Download presentation
Presentation is loading. Please wait.

1
Cerebrovascular Accident Aka: Stroke Brain Attack

2
http://www.strokecenter.org/ education/index.html

3
In this Session Brain structure and function Cerebral circulation Haemorrhagic stroke TIA Ischaemic stroke Manifestations Diagnosis and management Long term disabilities

4
Review of Brain Structure & Function

5
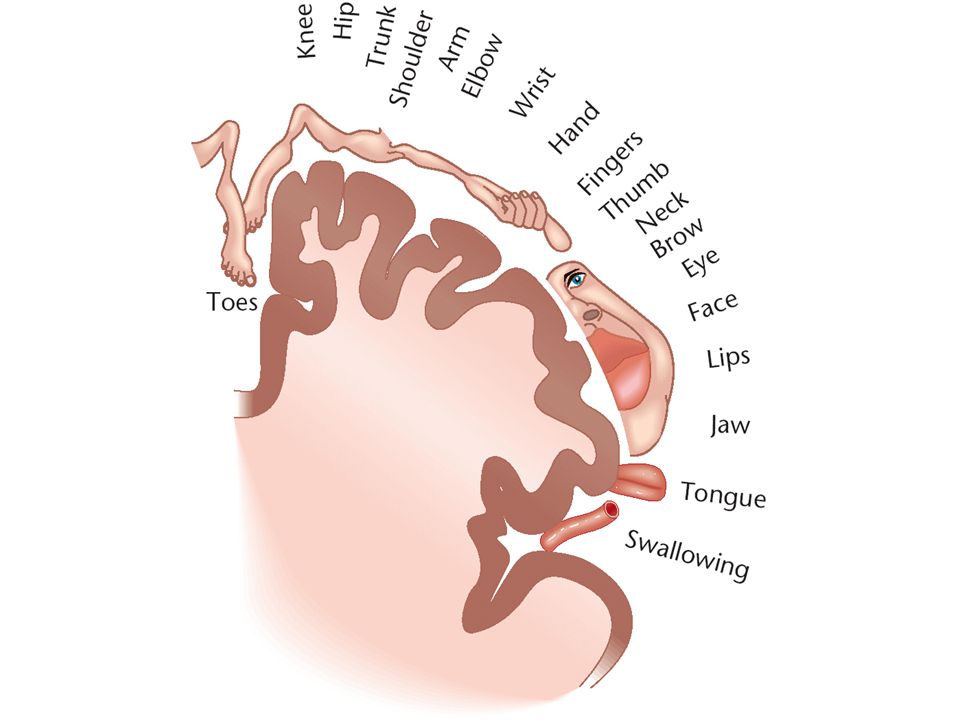
Cerebral Cortex –Divided into Hemispheres –Functions Motor - Controlling voluntary movements Sensory - Registers and processing sensations Association - Higher mental functions Language - Comprehension and Production

7
Cerebral Hemispheres: Lobes –Frontal –Temporal –Parietal –Occipital

10
Other Brain Structures –Brainstem –Medulla –Reticular formation

12
Other Brain Structures –Thalamus

14
Other Brain Structures –Cerebellum

16
Other Brain Structures –Hypothalamus

18
Language Wernicke’s Area –Temporal lobe –Recognition of spoken & written language –Composition of spoken and written language

19
Language Broca’s Area –Frontal lobe –Speech motor function

21
Coordination of Language in the Brain - How do we read aloud?

22
Vision

24
Cerebral Circulation

27
Arteries supplying the Brain Aortic Arch Common Carotid Artery (left & right) internal carotid artery (Left & Right) Circle of Willis Aortic Arch Subclavian Arteries Vertebral Arteries (Left & Right) Merge to form Basilar Artery Circle of Willis Circle of Willis left & right: Anterior, Middle & Posterior Cerebral Arteries
 internal carotid artery (Left & Right) Circle of Willis Aortic Arch Subclavian Arteries Vertebral Arteries (Left & Right) Merge to form Basilar Artery Circle of Willis Circle of Willis left & right: Anterior, Middle & Posterior Cerebral Arteries")
29
Definition of Stroke Acute focal neurological deficit as a result of vascular disorder

30
Epidemiology Third leading cause of death Over 70% strokes in people aged > 65 yr Ave. age males 68 yr, female 74 yr 1998 Age-standardised stroke mortality (per 100,000 pop) is 43 male, 42 female A leading cause of Disability
 is 43 male, 42 female A leading cause of Disability.")
31
Risk Factors for Stroke Advanced age Systolic hypertension Diabetes mellitus Hypercholesterolemia Carotid artery stenosis TIAs CIGARETTE SMOKING Lack of exercise CV disease especially atrial fibrillation Increased weight

32
Non-Modifiable Risk Factors Age –Risk doubles for each decade after 55 years of age Gender –Men slightly higher than women Race Heredity

33
AGE and STROKE

34
Modifiable Risk Factors HypertensionRR 4.0 DiabetesRR 1.8 SmokingRR 1.7 Coronary diseaseRR 2.2 TIARR 3.9 Atrial fibrillationRR 2.6-4.5 HyperlipidemiaRR 1.8-2.6

35
Modifiable Risk Factors For ischaemic stroke: Being overweight increases risk by 22% Being obese increases risk by 64%

36
Diet and Stroke Fish: 3 servings a day associated with a 6% lower risk of stroke Fruits and vegetables: >5 servings a day associated with a 26% lower risk of stroke Meat: Each daily serving associated with a 24% increased risk of stroke Reduced-fat milk: associated with a lower risk of stroke vs full-fat milk Chocolate: High consumption associated with a 29% lower risk of stroke

37
Diet and Stroke Coffee: 3 to 4 cups per day associated with a 17% lower risk of stroke Tea: ≥3 cups per day associated with a 21% lower risk of stroke Sugar-sweetened beverages: high intake associated with increased obesity, diabetes, metabolic syndrome, and coronary heart disease Whole grains: high intake associated with a 21% lower incidence of cardiovascular events Rice: intake not associated with risk of stroke

38
Types of Stroke Haemorrhagic AND Ischaemic

39
Haemorrhagic Stroke 15% of strokes Release of blood into the extravascular space Caused by: –Hypertension –Aneurysms –Head Injury

40
Berry Aneurysm Cause unknown Usually around Circle of Willis

42
Haemorrhagic Stroke Rupture of blood vessel causes: –Haemorrhage –Oedema –Compression Death is common

43
Haemorrhage Intracerebral haemorrhage Subarachnoid haemorrhage

44
Transient Ischaemic Attack (TIA) Ministroke or Brain angina Fleeting attack of paralysis, numbness, tingling, aphasia, unilateral blindness or dizziness Zone of penumbra without central infarction Last less than 24 hours
 Ministroke or Brain angina Fleeting attack of paralysis, numbness, tingling, aphasia, unilateral blindness or dizziness Zone of penumbra without central infarction Last less than 24 hours")
45
TIA’s Warning First month after a TIA, carries a 4-8% risk of stroke First year, 12-13%; 24-29% over 5 years Note: Do not have associated pain (rare), so people may ignore them Person should seek immediate medical attention
, so people may ignore them Person should seek immediate medical attention")
46
Ischaemic Penumbra Prolonged hypoperfusion (<10 ml/100 gm/min) leads to Cell death Ischaemic penumbra is a zone of dysfunctional but not dead brain tissue surrounding an infarct Dysfunctional tissue may infarct “Brain is Time”- need treatment within 3 hours
 leads to Cell death Ischaemic penumbra is a zone of dysfunctional but not dead brain tissue surrounding an infarct Dysfunctional tissue may infarct Brain is Time - need treatment within 3 hours")
47
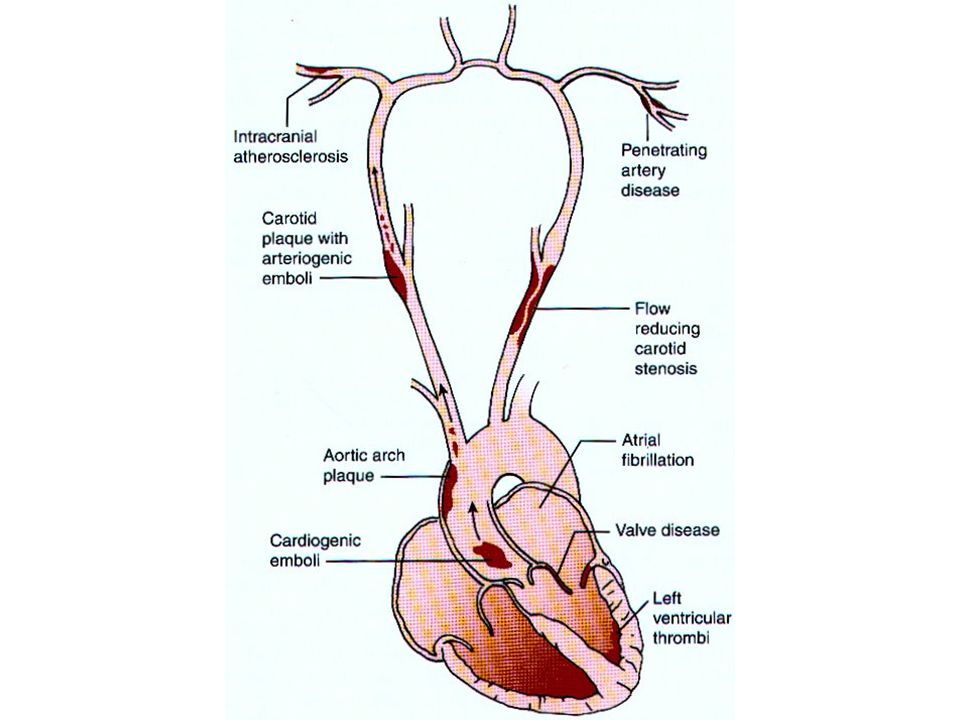
Ischaemic Stroke 85% of all strokes Ischaemic: lack of blood flow Caused by –Emboli –Thrombosis Types are Thrombotic Stroke, Cardiogenic Embolic Stroke, Lacunar Stroke

48
Thrombotic Stroke Most common Common sites are the origins of internal carotid, vertebral arteries and junctions of basilar and vertebral arteries Normally a single cerebral artery is affected

50
Cardiogenic Emboli Stroke Caused by a moving blood clot Most common site is middle cerebral artery Most emboli originate in the left heart Atrial fibrillation and other heart disease predisposes to embolus formation

51
Lacunar Stroke Small infarcts in deeper, noncortical parts of brain or brain stem Cause can be embolism, hypertension, small haemorrhages Leave lacunae upon healing Produce “lacunar syndromes” MRI for diagnosis

52
Manifestations

53
Terminology Hemiplegia – Paralysis on one side of body Hemiparesis – weakness on one side of body Hemianopia –vision loss in one side of visual field Aphasia –language disturbance (speech, comprehension, writing) Dysarthria – slurred speech
 Dysarthria – slurred speech")
54
Terminology Diplopia – double vision Dysphagia – difficulty swallowing Agnosia – impairment of recognition of sensory stimuli Ataxia – imbalance Apraxia – inability to properly execute movements

55
Presentations of Acute Stroke Alteration in Consciousness Stupor, delirium, coma, confusion, memory loss, seizures Headache; severe and/or neck or facial pain (Not common) Aphasia Facial weakness or asymmetry
 Aphasia Facial weakness or asymmetry")
56
Presentations of Acute Stroke Weakness, paralysis, or sensory loss Ataxia (poor balance, clumsiness, or difficulty walking) Visual loss, monocular or binocular Intensive vertigo, double vision
 Visual loss, monocular or binocular Intensive vertigo, double vision")
57
Anterior Cerebral Artery Occlusion Paralysis of contralateral leg Paresis of contralateral arm Problems making decisions Speech disturbance (aphasia if left hemisphere stroke) Some sensory loss over toes, foot, leg
 Some sensory loss over toes, foot, leg")
58
Middle Cerebral Artery Occlusion Contralateral hemiplegia (face & arm) Contralateral Sensory impairment Speech disturbance (aphasia), including difficulty in comprehending written words and writing Some visual field loss
 Contralateral Sensory impairment Speech disturbance (aphasia), including difficulty in comprehending written words and writing Some visual field loss")
59
Posterior Cerebral Artery Occlusion Visual distubances (Hemianopsia, colour blindness) Memory deficits Loss of all sensory modalities (thalamus)
 Memory deficits Loss of all sensory modalities (thalamus)")
60
Basilar Artery Occlusion Complete obstruction of the basilar artery is usually rapidly fatal Rapid onset of unconsciousness and deepening coma. Supplies the Brain Stem

61
Vertebral Artery Occlusion Vertigo at onset Visual distubances (diplopia) Ataxia Dysphagia Dysphonia
 Ataxia Dysphagia Dysphonia")
62
Stroke Diagnosis Neurological Assessment Neuroimaging –Eg. CT, MRI (important for differentiating ischaemic from haemorrhagic stroke) Vascular Imaging –Eg. Angiography Carotid Ultrasound
 Vascular Imaging –Eg. Angiography Carotid Ultrasound.")
63
Management: Ischaemic Stroke Goal: protection of penumbra zone –Maximize cerebral blood flow and blood volume, reduce viscosity –Maintain perfusion pressure Recanalization with thrombolytic therapy Eg. Tissue plasminogen activator (tPA), streptokinase, urokinase Anticoagulants to block occlusive processes (eg. Aspirin)
, streptokinase, urokinase Anticoagulants to block occlusive processes (eg. Aspirin).")
64
Long Term Disabilities Motor deficits Language and speech problems Dysarthria Aphasia Denial or hemiattention

Similar presentations















>")


 Stroke - Overview Third leading cause of death in industrialized countries. Total cost of strokes in the U.S. is roughly.>")

 neurological defecit of sudden onset and lasting> 24h (or leading to death), and of presumed vascular origin 5-10 per.>")










