Download presentation
Presentation is loading. Please wait.

1
Head and Neck Pathologies Orthopedic Assessment III – Head, Spine, and Trunk with Lab PET 5609C

2
Head and Neck Pathologies Sports related concussions – 300,000 mild traumatic brain injuries/yr Sports related concussions – 300,000 mild traumatic brain injuries/yr 3-8% of all high school and collegiate football players sustain concussions each year 3-8% of all high school and collegiate football players sustain concussions each year NCAA Injury Surveillance System had reported concussions constitute 12.2 and 4.8% of all injuries occurring in collegiate hockey and soccer NCAA Injury Surveillance System had reported concussions constitute 12.2 and 4.8% of all injuries occurring in collegiate hockey and soccer

3
Head and Neck Pathologies Concussions – Mild traumatic Brain Injuries Concussions – Mild traumatic Brain Injuries Immediate (but transient) posttraumatic impairment of brain function Immediate (but transient) posttraumatic impairment of brain function Immediate effect – brain cell loss Immediate effect – brain cell loss Secondary damage (↑ risk of brain cell death) Secondary damage (↑ risk of brain cell death) Diagnosis: Diagnosis: Duration of symptoms (i.e. loss of consciousness) Duration of symptoms (i.e. loss of consciousness) Neuropsychological findings Neuropsychological findings
 Duration of symptoms (i.e. loss of consciousness) Neuropsychological findings Neuropsychological findings.")
4
Head and Neck Pathologies Head and Neck Pathologies Concussion: Cognitive Features Concussion: Cognitive Features State of unawareness (i.e. team opponent) State of unawareness (i.e. team opponent) Mental confusion Mental confusion Difficulty concentrating Difficulty concentrating Loss of Consciousness Loss of Consciousness Amnesia Amnesia Anterograde Anterograde Retrograde Retrograde
 State of unawareness (i.e. team opponent) Mental confusion Mental confusion Difficulty concentrating Difficulty concentrating Loss of Consciousness Loss of Consciousness Amnesia Amnesia Anterograde Anterograde Retrograde Retrograde.")
5
Head and Neck Pathologies Head and Neck Pathologies Concussion: Subjective Symptoms Concussion: Subjective Symptoms Headache Headache Dizziness Dizziness Nausea Nausea Loss of Balance Loss of Balance Feeling “dinged” Feeling “dinged” Seeing stars/flashing lights Seeing stars/flashing lights Hearing problems Hearing problems Irritability Irritability Double Vision Double Vision

6
Head and Neck Pathologies Head and Neck Pathologies Concussion: Objective Signs Concussion: Objective Signs Loss of or impaired conscious state Loss of or impaired conscious state Poor coordination/balance Poor coordination/balance Gait unsteadiness Gait unsteadiness Poor concentration Poor concentration Vomiting Vomiting Vacant stare/glassy eyed appearance Vacant stare/glassy eyed appearance Slurred speech Slurred speech Personality changes Personality changes

8
Head and Neck Pathologies Response to Trauma: Biochemical Changes with Concussion Response to Trauma: Biochemical Changes with Concussion Excitatory Neurotransmitters are Released Excitatory Neurotransmitters are Released Influx of extracellular potassium Influx of extracellular potassium Altered ionic balance Altered ionic balance Brain enters state of Hypermetabolism (Hyperglycolysis) Brain enters state of Hypermetabolism (Hyperglycolysis) Can last up to 7-10 days Can last up to 7-10 days During this state, Brain needs extra nutrients, sensitive to inadequate blood flow During this state, Brain needs extra nutrients, sensitive to inadequate blood flow Biochemical changes: Biochemical changes: Implicated in neuronal loss and Cell Death Implicated in neuronal loss and Cell Death Potential Mechanism for Lifelong Depression due to Neuronal Death?? Potential Mechanism for Lifelong Depression due to Neuronal Death??

9
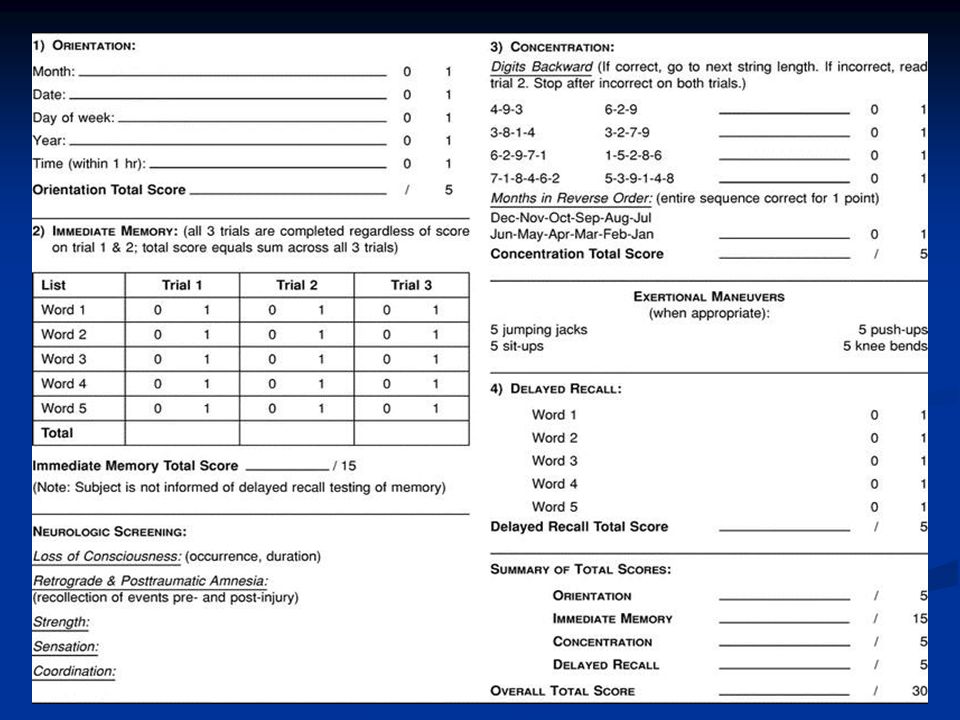
Head and Neck Pathologies Standardized Assessment of Concussion (SAC) Standardized Assessment of Concussion (SAC) Abbreviated neuropsychological test Abbreviated neuropsychological test Immediate objective data Immediate objective data Presence and severity of neurocognitive impairment Presence and severity of neurocognitive impairment On or off field evaluation On or off field evaluation Tests: Tests: Orientation Orientation Immediate Memory Recall Immediate Memory Recall Concentration Concentration Delayed Recall Delayed Recall Glasgow Coma Scale Glasgow Coma Scale Severe brain injury Severe brain injury Normal score: 15 Normal score: 15 > 11: Excellent prognosis for recovery > 11: Excellent prognosis for recovery < 7: Serious brain dysfunction < 7: Serious brain dysfunction
 Standardized Assessment of Concussion (SAC) Abbreviated neuropsychological test Abbreviated neuropsychological test Immediate objective data Immediate objective data Presence and severity of neurocognitive impairment Presence and severity of neurocognitive impairment On or off field evaluation On or off field evaluation Tests: Tests: Orientation Orientation Immediate Memory Recall Immediate Memory Recall Concentration Concentration Delayed Recall Delayed Recall Glasgow Coma Scale Glasgow Coma Scale Severe brain injury Severe brain injury Normal score: 15 Normal score: 15 > 11: Excellent prognosis for recovery > 11: Excellent prognosis for recovery < 7: Serious brain dysfunction < 7: Serious brain dysfunction")
11
RESPONSEPOINTSACTION Eye Opening Spontaneously Spontaneously4 Reticular system intact; pt. may not be aware To verbal command To verbal command3 Opens eyes when told to do so To pain To pain2 Opens eyes in response to pain None None1 Does not open eyes to any stimuli Verbal Oriented, converses Oriented, converses5 Relatively intact CNS; aware of self and surroundings Disoriented, converses Disoriented, converses4 Well articulated, organized, but disoriented Inappropriate words Inappropriate words3 Random, exclamatory words Incomprehensible Incomprehensible2 No recognizable words No response No response1 No audible sounds Motor Obeys verbal commands Obeys verbal commands6 Readily moves limbs when told to Localizes painful stimuli Localizes painful stimuli5 Moves limb in effort to avoid pain Flexion withdrawal Flexion withdrawal4 Pulls away from pain with a flexion motion Abnormal flexion Abnormal flexion3 Exhibits decorticate rigidity Extension Extension2 Exhibits decerebrate rigidity No response No response1 Demonstrates dypotonicity, flaccid: Suggests loss of medullary function or spinal cord injury

13
Concussion Grading: University of North Carolina

14
Grade 1 st Concussion 2 nd Concussion 3 rd Concussion Grade 1 (mild) May return to play if asymptomatic Return to play in 2 weeks if athlete is asymptomatic during the previous week Terminate season; may return to play the following season if asymptomatic Grade 2 (moderate) Return to play after being asymptomatic for 1 week Out a minimum of 1 month; may return to play then if asymptomatic for 1 week; consider termination of season Terminate season; may return to play the following season if asymptomatic Grade 3 (severe) Out a minimum of 1 month; may then return to play if asymptomatic for 1 week Terminate season; may return to play the following season if asymptomatic; Consider terminating career Terminate career in contact sports
 May return to play if asymptomatic Return to play in 2 weeks if athlete is asymptomatic during the previous week Terminate season; may return to play the following season if asymptomatic Grade 2 (moderate) Return to play after being asymptomatic for 1 week Out a minimum of 1 month; may return to play then if asymptomatic for 1 week; consider termination of season Terminate season; may return to play the following season if asymptomatic Grade 3 (severe) Out a minimum of 1 month; may then return to play if asymptomatic for 1 week Terminate season; may return to play the following season if asymptomatic; Consider terminating career Terminate career in contact sports")
15
Head and Neck Pathologies Return to Play Guidelines: Grade 0 Concussion Return to Play Guidelines: Grade 0 Concussion Remove athlete from contest Remove athlete from contest Examine immediately: Examine immediately: Abnormal cranial nerve function Abnormal cranial nerve function Cognition Cognition Coordination Coordination Postconcussive symptoms (both at rest and with exertion) Postconcussive symptoms (both at rest and with exertion) Return to contest: Return to contest: Exam is normal and athlete asymptomatic for 20 minutes Exam is normal and athlete asymptomatic for 20 minutes If any Sx. develop within 20 minutes, return that day is NOT permitted If any Sx. develop within 20 minutes, return that day is NOT permitted University of North Carolina Guidelines

16
Head and Neck Pathologies Return to Play Guidelines: Grade 1 Concussion Return to Play Guidelines: Grade 1 Concussion Daily follow-up evaluations Daily follow-up evaluations May begin restricted participation when asymptomatic at rest and after exertion tests for the 2 days May begin restricted participation when asymptomatic at rest and after exertion tests for the 2 days Unrestricted participation allowed if asymptomatic for 1 additional day and neuropathological and balance testing normal Unrestricted participation allowed if asymptomatic for 1 additional day and neuropathological and balance testing normal University of North Carolina Guidelines

17
Head and Neck Pathologies Return to Play Guidelines: Grade 2 Concussion Return to Play Guidelines: Grade 2 Concussion Remove athlete/prohibit return Remove athlete/prohibit return Examine immediately and at 5-minute intervals for evolving intracranial pathology Examine immediately and at 5-minute intervals for evolving intracranial pathology Re-examine daily Re-examine daily May return to restricted participation when ATC and physician are assured athlete has been asymptomatic at rest and with exertion testing for 4 days May return to restricted participation when ATC and physician are assured athlete has been asymptomatic at rest and with exertion testing for 4 days Unrestricted participation if asymptomatic for additional 2 days and performing restricted activities normally Unrestricted participation if asymptomatic for additional 2 days and performing restricted activities normally University of North Carolina Guidelines

18
Head and Neck Pathologies Return to Play Guidelines: Grade 3 Concussion Return to Play Guidelines: Grade 3 Concussion Treat athlete on the field as if cervical spine injury has occurred Treat athlete on the field as if cervical spine injury has occurred Immediate re-examination at 5-minute intervals for signs of intracranial pathology Immediate re-examination at 5-minute intervals for signs of intracranial pathology Return based on resolution of symptoms: Return based on resolution of symptoms: If symptoms totally resolve within 1 week, return to restricted participation when athlete has been asymptomatic at rest and exertion for 10 days. If asymptomatic for an additional 3 days of restricted activity, athlete may return to full participation If symptoms totally resolve within 1 week, return to restricted participation when athlete has been asymptomatic at rest and exertion for 10 days. If asymptomatic for an additional 3 days of restricted activity, athlete may return to full participation University of North Carolina Guidelines

20
University of North Carolina Return to Play Progression

21
Head and Neck Pathologies Postconcussion Syndrome: Postconcussion Syndrome: Extended symptoms (cognitive impairment) Extended symptoms (cognitive impairment) Altered neurotransmitter function Altered neurotransmitter function Occurs more frequently in women Occurs more frequently in women Symptoms: Symptoms: ↓ attention span ↓ attention span Trouble concentrating Trouble concentrating Impaired memory and irritability Impaired memory and irritability Exercise induced headaches, dizziness, premature fatigue Exercise induced headaches, dizziness, premature fatigue Balance disruption, ↓ cognitive performance Balance disruption, ↓ cognitive performance
 Extended symptoms (cognitive impairment) Altered neurotransmitter function Altered neurotransmitter function Occurs more frequently in women Occurs more frequently in women Symptoms: Symptoms: ↓ attention span ↓ attention span Trouble concentrating Trouble concentrating Impaired memory and irritability Impaired memory and irritability Exercise induced headaches, dizziness, premature fatigue Exercise induced headaches, dizziness, premature fatigue Balance disruption, ↓ cognitive performance Balance disruption, ↓ cognitive performance")
22
Head and Neck Pathologies Second Impact Syndrome: Second Impact Syndrome: Athlete who has suffered a head injury sustains a 2 nd head injury before the signs/symptoms of the initial injury have subsided Athlete who has suffered a head injury sustains a 2 nd head injury before the signs/symptoms of the initial injury have subsided Scenario: Athlete suffering from postconcussion symptoms (headache, visual, motor problems) returns to play prematurely…suffers 2 nd injury Scenario: Athlete suffering from postconcussion symptoms (headache, visual, motor problems) returns to play prematurely…suffers 2 nd injury SIS: Athlete appears stunned…within seconds to minutes, displays life-threatening symptoms (semicomatose state, rapidly dilating pupils, respiratory failure) SIS: Athlete appears stunned…within seconds to minutes, displays life-threatening symptoms (semicomatose state, rapidly dilating pupils, respiratory failure) ↑ Intracranial pressure (inability or loss of brain blood supply regulation) ↑ Intracranial pressure (inability or loss of brain blood supply regulation) Time frame to brain stem failure is rapid! (2-5 minutes post- impact) → High mortality rate (50%) Time frame to brain stem failure is rapid! (2-5 minutes post- impact) → High mortality rate (50%)
 → High mortality rate (50%) Time frame to brain stem failure is rapid. (2-5 minutes post- impact) → High mortality rate (50%).")
23
Head and Neck Pathologies Cumulative Injury: Research has shown an ↑ risk of concussion incidence following initial injury Risk of suffering a 2 nd concussion is approximately 4 times that of the chance of initial injury in high school football players Recent study: Collegiate players with previous history (3 or more) were 3 times as likely to suffer a concussion in comparison to those with no prior history
 were 3 times as likely to suffer a concussion in comparison to those with no prior history")
24
Head and Neck Pathologies Epidural Hematoma: Epidural Hematoma: Arterial bleeding between the dura mater and the skull Arterial bleeding between the dura mater and the skull Onset of symptoms → within hours Onset of symptoms → within hours MOI: blow to the head MOI: blow to the head Size of hematoma ↑, condition deteriorates Size of hematoma ↑, condition deteriorates Progression of symptoms: Progression of symptoms: Patient has signs of concussion Patient has signs of concussion Period of very lucid consciousness (may eliminate suspicion of serious concussion) Period of very lucid consciousness (may eliminate suspicion of serious concussion) Patient becomes disoriented, confused, drowsy Patient becomes disoriented, confused, drowsy Patient complaints of headache that ↑ in intensity with time Patient complaints of headache that ↑ in intensity with time Signs and symptoms of cranial nerve disruption Signs and symptoms of cranial nerve disruption Onset of coma Onset of coma Left untreated, death or permanent brain damage occurs Left untreated, death or permanent brain damage occurs
 Period of very lucid consciousness (may eliminate suspicion of serious concussion) Patient becomes disoriented, confused, drowsy Patient becomes disoriented, confused, drowsy Patient complaints of headache that ↑ in intensity with time Patient complaints of headache that ↑ in intensity with time Signs and symptoms of cranial nerve disruption Signs and symptoms of cranial nerve disruption Onset of coma Onset of coma Left untreated, death or permanent brain damage occurs Left untreated, death or permanent brain damage occurs")
25
Head and Neck Pathologies

26
Subdural Hematoma: Subdural Hematoma: Hematoma between the brain and dura mater Hematoma between the brain and dura mater Usually involves venous bleeding Usually involves venous bleeding Slow accumulation of blood (low BP) Slow accumulation of blood (low BP) Symptoms may occur hours, days, or even weeks after initial trauma Symptoms may occur hours, days, or even weeks after initial trauma Simple subdural hematoma: Simple subdural hematoma: No direct cerebral damage No direct cerebral damage Complex subdural hematoma: Complex subdural hematoma: Contusions of brain’s surface with associated swelling Contusions of brain’s surface with associated swelling
 Slow accumulation of blood (low BP) Symptoms may occur hours, days, or even weeks after initial trauma Symptoms may occur hours, days, or even weeks after initial trauma Simple subdural hematoma: Simple subdural hematoma: No direct cerebral damage No direct cerebral damage Complex subdural hematoma: Complex subdural hematoma: Contusions of brain’s surface with associated swelling Contusions of brain’s surface with associated swelling")
27
Head and Neck Pathologies

28
Skull Fractures: Skull Fractures: History: History: Onset: Acute Onset: Acute Pain characteristics: Pain over impact site, possible headache Pain characteristics: Pain over impact site, possible headache MOI: Blunt trauma to head MOI: Blunt trauma to head Inspection: Inspection: Bleeding Bleeding Ecchymosis under eyes and over mastoid process Ecchymosis under eyes and over mastoid process Rounded contour of skull may be lost Rounded contour of skull may be lost Palpation: Palpation: Crepitus Crepitus Do not palpate over obvious deformity Do not palpate over obvious deformity Neurological Tests: Neurological Tests: Cranial nerve assessment, sensory and motor testing Cranial nerve assessment, sensory and motor testing Comments: Comments: Rule out cervical fracture/dislocation Rule out cervical fracture/dislocation No object should be inserted into site of skull laceration No object should be inserted into site of skull laceration A cerebral concussion may be associated with injury A cerebral concussion may be associated with injury Immediate referral Immediate referral

29
Depressed Skull FractureLinear Parietal Skull Fracture Head and Neck Pathologies

30
Cervical Spinal Cord Trauma: Cervical Spinal Cord Trauma: 1976: NCAA and NFHSA outlawed spearing in football 1976: NCAA and NFHSA outlawed spearing in football Present: Estimated that spearing still occurs in 19% of football plays Present: Estimated that spearing still occurs in 19% of football plays Spinal cord function: Inhibition Spinal cord function: Inhibition Impingement or laceration secondary to bony displacement Impingement or laceration secondary to bony displacement Compression secondary to hemorrhage, edema, and ischemia of the cord Compression secondary to hemorrhage, edema, and ischemia of the cord Trauma to spinal cord above C4: ↑ probability of death secondary to dysfunction of brain stem or phrenic nerve Trauma to spinal cord above C4: ↑ probability of death secondary to dysfunction of brain stem or phrenic nerve

31
Head and Neck Pathologies Cervical Fracture or Dislocation: Cervical Fracture or Dislocation: Dislocation: Dislocation: ↑ threat to spinal cord ↑ threat to spinal cord Lower cervical vertebrae (C4-C6) Lower cervical vertebrae (C4-C6) MOI: Neck forced into flexion and rotation MOI: Neck forced into flexion and rotation History: History: Onset: Acute Onset: Acute Chief complaints: Chief complaints: Pain in cervical spine Pain in cervical spine Numbness, weakness, parasthesia radiating into extremities Numbness, weakness, parasthesia radiating into extremities Cervical muscle spasm Cervical muscle spasm Chest pain Chest pain Loss of bladder or bowel control Loss of bladder or bowel control
 Lower cervical vertebrae (C4-C6) MOI: Neck forced into flexion and rotation MOI: Neck forced into flexion and rotation History: History: Onset: Acute Onset: Acute Chief complaints: Chief complaints: Pain in cervical spine Pain in cervical spine Numbness, weakness, parasthesia radiating into extremities Numbness, weakness, parasthesia radiating into extremities Cervical muscle spasm Cervical muscle spasm Chest pain Chest pain Loss of bladder or bowel control Loss of bladder or bowel control")
32
Head and Neck Pathologies Cervical Fracture or Dislocation: History: MOI: Most fractures: axial load Most dislocations: hyperflexion or hyperextension and rotation Predisposing Conditions: ↑ risk of cervical fracture if normal lordoctic curve of cervical spine is ↓ Inspection: Malalignment of cervical spine Head may be abnormally tilted and rotated Unilateral dislocation → head tilts towards site of dislocation; muscles on opposite side are in spasm; muscles on side of dislocation are flaccid Swelling

33
Head and Neck Pathologies Cervical Fracture or Dislocation: Cervical Fracture or Dislocation: Functional Tests: Functional Tests: ROM testing should not be performed if numbness, weakness, or parasthesia radiating into extremities or bowel/bladder signs present ROM testing should not be performed if numbness, weakness, or parasthesia radiating into extremities or bowel/bladder signs present Neurological Tests: Neurological Tests: Upper and lower quarter screen Upper and lower quarter screen Special Tests: Special Tests: Not applicable if fracture/dislocation suspected Not applicable if fracture/dislocation suspected Comments: Comments: Immediate transportation (EMS activation) Immediate transportation (EMS activation)
 Immediate transportation (EMS activation)")
34
Fracture of C4-C5 segmentDislocation: Result - Quadriplegia Head and Neck Pathologies

35
Spinal repair involving four types of spinal reconstruction. Several of the vertebral disks have been replaced with bone graft material. A plate and screws have been used to lock the vertebral bodies of C5, C6 and C7 tightly against the graft. From a posterior approach, lateral mass screws at C4, C5 and C6 prevent rotation and lateral bending. A thin titanium cable and cable clamp has also been used to lash a strut of bone onto the spinous processes of C4 to C7 to resist flexion forward. Head and Neck Pathologies

36
Transient Quadriplegia: Transient Quadriplegia: Body-wide state of decreased or absent sensory and motor function Body-wide state of decreased or absent sensory and motor function MOI: Blow to head (cervical spine forced into hyperextension, hyperflexion or axial load force) MOI: Blow to head (cervical spine forced into hyperextension, hyperflexion or axial load force) Result: Neuropraxia of cervical spinal cord Result: Neuropraxia of cervical spinal cord Predispositions: Predispositions: Spinal stenosis (C3-C4 ) Spinal stenosis (C3-C4 ) Congenital fusion of cervical canal or other abnormalities Congenital fusion of cervical canal or other abnormalities Cervical instability Cervical instability Pavlov ratio 0.80 or less (ratio between diameter of spinal canal and diameter of vertebral body) Pavlov ratio 0.80 or less (ratio between diameter of spinal canal and diameter of vertebral body)
 MOI: Blow to head (cervical spine forced into hyperextension, hyperflexion or axial load force) Result: Neuropraxia of cervical spinal cord Result: Neuropraxia of cervical spinal cord Predispositions: Predispositions: Spinal stenosis (C3-C4 ) Spinal stenosis (C3-C4 ) Congenital fusion of cervical canal or other abnormalities Congenital fusion of cervical canal or other abnormalities Cervical instability Cervical instability Pavlov ratio 0.80 or less (ratio between diameter of spinal canal and diameter of vertebral body) Pavlov ratio 0.80 or less (ratio between diameter of spinal canal and diameter of vertebral body)")
37
Head and Neck Pathologies Transient Quadriplegia: Transient Quadriplegia: Predisposing Conditions: (continued) Predisposing Conditions: (continued) Spear Tackler’s Spine: Spear Tackler’s Spine: Pavlov ratio of <0.8 Pavlov ratio of <0.8 Straight or kyphotic alignment of the neck on a neutral lateral radiograph Straight or kyphotic alignment of the neck on a neutral lateral radiograph Posttraumatic radiographic abnormality Posttraumatic radiographic abnormality Documentation of the patient's use of the spear- tackling technique Documentation of the patient's use of the spear- tackling technique Spear tackler's spine = contraindication for return to play Spear tackler's spine = contraindication for return to play
 Predisposing Conditions: (continued) Spear Tackler’s Spine: Spear Tackler’s Spine: Pavlov ratio of <0.8 Pavlov ratio of <0.8 Straight or kyphotic alignment of the neck on a neutral lateral radiograph Straight or kyphotic alignment of the neck on a neutral lateral radiograph Posttraumatic radiographic abnormality Posttraumatic radiographic abnormality Documentation of the patient s use of the spear- tackling technique Documentation of the patient s use of the spear- tackling technique Spear tackler s spine = contraindication for return to play Spear tackler s spine = contraindication for return to play")
38
Head and Neck Pathologies Transient Quadriplegia: Transient Quadriplegia: Signs and Symptoms: Signs and Symptoms: Initially, resemble those of catastrophic cervical injury Initially, resemble those of catastrophic cervical injury Sensory dysfunction, burning, pain, numbness, parasthesia in upper and lower extremities Sensory dysfunction, burning, pain, numbness, parasthesia in upper and lower extremities Motor dysfunction (weakness to paralysis) Motor dysfunction (weakness to paralysis) Symptoms clear: 15 minutes to 2 days Symptoms clear: 15 minutes to 2 days Diagnosis: Diagnosis: X-rays, CT, MRI, electromyelograms X-rays, CT, MRI, electromyelograms
 Motor dysfunction (weakness to paralysis) Symptoms clear: 15 minutes to 2 days Symptoms clear: 15 minutes to 2 days Diagnosis: Diagnosis: X-rays, CT, MRI, electromyelograms X-rays, CT, MRI, electromyelograms")
Similar presentations











>")









