Download presentation
Presentation is loading. Please wait.

1
Proposal study: Differentiation between idiopathic toe walking and mild diplegia using random forest

2
Definitions: Idiopathic (cause unknown) toe walking Toe-walking at mild diplegia (cerebral palsy) gait analysis Random forest
 toe walking Toe-walking at mild diplegia (cerebral palsy) gait analysis Random forest")
3
What is toe-walking? Toe-walking is failure of the heel to make contact with the floor at the onset of stance or absence of a heel strike. i.e. toe-walking is walking on the toes OR on the ball of foot

4
Cerebral palsy (most common cause) Duchenne muscular dystrophy Myopathy Neuropathy Spinal dysraphism Developmental disorders (ex/ autism) Idiopathic toe walking (diagnosis of exclusion)
 Duchenne muscular dystrophy Myopathy Neuropathy Spinal dysraphism Developmental disorders (ex/ autism) Idiopathic toe walking (diagnosis of exclusion)")
5
Toe-walking without any neurological problems Toddlers (after age of 3 => habitual toe walking) Toe walking with coordinated work of muscles
 Toe walking with coordinated work of muscles")
6
Studies have noted a positive family history of toe walking in children with ITW with a reported incidence of between 10 and 88 % (Fox 2006 ).
.")
7
Congenital short tendo calcaneus (achilles tendon) Limitations in passive ankle dorsiflexion Neurologically: muscle tone, deep tendon reflexes, muscle strength, and sensation are normal Children ambulate independently on bilateral toes at a normal age and walk on their toes from initiation of independent walking
 Limitations in passive ankle dorsiflexion Neurologically: muscle tone, deep tendon reflexes, muscle strength, and sensation are normal Children ambulate independently on bilateral toes at a normal age and walk on their toes from initiation of independent walking")
8
Toe-walking without a decrease in range of joint motion of the ankle joint is reported to be present in children with autism, in children with communication (language) disorders and learning disabilities, as well as in children with fine motor, visuomotor- and gross motor delays
 disorders and learning disabilities, as well as in children with fine motor, visuomotor- and gross motor delays")
9
Cerebral palsy Autism Other developmental disorders

10
Toe walking Other symptoms may be speech delay, seizures, poor coordination, etc.

12
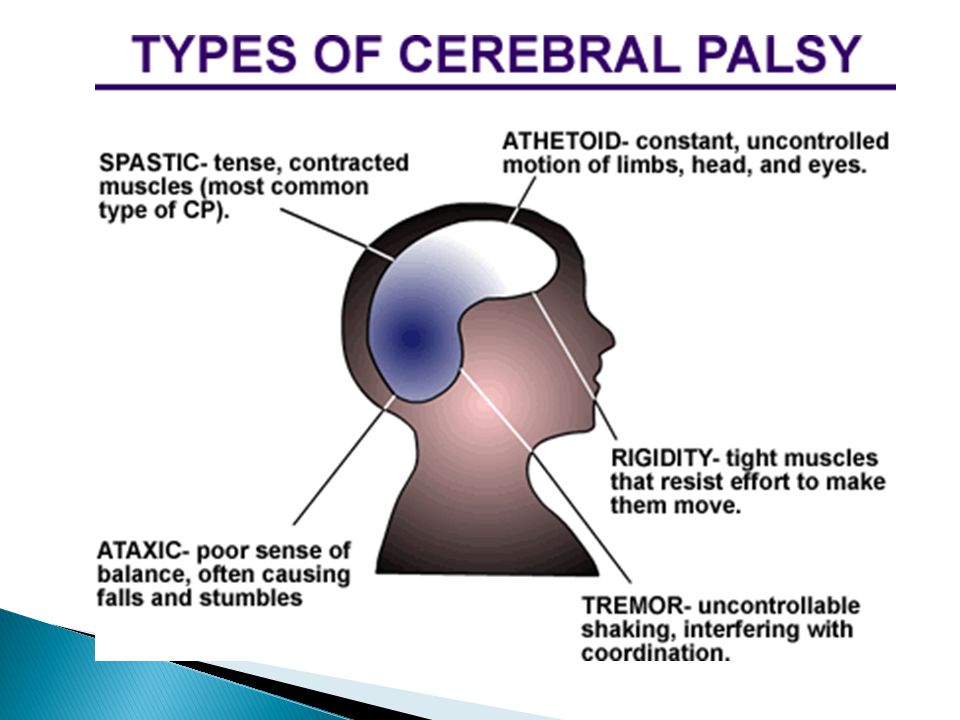
Gait at CP (spastic type)
")
13
Armand, et al carried out 2511 gait analyses in 1736 patients with 11950 trials.4 The authors established three equines gait patterns based on ankle kinematics during stance phase: G1 – A long progressive dorsiflexion followed by plantar flexion until toe off. This pattern was more prevalent in old equinovarus feet, myopathies and neuropathies. G2 – Short lived dorsiflexion with progressive plantar flexion until toe off. This pattern was most common in ITW patients (up to 44% of all in the series). G3 – Double bump pattern, short lived dorsiflexion, short lived plantar flexion and plantar flexion until toe off (cerebral palsy pattern).
. G3 – Double bump pattern, short lived dorsiflexion, short lived plantar flexion and plantar flexion until toe off (cerebral palsy pattern)..")
14
Variable heel strike Reversal of second rocker Early firing of the soleus by EMG evaluation Silence of the gastrocnemius muscle in the swing phase Normal anterior tibial function by EMG. Premature ankle plantar flexion during the second rocker.

15
Equinus (CP) Kinematics ◦ Persistent PF ◦ Knee extension in stance Kinetics ◦ Double bump pattern ◦ Loss of ankle dorsiflexion moment in initial stance ◦ Knee flexion moment in stance
 Kinematics ◦ Persistent PF ◦ Knee extension in stance Kinetics ◦ Double bump pattern ◦ Loss of ankle dorsiflexion moment in initial stance ◦ Knee flexion moment in stance")
Similar presentations

 (MND) are a group of neurological disorders that selectively affect motor neurons.>")


















