures Self- report pain and discomfort symptoms Time delay Distribution of WMSD symptoms Psychosocial Factors

27
Evaluation of the Case Study Despite higher initial physical job demands, the Intervention Line workers underwent a smaller increase in pain than did the Comparison Line workers.

28
Evaluation of Ergonomic Interventions Targeting Mechanical Exposure for Reducing WMSD LEADING LAGGING 0: Societal, Medico-legal, business and compensation climate 1: Management/ workforce attitudes to changing the work environment 2: Workplace changes 3: Change in exposure 4: Changes in Pain/Discomfort 5: Reporting of Pain and Discomfort 6: Disability at Work 7: Costs of Disability Conditions Pathway and Modifiers Measures First-aid log (OSHA log) Medical visits/first aid Workplace Psychosocial Factors, e.g. Control Attribution Level of pain/discomfort Absolute exposure Filter Effects

29
Evaluation of Ergonomic Interventions Targeting Mechanical Exposure for Reducing WMSD LEADING LAGGING 0: Societal, Medico-legal, business and compensation climate 1: Management/ workforce attitudes to changing the work environment 2: Workplace changes 3: Change in exposure 4: Changes in Pain/Discomfort 5: Reporting of Pain and Discomfort 6: Disability at Work 7: Costs of Disability Conditions Pathway and Modifiers Measures Work Disability Scales Work Role Function DASH WCB (No) Lost-Time Claims Psychosocial Factors e.g. Control Return To Work Program Physiotherapy on-site Reactive workplace changes

30
Evaluation of Ergonomic Interventions Targeting Exposure for Reducing WMSD Not considered LEADING LAGGING 0: Societal, Medico-legal, business and compensation climate 1: Management/ workforce attitudes to changing the work environment 2: Workplace changes 3: Change in (mechanical) exposure 4: Changes in Pain/Discomfort 5: Reporting of Pain and Discomfort 6: Disability at Work 7: Costs of Disability Conditions Pathway and Modifiers Measures WCB Claim costs Sickness Absence costs Indirect Costs including replacement, retraining, etc Psychosocial Factors Return To Work Program Physiotherapy on-site Reactive workplace changes
 exposure 4: Changes in Pain/Discomfort 5: Reporting of Pain and Discomfort 6: Disability at Work 7: Costs of Disability Conditions Pathway and Modifiers Measures WCB Claim costs Sickness Absence costs Indirect Costs including replacement, retraining, etc Psychosocial Factors Return To Work Program Physiotherapy on-site Reactive workplace changes")
31
Evaluation of Ergonomic Interventions Targeting Exposure for Reducing WMSD LEADING LAGGING 0: Societal, Medico-legal, business and compensation climate 1: Management/ workforce attitudes to changing the work environment 2: Workplace changes 3: Change in (mechanical) exposure 4: Changes in Pain/Discomfort 5: Reporting of Pain and Discomfort 6: Disability at Work 7: Costs of Disability Conditions Pathway and Modifiers Measures Conclusion: The intervention did not progress identifiably past this point after 9 months of team activity Yes Small Effect Small Effect?
 exposure 4: Changes in Pain/Discomfort 5: Reporting of Pain and Discomfort 6: Disability at Work 7: Costs of Disability Conditions Pathway and Modifiers Measures Conclusion: The intervention did not progress identifiably past this point after 9 months of team activity Yes Small Effect Small Effect")
32
Issues “Reportable Injuries” and Costs should not be the only measures of the success of ergonomic interventions due to the considerable variation in the manner of: collection, classification systems, routinization of aggregation, and transparency of reporting,

33
Step Up Ladies and Gentlemen to the Circus Midway and Try Your Luck at the Gopher Game also known as “Lower Your WMSD Injury Costs” Caution: Your mileage may differ!

34
$ Lost Time Claims No-Lost Time Claims Modified DaysSickness/Absence Insurance $ Lost Time Injuries Too High? Surcharges Possible? Reduce Those Lost Time Costs!

35
$ Lost Time Claims Modified DaysSickness/Absence Insurance $ No-Lost Time Claims No-Lost Time Injuries Too High? Reduce Those No-Lost Time Costs

36
Lost Time Claims No-Lost Time Claims Modified DaysSickness/Absence Insurance $ Too Many Modified Duties? Reduce Overtime and Replacement Worker Costs

37
Our View on What Works… 0: Societal, Medico-legal, business and compensation climate 1: Management/ workforce attitudes to changing the work environment 2: Workplace changes 3: Change in exposure 4: Changes in Pain/Discomfort/ Symptoms 5: Reporting of Pain and Discomfort 6: Disability at Work 7: Costs of Disability } Beware Filter Effects } Ergonomics } “Culture”

38
What we need… A range of indicators at different levels, leading to lagging, to: Advance the methodology in Ergonomic Intervention Research Help organizations audit and improve their own interventions

39
Ergonomics Programs? Tackling work-related WMSDs: Success factors 1 The use of prevention-focused interventions at the organizational level. These are more sustainable than rehabilitation or individual – level interventions. 2 Interventions should reflect a holistic, organizational approach 3 A sound risk assessment is vital for the design of ergonomic interventions 4 Commitment, involvement, and support from top management are crucial 5 Training and advice should always be provided 6 Evaluation is essential to ascertain the sustainability of efforts 7 Research evidence can be used to identify and share good practice 8 Constructive partnerships at all levels are important for coordination of efforts. What is risk assessment for work-related WMSDs? Risk assessment is designed to help employers and employees deal with ergonomic risks in an evidence based but user-friendly manner. It involves: 1 Assessment of risks 2 Design of interventions 3 Implementation and monitoring of interventions 4 Evaluation and reassessment

40
Ergonomics Program? Tackling work-related stress: Success factors 1 The use of prevention-focused interventions at the organizational level. These are more sustainable than rehabilitation or individual – level interventions. 2 Interventions should reflect a holistic, organizational approach 3 A sound risk assessment is vital for the design of stress interventions 4 Commitment, involvement, and support from top management are crucial 5 Training and advice should always be provided 6 Evaluation is essential to ascertain the sustainability of efforts 7 Research evidence can be used to identify and share good practice 8 Constructive partnerships at all levels are important for coordination of efforts. What is risk assessment for work-related stress Risk assessment is designed to help employers and employees deal with psychosocial risks in an evidence based but user-friendly manner. It involves: 1 Assessment of risks 2 Design of interventions 3 Implementation and monitoring of interventions 4 Evaluation and reassessment

41
Ergonomics Program? No… a Stress Program Report on Workshop 1: Work- related stress, in: Preventing Psychosocial risks at Work: European perspectives, Forum, European Agency for Safety and Health at Work, 9, pp4-5, (2003) Tackling work-related stress: Success factors 1 The use of prevention-focused interventions at the organizational level. These are more sustainable than rehabilitation or individual – level interventions. 2 Interventions should reflect a holistic, organizational approach 3 A sound risk assessment is vital for the design of stress interventions 4 Commitment, involvement, and support from top management are crucial 5 Training and advice should always be provided 6 Evaluation is essential to ascertain the sustainability of efforts 7 Research evidence can be used to identify and share good practice 8 Constructive partnerships at all levels are important for coordination of efforts. What is risk assessment for work-related stress Risk assessment is designed to help employers and employees deal with psychosocial risks in an evidence based but user-friendly manner. It involves: 1 Assessment of risks 2 Design of interventions 3 Implementation and monitoring of interventions 4 Evaluation and reassessment
 Tackling work-related stress: Success factors 1 The use of prevention-focused interventions at the organizational level. These are more sustainable than rehabilitation or individual – level interventions. 2 Interventions should reflect a holistic, organizational approach 3 A sound risk assessment is vital for the design of stress interventions 4 Commitment, involvement, and support from top management are crucial 5 Training and advice should always be provided 6 Evaluation is essential to ascertain the sustainability of efforts 7 Research evidence can be used to identify and share good practice 8 Constructive partnerships at all levels are important for coordination of efforts. What is risk assessment for work-related stress Risk assessment is designed to help employers and employees deal with psychosocial risks in an evidence based but user-friendly manner. It involves: 1 Assessment of risks 2 Design of interventions 3 Implementation and monitoring of interventions 4 Evaluation and reassessment.")
42
What we need… Integration of ergonomic intervention research into a broader healthy and productive workplaces approach

43
Supported by: HealNET Ontario Workplace Safety and Insurance Board The people, corporations, and unions that have made this program of Research at Work successful www.iwh.on.cawww.iwh.on.ca www.ergonomics.uwaterloo.ca/bprint.htmlwww.ergonomics.uwaterloo.ca/bprint.html wells@uwaterloo.ca

45
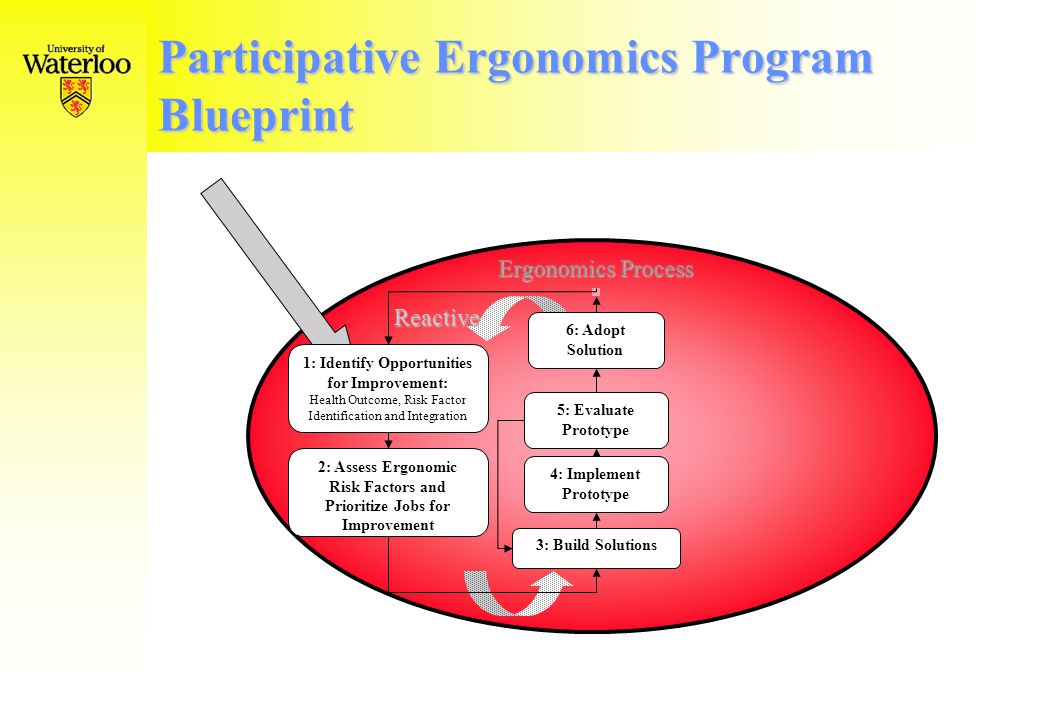
Participative Ergonomics Program Blueprint Ergonomics Process 1: Identify Opportunities for Improvement: Health Outcome, Risk Factor Identification and Integration 2: Assess Ergonomic Risk Factors and Prioritize Jobs for Improvement 3: Build Solutions 4: Implement Prototype 5: Evaluate Prototype 6: Adopt Solution Reactive

46
Participative Ergonomics Program Blueprint Ergonomics Process 3: Build Solutions 4: Implement Prototype 5: Evaluate Prototype 6: Adopt Solution Proactive 7b: Employ Ergonomic Design Criteria and Purchasing Guidelines 7a: Use Feed-- back from Previous designs and plants + +

47
Participative Ergonomics Program Blueprint Ergonomics Program Training and Education Management of the Ergonomics Program Evaluation Process (Medical Management) Documentation (Compliance Assurance) Participation and Consultation Management Support of Ergonomics and Resources Corporate Ergonomics Policy Ergonomic Tools, Techniques and Skills Ergonomics Process
 Documentation (Compliance Assurance) Participation and Consultation Management Support of Ergonomics and Resources Corporate Ergonomics Policy Ergonomic Tools, Techniques and Skills Ergonomics Process")
Similar presentations



 Job Hazard Analysis Mishap reporting 1 This class is only intended to familiarize you with the programs in place.>")














 Prevention Centre of Research Expertise for.>")

