Download presentation
Presentation is loading. Please wait.

1
Overview of Chronic Disease Care: The Next Level Mike Davies, MD FACP Mark Murray and Associates

3
Copyright restrictions may apply. Jemal, A. et al. JAMA 2005;294:1255-1259. Trends in Age-Standardized Death Rates for the 6 Leading Causes of Death (US) 1970-2002
")
4
Clinical Care: 10 Topics Prevention –Flu Vaccination –Pneumonia Vaccination –Breast Cancer –Cervical Cancer –Colon Cancer Chronic Disease –HTN –CHF –DM –Lipids –Depression

5
Today Focus on 3 disease categories Consider the current performance gaps Consider the current system Start to understand tasks in these 3 areas Discuss BHL role and Generalist role Share findings with group

6
Hilleman, D. E. et al. Chest 2000;118:1278-1285 Annual median treatment costs stratified by year

7
COPD Level 1 = FEV1 > 50% Level 2 = FEV1 35% Level 3 = FEV 1 < 35% Hilleman DE; Chest 2000; 118:1278-85

8
Sicker Patients Use More Resources Hilleman DE, Chest 2000; 118:1278-85

9
COPD Case Management: Randomized Trial in Canada 191 patients hospitalized for COPD in prior year Usual care vs. Education and Self Management –7 to 8 one hour home visits –Action plan with prednisone and antibiotic Rx’s Significant reductions in –Hospitalizations (40%) –All other admissions (57%) –ED visits (41%) Bourbeau J, Arch Int Med 2003; 163:585
 –All other admissions (57%) –ED visits (41%) Bourbeau J, Arch Int Med 2003; 163:585.")
10
What have we learned? Sicker patients use more resources Intervening with the right changes for the right patients keeps them well Specific patient focused interventions work This principle also applies to asthma and other diseases

11
Asthma Tasks History Physical Exam Spirometry Spirometry with and without bronchodialator Peak Expiratory Flow for some patients Diagnosis Treatment with Inhaled corticosteroids and short acting bronchodialators Immunizations Repeat visits Asthma education

12
Asthma Roles Generalist? History Physical Exam Spirometry Spirometry with and without bronchodialator Peak Expiratory Flow for some patients Diagnosis Treatment with Inhaled corticosteroids and short acting bronchodialators Immunizations Repeat visits BHL? Asthma education Measurement for Generalist? F/U education after ER visit or hospitalization? Focused education for the most severe cases? Proactively review PEF during winter for most severe cases? New staff education (for generalist)? Organize patient support groups? Other?
. Organize patient support groups. Other .")
13
Natural History of DM

14
DCCT Trial Type 1 DM # Patients1400 Length of f/u7 years Change in A1C2% % less complications Retinopathy76% Microalbuminuria54% Neuropathy60%

15
DM Type 1 Potential Gain If 120,000 patients with Type 1 DM had an A1C of < 7 compared to now, pts would: –Gain 920,000 years of sight –691,000 years free from dialysis –678,000 years free from limb amputation –611,000 years of life

16
How are we doing? 37% with A1C < 7% 37% with A1C > 8% 36% with DBP < 130/80 40% with DBP > 140/90 52% with cholesterol > 200 Only 7% had all 3 at goal NHANES III (JAMA 2004 291:335)
.")
17
Patients With DM Report Their Needs Peer Support Record Keeping Continuous Education and Reinforcement Menu planning Monitoring of medical advanceds Education of family, co-workers, friends Juvenile diabetes: children’s activities Clinical advice and questions answered

18
Diabetes Tasks Reliably Identify Pts. With Diabetes upon Visit Are appropriate pts. screened? (> 40 q 3 yrs; those with risk factors q 2 yrs) Hgb A1C q 3-6 months? BP q visit? Foot Exam Yearly? Eye Exam Yearly? (or q 2 yrs if no retinopathy and A1C < 8 Diabetes Flow sheet? Pt. Education initial? Pt. education ongoing? Weight Addressed? Smoking Addressed? Physical Activity Addressed? Lipids Yearly? Vaccinations (flu/pneumovax) done?
 Hgb A1C q 3-6 months. BP q visit. Foot Exam Yearly. Eye Exam Yearly. (or q 2 yrs if no retinopathy and A1C < 8 Diabetes Flow sheet. Pt. Education initial. Pt. education ongoing. Weight Addressed. Smoking Addressed. Physical Activity Addressed. Lipids Yearly. Vaccinations (flu/pneumovax) done .")
19
Diabetes Roles Generalist Reliably Identify Pts. With Diabetes upon Visit Are appropriate pts. screened? (> 40 q 3 yrs; those with risk factors q 2 yrs) Hgb A1C q 3-6 months? BP q visit? Foot Exam Yearly? Eye Exam Yearly? (or q 2 yrs if no retinopathy and A1C < 8 Diabetes Flow sheet? Pt. Education initial? Pt. education ongoing? Weight Addressed? Smoking Addressed? Physical Activity Addressed? Lipids Yearly? Vaccinations (flu/pneumovax) done? BHL Patient education? Family education? Proactively educate highest risk patients? (high A1C) Focused education on those with ER visits and hospitalizations due to DM? Measurement for clinic? Professional development education for generalist staff?
 Hgb A1C q 3-6 months. BP q visit. Foot Exam Yearly. Eye Exam Yearly. (or q 2 yrs if no retinopathy and A1C < 8 Diabetes Flow sheet. Pt. Education initial. Pt. education ongoing. Weight Addressed. Smoking Addressed. Physical Activity Addressed. Lipids Yearly. Vaccinations (flu/pneumovax) done. BHL Patient education. Family education. Proactively educate highest risk patients. (high A1C) Focused education on those with ER visits and hospitalizations due to DM. Measurement for clinic. Professional development education for generalist staff .")
20
Hypertension Preceded development of heart failure in 91% of cases Is associated with a 2 to 3 fold increased risk of heart failure after adjustment for age and other factors Carried greatest risk for development of heart failure among all risk factors (HTN, MI, Angina, DM, LVH, Valvular heart disease Levy D et al. JAMA 1996 275; 1557-1562

21
HTN LVH MI Diastolic Dysfunction Systolic Dysfunction CHF Normal LV Structure & Function LV Remodeling Sub-clinical LV Dysfunction Overt Heart Failure Progression….. Vasan RS, Levy D; Arch Int Med 1996; 156; 1790

22
Benefits of Beta Blocker in HTN Meta-analysis of 18 randomized studies (N = 18,883) use of Beta Blockers decreased –Risk of stroke by 29% –Risk of CHD by 7% –Risk of CHF by 42% Pasly BM et al JAMA 1997, 277; 536-545
 use of Beta Blockers decreased –Risk of stroke by 29% –Risk of CHD by 7% –Risk of CHF by 42% Pasly BM et al JAMA 1997, 277;")
23
But BP control is inadequate because…. Physicians accept inadequate control It is difficult to control with one drug BP goals now more aggressive than in past Lack of patient compliance –Perceived side effect –Frequency of dosing JNC Arch Inter Med 1997

24
Hypertension (Vascular Health) One of four adults has HTN 1/3 don’t know they have it Continuous, consistent, and independent relationship of BP and heart attack, heart failure, stroke, and kidney disease
 One of four adults has HTN 1/3 don’t know they have it Continuous, consistent, and independent relationship of BP and heart attack, heart failure, stroke, and kidney disease")
25
Cochrane Review: Interventions used to improve control of BP in patients with HTN 59 Randomized Controlled Trials Found “organized system” of regular review linked to vigorous antihypertensive drug therapy –Decreased 8/12/11 (Systolic, Diastolic, Mean) –Mortality @ 5 years down 1.4% (6.4% vs. 7.8%) Self management decreased diastolic by 2
 Self management decreased diastolic by 2.")
26
InterventionOutcome Self Monitoring ++ Some improvement in BP Control Educate Patient No Change Educate Health Professional No Change Nurse/Pharmacist Led Care Too Early to Tell Organized System of Regular Review linked to Drug Therapy ++++ Improvement in both BP Control and Mortality Appointment Reminders Increased F/U visits Source: Cochrane Review

27
4 Strategies for HTN Pay attention to blood pressure before it is high In people over age 50, systolic pressure is more important than diastolic Two (or more) drugs are better than one for most patients Build trusting relationships that motivate patients to be healthy
 drugs are better than one for most patients Build trusting relationships that motivate patients to be healthy")
28
HTN Who? All patients get BP reading every time by nurse What? Nurse records BP and notifies doctor if high Where? Clinic When? Every visit Why? Detect and manage HTN

29
Hypertension Goal Good control Denominator: All patients with HTN Numerator: Those patients with both systolic and diastolic BP < 140/90 Poor Control Denominator: All patients with HTN Numerator: Those patients with either systolic or diastolic BP > 160/100

30
Hypertension tasks HTN Pts. Identified? BP taken at each visit? (and re-taken if high?) Routine lab tests done on all patients with HTN initially? Pts. outside of treatment targets addressed? Pts. On at least 2 drugs? HTN Flow sheet used? HTN Education for Patients/Families Prevention Assessment/Activities
 Routine lab tests done on all patients with HTN initially. Pts. outside of treatment targets addressed. Pts. On at least 2 drugs. HTN Flow sheet used. HTN Education for Patients/Families Prevention Assessment/Activities.")
31
New World Identify chronic diseases for practice and panel Identify key interventions Build a reliable system Measure outcomes Continually improve

32
What are the financial and staffing implications/costs? HTN as an example

33
HTN Tasks Initial and Over 5 Visits Measure BP Look for Target Organ Damage –Exam (Perform and interpret) –Labs: CBC, UA, Chemistries, Lipids, Glucose (Order, do and interpret) –EKG (Order and interpret) Facilitate Lifestyle Changes –Weight (Counseling/encourage/assist goal setting & improvement) –Exercise (Counseling/encourage/assist goal setting & improvement) –Diet (Counseling/encourage/assist goal setting & improvement) –Smoking (Counseling/encourage/assist goal setting & improvement) Reassess/review/adjust plan over time (Assess, Decide, order, Carry out plan)
 –Labs: CBC, UA, Chemistries, Lipids, Glucose (Order, do and interpret) –EKG (Order and interpret) Facilitate Lifestyle Changes –Weight (Counseling/encourage/assist goal setting & improvement) –Exercise (Counseling/encourage/assist goal setting & improvement) –Diet (Counseling/encourage/assist goal setting & improvement) –Smoking (Counseling/encourage/assist goal setting & improvement) Reassess/review/adjust plan over time (Assess, Decide, order, Carry out plan)")
34
Time for Each Task (Estimate) Tasks Time (min) Measure BP 2 Exam5 Order Lab/XR1-3 Interpret Tests2 Facilitate Patient Lifestyle Changes 20 Reassess BP2 Order/Adjust Meds 1-3
 Tasks Time (min) Measure BP 2 Exam5 Order Lab/XR1-3 Interpret Tests2 Facilitate Patient Lifestyle Changes 20 Reassess BP2 Order/Adjust Meds 1-3")
35
TasksProviderRNLPNMA Measure BP XXXX Exam X Order Lab/XR XX* Interpret Tests X Facilitate Patient Lifestyle Changes XXXX Reassess BP XXXX Order/Adjust Meds X * = “Functions Under Standardized Protocols Who Could Perform Tasks?

36
Level of Effort (in Time) Tasks Time (min)FrequencyTotal (min) Initial BP 224 Exam5210 Order Lab/XR1-3 1-9 Interpret Tests 21-32-6 Facilitate Patient Lifestyle Changes 151-315-45 Reassess BP25-710-14 Order/Adjust Meds 1-333-9
 Tasks Time (min)FrequencyTotal (min) Initial BP 224 Exam5210 Order Lab/XR Interpret Tests Facilitate Patient Lifestyle Changes Reassess BP Order/Adjust Meds")
37
Total Time for 5 Visits Tasks Total (min) Initial BP 4 Exam 10 Order Lab/XR 1-9 Interpret Tests 2-6 Facilitate Patient Lifestyle Changes 15-45 Reassess BP 10-14 Order/Adjust Meds 3-9 Total 45-97
 Initial BP 4 Exam 10 Order Lab/XR 1-9 Interpret Tests 2-6 Facilitate Patient Lifestyle Changes Reassess BP Order/Adjust Meds 3-9 Total 45-97")
38
Thought Experiment….Doc Doc does it all –Cost = Doc time @ $1.42/min X 70 min= $99.40 –Doc doing work someone else could do! (Not doing other high value work) –Quality presumably good, but some studies say docs are not as good at protocol work…. –Access probably poor for other patients –Visits relatively low value
 –Quality presumably good, but some studies say docs are not as good at protocol work…. –Access probably poor for other patients –Visits relatively low value.")
39
Thought experiment….Nurse Nurse does it all –Cost = Nurse time @ $0.66/min X 70 min = $46.20 –Nurse not able to do all parts of the work (order/interpret)…although APN may….. –Quality presumably good but nurses may not be good at non-protocol work (secondary HTN dx, etc) –Access to doc probably better (less work for doc) –Value of doc visits probably higher –Access to nurse may be poor if not enough nurses
 –Access to doc probably better (less work for doc) –Value of doc visits probably higher –Access to nurse may be poor if not enough nurses.")
40
Thought Experiment MA MA does it all –Cost = MA time @ $0.24/min X 70 = $16.80 –MA cannot do all parts of the work (order or interpret tests) – Quality poor since all tasks not completed –Access to doc and nurse both probably better if MA takes some of work away –Value of doc and nurse time both higher
 – Quality poor since all tasks not completed –Access to doc and nurse both probably better if MA takes some of work away –Value of doc and nurse time both higher")
41
Who Should Perform Tasks? (Assumes each performs at highest possible level) Tasks Provider RNLPNMA Measure BP X ExamX Order Lab/XRX* Interpret Tests X Facilitate Patient Lifestyle Changes X Reassess BPX Order/Adjust Meds X
 Tasks Provider RNLPNMA Measure BP X ExamX Order Lab/XRX* Interpret Tests X Facilitate Patient Lifestyle Changes X Reassess BPX Order/Adjust Meds X.")
42
Cost (Min) with Team Tasks Total (min)Doc Time (min) Team Time (min) Initial BP 4 Exam 10 Order Lab/XR 1-9 Interpret Tests 2-6 Facilitate Patient Lifestyle Changes 15-45 Reassess BP 10-14 Order/Adjust Meds 3-9 Total 45-9715-2526-68
 with Team Tasks Total (min)Doc Time (min) Team Time (min) Initial BP 4 Exam 10 Order Lab/XR 1-9 Interpret Tests 2-6 Facilitate Patient Lifestyle Changes Reassess BP Order/Adjust Meds 3-9 Total")
43
Tasks in First 5 Visits Total (min) Doc Time ($1.42/min) Team Time (MA $0.24/min; Nurse $0.66/min) Initial BP 40.96 Exam 1014.20 Order Lab/XR 1-90.66 – 5.94 Interpret Tests 2-62.84 – 8.52 Facilitate Patient Lifestyle Changes 15-45 3.60 – 10.80 OR 9.90 – 29.70 Reassess BP 10-142.40 – 3.36 Order/Adjust Meds 3-9 4.26 – 12.78 Total 45-97 min $21.30 – 35.35 $7.62 – 39.96
 Doc Time ($1.42/min) Team Time (MA $0.24/min; Nurse $0.66/min) Initial BP Exam Order Lab/XR – 5.94 Interpret Tests – 8.52 Facilitate Patient Lifestyle Changes – OR 9.90 – Reassess BP – 3.36 Order/Adjust Meds – Total min $21.30 – $7.62 – 39.96")
44
Team Analysis Doc NurseMATotal Time (min)2224 70 Cost ($)31.2415.845.7652.80
 Cost ($)")
45
Bottom Line HTN Cost Doc Alone Team Time (min)70 Cost ($)99.4052.80 QualityGood AccessLessMore
70 Cost ($) QualityGood AccessLessMore")
46
Patients with HTN No ER visits or admits for HTN ER visits for HTN Admits For HTN

47
Patients with HTN No ER visits or admits for HTN ER visits for HTN Admits For HTN Population Of Focus For Intervention

48
Roles Generalist HTN Pts. Identified? BP taken at each visit? (and re-taken if high?) Routine lab tests done on all patients with HTN initially? Pts. outside of treatment targets addressed? Pts. On at least 2 drugs? HTN Flow sheet used? HTN Education for Patients/Families Prevention Assessment/Activities BHL HTN education? Vascular education? Family education? f/u calls for patients with highest readings? Measurement for clinic? Staff development inservices? Other?
 Routine lab tests done on all patients with HTN initially. Pts. outside of treatment targets addressed. Pts. On at least 2 drugs. HTN Flow sheet used. HTN Education for Patients/Families Prevention Assessment/Activities BHL HTN education. Vascular education. Family education. f/u calls for patients with highest readings. Measurement for clinic. Staff development inservices. Other .")
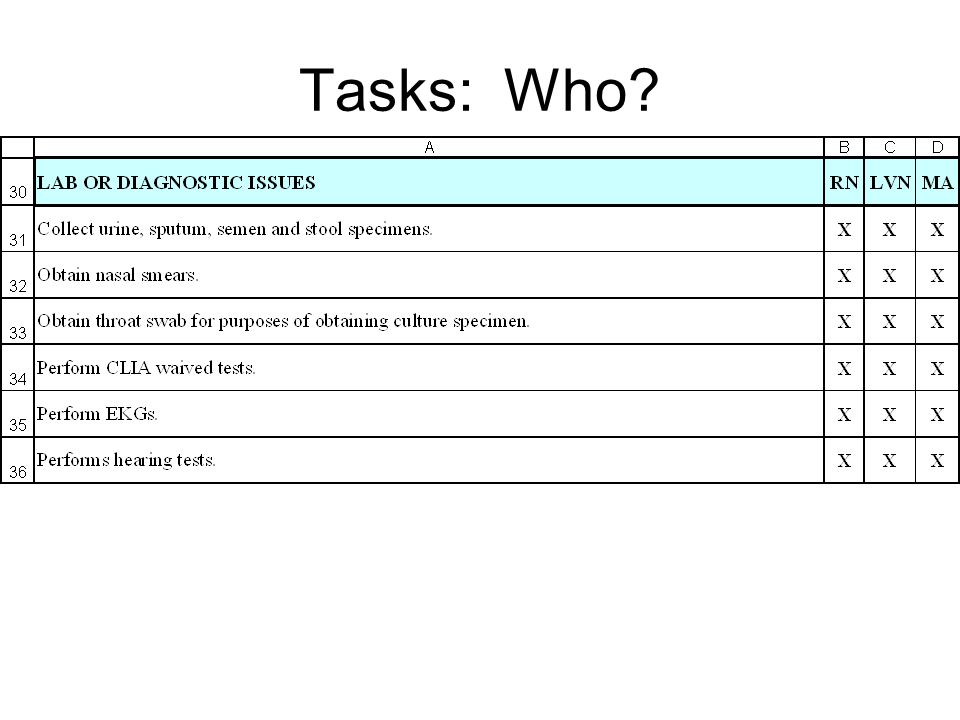
49
Tasks: Who?

54
General Approach Identify topic Agree on Measurement Feedback of results Engagement of teams in improvement

55
Pneumococcal Vaccination Rates VHA Healthy People 2000 Iowa99* * Iowa: Petersen, Med Care 1999;37:502-9. >65/ch dz

56
Beta Blocker following AMI in VHA Medical Centers VHA NCQA Non-Govt AHCPR (NJ)
")
58
One Network’s results with retrospective measurement and feedback 1. A1C in last year and most recent A1C < 9 2. Most recent BP this year < 140/90 3. Retinal Eye Exam in last 2 years (or last year if A1C > 8 or known retinopathy 4. LSL in last year and most recent LSL < 100 11% of patients compliant with none of measures 50% compliant with at least 3 of the 4 measures

59
Changes Switched from retrospective reporting on past results to a prospective system that forecasts clinician’s patients chronic disease screening needs for the future

60
Key Elements of one VA Network Patients Periodic letters containing: –Guidelines and goals –Personal compliance status –Tests due now –Actions needed to improve Ability to self schedule recommended lab and tests Reliable feedback on disease Access to education and self management support Primary Care Team Summary Measures Detail of patients not meeting measures Dedicated time to address chronic disease Focus on profiling population and disease Informed Activated Patient Prepared Proactive Practice Team

61
Patient Centered Care Products Diabetes Resource Center –Multidisciplinary clinic Individualized Patient Letter –All patients vs. those needing tests Automated Orders –For eye exams and labs BP and Foot exams in Resource Center –Patients self schedule DM teaching –Standard films and powerpoints –Customized care Web Access to Data –Stand alone web site Phone Clinic –Providers plan on phone time to follow-up on some patients

62
Key Points Chronic Disease is very common Chronic Disease outcomes improve dramatically with careful management of key elements of care Traditional visit based care does not perform well for our patients Increasing access and team care is needed

63
But How?

66
IOM Framework

67
Resources for Improved Outcomes Interactions –Communication between patients and staff Clinical Information Systems –To identify and help inform patients and staff Decision Support Tools –Such as Standard Forms and Data Delivery System –The processes, tasks, and results Patient Self Management –Activates and engages the patients Community –Support Groups

68
Future Professional Team (Doc/Nurse/MA/Others) –Screen and evaluate results of screening –Teach alone and in groups –Evaluate and f/u on positives Self Management –Entire change in interaction style –Patient goal setting
 –Screen and evaluate results of screening –Teach alone and in groups –Evaluate and f/u on positives Self Management –Entire change in interaction style –Patient goal setting")
69
Tele-Eye Outcomes 68% reduction in demand for diabetic eye exams in Eye Clinic –93% of Primary Care Exams do not require Eye clinic follow-up Increased diabetic screening rate 75% 91% completed annual exam Reduced eye clinic waiting time 80 days 11 days

70
Examples of Outlier Strategies (For Future) Service Agreements with BHL Tele-health Some home visits Group Visits? Individual letters with disease profile Web based self care

71
Telehealth Overview The Future Tele-homecare

72
What happens to me today? What is the process? Is the process timely? Is the process reliable? How are we doing as a team? Which patients need help? What help do they need? Dual Perspective Needed

73
Generalist Tasks for today’s care Uses standard tools Happens reliably Core care understood Most done by team Generalist and Specialist (BHL) Clinic does individual episode of care Measurement? Help with outliers? Assist with Population Mgt? Roles

74
Focus Understand current focus of generalist clinics and BHL Focus on flow map, task analysis, and improvement of generalist clinical care Review wider area of clinical care Discuss ideal flow process for clinical care

75
Instructions for breakout # 1 Go to assigned small group (Asthma, DM, or HTN) Make a list of tasks done now (current state) Then brainstorm the ideal state (ideally, what tasks should be done by BHL and what tasks done by the generalist clinic) Report out
 Make a list of tasks done now (current state) Then brainstorm the ideal state (ideally, what tasks should be done by BHL and what tasks done by the generalist clinic) Report out")
76
Breakout # 2: At home in the clinic Focus on the 3 conditions Focus on the tasks that should be done in the clinic Flow map the process Assign the tasks: who does what? Sketch out the tool: paper?

Similar presentations












 Asthma GP monitoring Guideline 2) Asthma Diagnosis Guideline 3) Acute asthma.>")
 Asthma.>")











