Download presentation
Presentation is loading. Please wait.

0
Pneumonia in the Critical Care Setting
Laura Loftis, M.D., M.S. Associate Professor of Pediatrics and Medical Ethics Baylor College of Medicine Text xxx00.#####.ppt 4/15/2017 3:37:49 AM

1
Objectives 1. To review diagnostic criteria for pneumonia
2. To examine treatment algorithms for pneumonia 3. Upon completion, the learner will be able to identify controversies surrounding identification of ventilator associated pneumonia Text xxx00.#####.ppt 4/15/2017 3:37:49 AM

2
Categories of pneumonia
1. Community acquired pneumonia 2. Pneumonia in special populations immunocompromised cystic fibrosis chronically ventilator dependent 3. Ventilator associated pneumonia (VAP) Ventilator associated condition Text X xxx00.#####.ppt 4/15/2017 3:37:49 AM
 Ventilator associated condition. Text. X. xxx00.#####.ppt 4/15/2017 3:37:49 AM.")
3
Categories of pneumonia
1. Community acquired pneumonia 2. Pneumonia in special populations immunocompromised cystic fibrosis chronically ventilator dependent 3. Ventilator associated pneumonia (VAP) Text xxx00.#####.ppt 4/15/2017 3:37:49 AM
 Text. xxx00.#####.ppt 4/15/2017 3:37:49 AM.")
4
Guideline Eligibility Criteria: Age ≥ 60 days to 17 years
Healthy children without underlying conditions Clinical findings of CAP Guideline Exclusion Criteria: Aspiration Recent hospitalization (< 7 days before the onset of illness) Evidence-Based Outcomes Center Team: Quinn Franklin, MS, CCLS, Research Specialist Jennifer Nichols, MPH, Research Specialist Charles Macias, MD, MPH, Director Text xxx00.#####.ppt 4/15/2017 3:37:49 AM
 Evidence-Based Outcomes Center Team: Quinn Franklin, MS, CCLS, Research Specialist. Jennifer Nichols, MPH, Research Specialist. Charles Macias, MD, MPH, Director. Text. xxx00.#####.ppt 4/15/2017 3:37:49 AM.")
6
Clinical Indicators May be subtle Fever
Young infants may have afebrile pneumonia related to Chlamydia trachomatis may be the only sign of occult pneumonia in highly febrile young children Tachypnea absence of tachypnea - single most valuable sign for excluding pneumonia Respiratory distress Retractions, hypoxemia (< 90% sats on RA), irritability, nasal flaring Grunting, when present, is a sign of severe disease and impending respiratory failure Cough may be minimal if primarily an alveolar process In one report, 26 percent of 146 children (<5 years) with fever ≥39ºC, no clinical evidence of pneumonia or other localizing signs, and peripheral white blood cell count ≥20,000/microL had radiographic evidence of pneumonia Ann Emerg Med. 1999;33(2):166; JAMA 1998;279(4):308 xxx00.#####.ppt 4/15/2017
, irritability, nasal flaring. Grunting, when present, is a sign of severe disease and impending respiratory failure. Cough. may be minimal if primarily an alveolar process. In one report, 26 percent of 146 children (<5 years) with fever ≥39ºC, no clinical evidence of pneumonia or other localizing signs, and peripheral white blood cell count ≥20,000/microL had radiographic evidence of pneumonia. Ann Emerg Med. 1999;33(2):166; JAMA 1998;279(4):308. xxx00.#####.ppt 4/15/2017.")
7
Clinical Indicators - Lung exam
Crackles or rales Diminished breath sounds Wheezes more common in atypical or viral Pleural effusion - chest pain with splinting, dullness to percussion, distant breath sounds, pleural friction rub

8
Academic Emergency Medicine, 1996: 3(5), 396
, 396")
9
Radiographic patterns
Segmental consolidation - reasonably specific for bacterial pneumonia but lacks sensitivity not always easy to distinguish from segmental collapse (atelectasis), which is apparent in about 25 percent of children with bronchiolitis In a study of 254 children with radiographically defined pneumonia, the etiology was determined in 215 The sensitivity and specificity of alveolar infiltrate for bacterial pneumonia were 72 and 51 percent, respectively the sensitivity and specificity of interstitial infiltrates for viral pneumonia were 49 and 72 percent, respectively Acta Paediatr. 1993;82(4):360; Pediatr Radiol. 1974;2(3):155.; J Paediatr Child Health. 1990;26(4):209; Pediatrics 1998;102(6):1369; Thorax. 2002;57(5):438; Thorax. 1981;36(6):469
, which is apparent in about 25 percent of children with bronchiolitis. In a study of 254 children with radiographically defined pneumonia, the etiology was determined in 215. The sensitivity and specificity of alveolar infiltrate for bacterial pneumonia were 72 and 51 percent, respectively. the sensitivity and specificity of interstitial infiltrates for viral pneumonia were 49 and 72 percent, respectively. Acta Paediatr. 1993;82(4):360; Pediatr Radiol. 1974;2(3):155.; J Paediatr Child Health. 1990;26(4):209; Pediatrics 1998;102(6):1369; Thorax. 2002;57(5):438; Thorax. 1981;36(6):469.")
10
Alveolar – note airbronchograms
Interstitial

11
Lobar consolidation Atelectasis

12
Pleural effusions

13
RADIOLOGIC EVALUATION
Not necessary to confirm the diagnosis of suspected CAP in children with mild, uncomplicated lower respiratory tract infection who are well enough to be treated as outpatients Radiographic findings are poor indicators of the etiologic diagnosis Radiographic findings may lag behind the clinical findings For hospitalized children to assess for the presence of effusions or other complications

14
Admission Criteria: Unable to tolerate oral fluids and medications; severely dehydrated Moderate or severe respiratory distress Failed outpatient antibiotic treatment Altered mental status Oxygen saturation consistently < 90% Unsafe to send home / poor follow-up

16
CAP Pathogens S pneumoniae Most common bacteria in all age groups
less commonly S aureus or group A strep "Atypical" bacterial pneumonia Mycoplasma pneumoniae or Chlamydophila (formerly Chlamydia) pneumoniae Preschool aged children had as many episodes of atypical bacterial LRIs as older children. Afebrile pneumonia of infancy generally seen between two weeks and four months of life. classically caused by C. trachomatis, Clinical Infectious Diseases 2011: 53(7), e25-e76
 pneumoniae. Preschool aged children had as many episodes of atypical bacterial LRIs as older children. Afebrile pneumonia of infancy. generally seen between two weeks and four months of life. classically caused by C. trachomatis, Clinical Infectious Diseases 2011: 53(7), e25-e76.")
17
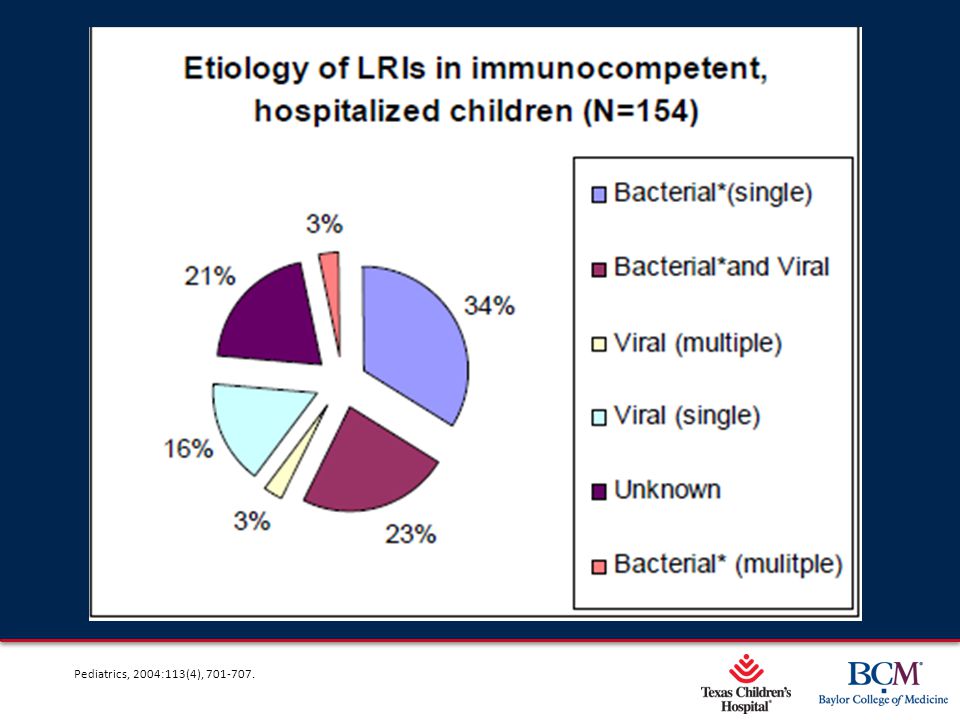
Pediatrics, 2004:113(4),
,")
21
Pleural Effusion small, simple pleural effusions
ampicillin to cover S. pneumoniae. ill-appearing children or those with clinical deterioration vancomycin and cefotaxime. complicated pleural effusion Chest thoracostomy tube (with or without fibrinolytics) or VATS
 or VATS.")
22
Categories of pneumonia
1. Community acquired pneumonia 2. Pneumonia in special populations immunocompromised cystic fibrosis chronically ventilator dependent 3. Ventilator associated pneumonia (VAP) Text xxx00.#####.ppt 4/15/2017 3:37:49 AM
 Text. xxx00.#####.ppt 4/15/2017 3:37:49 AM.")
23
Immunocompromised pt humoral immune deficiencies with accompanying diminished opsonizing capacity functional asplenia, hematopoietic malignancy, transplantation, or immunoglobulin deficiency encapsulated bacteria Streptococcus pneumoniae decreased cell-mediated immunity or macrophage function in patients receiving T-lymphocyte depleting therapies for rheumatologic diseases or inflammatory bowel disease. intracellular organisms (eg, Mycobacteria, Legionella, Nocardia, Strongyloides) infection due to yeasts (eg, Histoplasma, Cryptococcus) or molds (eg, Aspergillus) neutrophil dysfunction* / neutropenia / receiving glucocorticoids and/or T-cell suppression** chronic granulomatous disease* organ transplant recipients who require long-term immune suppression ** Nocardia and nontuberculous mycobacteria
 infection due to yeasts (eg, Histoplasma, Cryptococcus) or molds (eg, Aspergillus) neutrophil dysfunction* / neutropenia / receiving glucocorticoids and/or T-cell suppression** chronic granulomatous disease* organ transplant recipients who require long-term immune suppression ** Nocardia and nontuberculous mycobacteria.")
24
Immunocompromised pt Sequential infection
Ex: viral infection preceding bacterial or fungal infection Multiple simultaneous infections Ex: dual infection with Pneumocystis jirovecii (formerly P. carinii) and cytomegalovirus Disseminated disease (CNS, bones, abdomen) Ex: Aspergillus species, mycobacterial, or Nocardia infections Superimposition of another process (lung injury or drug toxicity) N Engl J Med. 1998;338(24):1741 ;
 and cytomegalovirus. Disseminated disease (CNS, bones, abdomen) Ex: Aspergillus species, mycobacterial, or Nocardia infections. Superimposition of another process (lung injury or drug toxicity) N Engl J Med. 1998;338(24):1741 ; source=search_result&search=pneumonia+in+immunocompromised&selectedTitle=2%7E150.")
25
So… Vanc (at meningitic doses), cefotaxime, zosyn …to start ID consult
Early imaging (CT / MRI) and specific microbiologic diagnoses are essential Invasive procedures (biopsies and bronchoscopy) are often necessary advanced diagnostic testing including immunohistology and quantitative molecular assays Reduction of immune suppression may be as important as antimicrobial therapy in the ultimate success of treatment N Engl J Med. 1998;338(24):1741 ;
 and specific microbiologic diagnoses are essential. Invasive procedures (biopsies and bronchoscopy) are often necessary. advanced diagnostic testing including immunohistology and quantitative molecular assays. Reduction of immune suppression may be as important as antimicrobial therapy in the ultimate success of treatment. N Engl J Med. 1998;338(24):1741 ; source=search_result&search=pneumonia+in+immunocompromised&selectedTitle=2%7E150.")
26
Categories of pneumonia
1. Community acquired pneumonia 2. Pneumonia in special populations immunocompromised cystic fibrosis chronically ventilator dependent 3. Ventilator associated pneumonia (VAP) Text xxx00.#####.ppt 4/15/2017 3:37:49 AM
 Text. xxx00.#####.ppt 4/15/2017 3:37:49 AM.")
27
Simon RH. Cystic fibrosis: Antibiotic therapy for lung disease
Simon RH. Cystic fibrosis: Antibiotic therapy for lung disease. UpToDate

28
Cystic Fibrosis current culture recommendations
perform cultures every three months although the value of antibiotic susceptibility testing based on conventional in vitro cultures has been questioned the correlation between test results and clinical response is poor Am J Infect Control. 2003;31(3 Suppl):S1.; J Pediatr. 2009;155(6 Suppl):S73.
:S1.; J Pediatr. 2009;155(6 Suppl):S73.")
29
Cystic Fibrosis The persistence of bacteria despite aggressive treatment is thought to be due to: Poor penetration of antibiotics into purulent airway secretions Native or acquired antibiotic resistance CF-related defects in mucosal defenses Biofilms produced by the bacteria that may render antibiotics ineffective or interfere with host defenses Simon RH. Cystic fibrosis: Antibiotic therapy for lung disease. UpToDate

30
Clinical indicators to treat?
Increased cough Increased sputum production or chest congestion Decreased exercise tolerance or increased dyspnea with exertion Increased fatigue Decreased appetite Increased respiratory rate or dyspnea at rest Change in sputum appearance Fever (present in a minority of patients) Absenteeism from school or work Increased nasal congestion or drainage J Pediatr. 2001;139(3):359.
 Absenteeism from school or work. Increased nasal congestion or drainage. J Pediatr. 2001;139(3):359.")
31
Treatment considerations
Pseudomonas aeruginosa Chronic infection - an independent risk factor for accelerated loss of pulmonary function and decreased survival Conversion of P. aeruginosa to the mucoid phenotype worsens prognosis Burkholderia cepacia complex Chronic infection - associated with an accelerated decline in pulmonary function and shortened survival in CF Lung transplantation is associated with recurrent and often severe infection, Lung transplantation associated with poor outcomes, particularly for those carrying B. cenocepacia is considered to be a contraindication to transplantation in many centers Pediatr Pulmonol. 2001;32(5):356; Pediatr Pulmonol. 2002;34(2):91; Paediatr Respir Rev. 2002;3(3):230; J Clin Microbiol. 2004;42(12):5537; Am J Respir Crit Care Med. 2006;173(4):421
:356; Pediatr Pulmonol. 2002;34(2):91; Paediatr Respir Rev. 2002;3(3):230; J Clin Microbiol. 2004;42(12):5537; Am J Respir Crit Care Med. 2006;173(4):421.")
32
Treatment considerations
treat any S. aureus treat Achromobacter xylosoxidans Some isolates can be particularly inflammatory and are associated with rates of FEV1 deterioration uncertainty regarding the importance of treating Stenotrophomonas maltophilia (S. maltophilia) merely a marker of more severe lung disease or a cause of it? Aspergillus species are generally not treated appear to be an unlikely cause of pulmonary exacerbations Simon RH. Cystic fibrosis: Antibiotic therapy for lung disease. UpToDate
 merely a marker of more severe lung disease or a cause of it Aspergillus species are generally not treated. appear to be an unlikely cause of pulmonary exacerbations. Simon RH. Cystic fibrosis: Antibiotic therapy for lung disease. UpToDate. source=search_result&search=cystic+fibrosis+and+pneumonia&selectedTitle=1%7E150.")
33
Treatment considerations
When in vitro testing can identify no antibiotic to which a bacterium is susceptible, select a combination of antibiotics that would otherwise be chosen empirically for that pathogen. generally avoid using two beta lactam antibiotics simultaneously based upon in vitro studies showing the antimicrobial effect of adding the second beta lactam is unpredictable and can sometimes be antagonistic to the first continue administering oral azithromycin during the acute exacerbation if it is a component of the chronic pulmonary regimen. Simon RH. Cystic fibrosis: Antibiotic therapy for lung disease. UpToDate

34
Simon RH. Cystic fibrosis: Antibiotic therapy for lung disease
Simon RH. Cystic fibrosis: Antibiotic therapy for lung disease. UpToDate

35
Antibiotic synergy testing
The only large clinical trial that studied the effect of combination antibiotic susceptibility testing failed to demonstrate any benefit associated with this approach Meta analysis: Combination antibiotic susceptibility testing did not improve clinical or bacteriologic outcomes did not prolong the period until the next acute exacerbation The reason to bring this up.. It is difficult to arrange (goes to Canada) and requires quite a bit of time for the isolates to grow (so not a quick turn around). Not saying not to do it at all but when asked by a distraught parent this info could assuage some concerns Lancet. 2005;366(9484):463; Cochrane Database Syst Rev. 2008 xxx00.#####.ppt 4/15/2017
 and requires quite a bit of time for the isolates to grow (so not a quick turn around). Not saying not to do it at all but when asked by a distraught parent this info could assuage some concerns. Lancet. 2005;366(9484):463; Cochrane Database Syst Rev xxx00.#####.ppt 4/15/2017.")
36
Categories of pneumonia
1. Community acquired pneumonia 2. Pneumonia in special populations immunocompromised cystic fibrosis chronically ventilator dependent 3. Ventilator associated pneumonia (VAP) Text xxx00.#####.ppt 4/15/2017 3:37:49 AM
 Text. xxx00.#####.ppt 4/15/2017 3:37:49 AM.")
37
Ventilator-dependent children
tracheostomy tubes bypass the protection of the nose, mouth, and upper airway the tube may result in various degrees of ulceration and tracheal denudation a humidified circuit results in colonization of the trachea aspirates show an average of six isolates per specimen, and the mean bacterial concentration was 107 organisms / ml In 1976: most frequent aerobic isolates - S. pneumoniae and S. aureus. predominant anaerobes - gram-positive cocci, F. nucleatum, and B. fragilis. replacement of one pathogen by another occurs frequently In 2010: gram-negative rods accounted for 71% of microorganisms Ann Otol Rhinol Laryngol, 74 (1965), pp. 785–798; Chest, 85 (1984), pp. 39–44; Chest, 76 (1979), pp. 420–424 ; Chest, 74 (1978), pp. 635–639
, pp. 785–798; Chest, 85 (1984), pp. 39–44; Chest, 76 (1979), pp. 420–424 ; Chest, 74 (1978), pp. 635–639.")
38
Ventilator-dependent children
Tracheitis v tracheobronchitis v pneumonia? colonization v real infection? culture material via tracheal aspirate suction trap, BAL, blind protected telescoping catheter (miniBAL)? quantitative cultures, semi-quantitative? No correlation found between the concentrations of polymorphonuclear leukocytes and quantitative bacterial counts Chest, 74 (1978), pp. 635–639; CHEST 1979: 76: ; CHEST 2013; 144(1):32–38; Pediatr Pulmonol. 2012; 47:409–414; Ped Crit Care Med Jan;9(1):96-100;
 quantitative cultures, semi-quantitative No correlation found between the concentrations of polymorphonuclear leukocytes and quantitative bacterial counts. Chest, 74 (1978), pp. 635–639; CHEST 1979: 76: ; CHEST 2013; 144(1):32–38; Pediatr Pulmonol. 2012; 47:409–414; Ped Crit Care Med Jan;9(1):96-100;")
39
Ventilator-dependent children
following trach placement 40% readmitted within 12 months 45% pneumonia / tracheitis clinical indicators oxygen saturations declined secretions changed in color, viscosity, or odor Increased need for airway suctioning Increased need for oxygen supplementation or ventilatory support new infiltrates or opacities on chest radiographs evidence-based guidelines lacking treat based on prior cultures or current gram stain Chest, 74 (1978), pp. 635–639; CHEST 1979: 76: ; CHEST 2013; 144(1):32–38; Pediatr Pulmonol. 2012; 47:409–414; Ped Crit Care Med Jan;9(1):96-100; Semin Pediatr Infect Dis 2006:17:11.
, pp. 635–639; CHEST 1979: 76: ; CHEST 2013; 144(1):32–38; Pediatr Pulmonol. 2012; 47:409–414; Ped Crit Care Med Jan;9(1):96-100; Semin Pediatr Infect Dis 2006:17:11.")
40
Categories of pneumonia
1. Community acquired pneumonia 2. Pneumonia in special populations immunocompromised cystic fibrosis chronically ventilator dependent 3. Ventilator associated pneumonia (VAP) Ventilator associated condition Text X xxx00.#####.ppt 4/15/2017 3:37:49 AM
 Ventilator associated condition. Text. X. xxx00.#####.ppt 4/15/2017 3:37:49 AM.")
41
Ventilator Associated Pneumonia (VAP)
The second most common hospital associated infection Accounts for 20% nosocomial infections in PICU’s Increased morbidity for patients Increased length of stay in the hospital Increased cost trach /vent dependent kids sig more likely to develop a VAT Text CHEST 2013; 144(1):32–38 xxx00.#####.ppt 4/15/2017 3:37:49 AM
:32–38. xxx00.#####.ppt 4/15/2017 3:37:49 AM.")
42
VAP clinical criteria for VAP are subjective and nonspecific:
worsening oxygenation change in the quality or quantity of sputum production new or progressive infiltrates from our AQI project - On 4 consecutive days, 4 different radiologists read the films and used 4 different words/phrases to describe the same thing autopsy series reveal that 1/3 to ½ of patients who met clinical criteria for VAP did not have pneumonia. CDC working group - shift the focus of surveillance from pneumonia alone to complications of mechanical ventilation in general. Text The Joint Commission Journal on Quality and Patient Safety 2008: 34(11) 629. xxx00.#####.ppt 4/15/2017 3:37:49 AM
 629. xxx00.#####.ppt 4/15/2017 3:37:49 AM.")
43
Text NEJM 2013:368;16 xxx00.#####.ppt 4/15/2017 3:37:49 AM

44
VAC – new definitions do not include radiographic criteria
reflects the recognition that they are counterproductive in surveillance definitions because they introduce substantial complexity and subjectivity without increasing accuracy opportunity to identify a population of patients who have serious complications that have previously not been acknowledged or attended to by quality-improvement programs will enable hospitals to benchmark their rates against peer institutions in a more meaningful way Antibiotic stewardship - the inclusion of an antibiotic criterion in the definition of IVAC will provide hospitals with a routine, widely reportable benchmark for the prescribing of antibiotics in their ICUs Text xxx00.#####.ppt 4/15/2017 3:37:49 AM

45
VAC in pediatrics Of 645 mechanically ventilated patients admitted, 22 (3.4%) met criteria for VAC - incidence 0.829%, lower than the 2.3% to 11.5% reported in adult studies Patients with VAC experienced - a significantly longer mean length of stay in the PICU ( days vs days; P ) and higher mean total ventilator time ( h vs h; P ). significant association between tracheostomy and VAC ( P < .000) and between chronic ventilator dependence and VAC ( P < .002). cultured microorganisms: Gram-negative rods 71%; staphylococcal or streptococcal species 26% Of those with two or more potentially causative pathogens - 67% (n=4) were in patients with a tracheostomy CHEST 2013; 144(1):32–38
 met criteria for VAC - incidence 0.829%, lower than the 2.3% to 11.5% reported in adult studies. Patients with VAC experienced - a significantly longer mean length of stay in the PICU ( days vs days; P ) and higher mean total ventilator time ( h vs h; P ). significant association between tracheostomy and VAC ( P < .000) and between chronic ventilator dependence and VAC ( P < .002). cultured microorganisms: Gram-negative rods 71%; staphylococcal or streptococcal species 26% Of those with two or more potentially causative pathogens - 67% (n=4) were in patients with a tracheostomy. CHEST 2013; 144(1):32–38.")
46
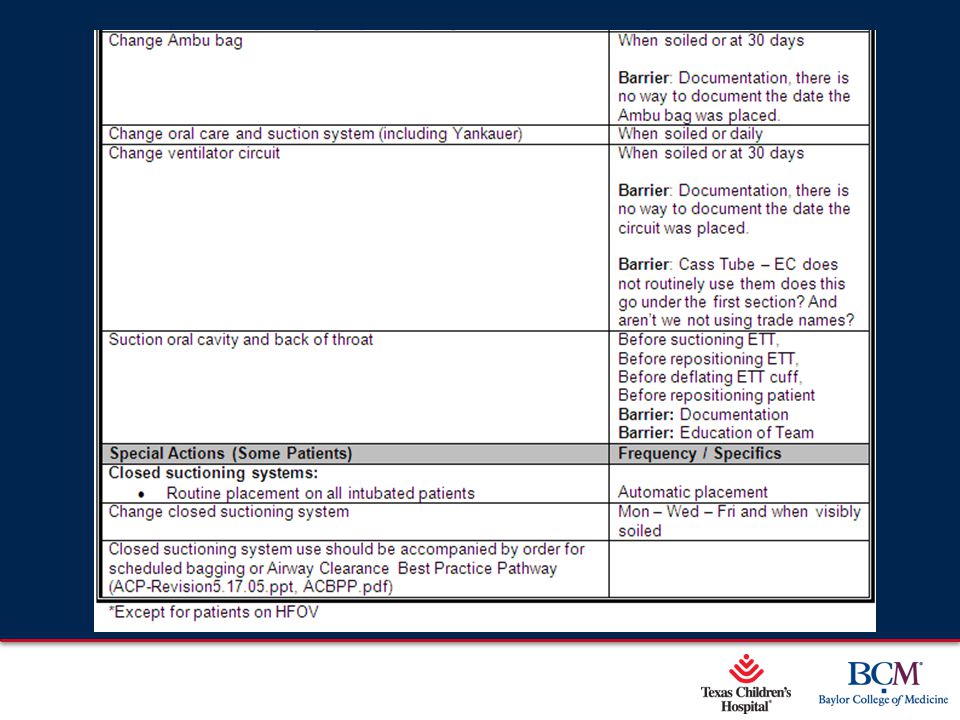
Prevention bundled care!

47
Text xxx00.#####.ppt 4/15/2017 3:37:49 AM

48
Text xxx00.#####.ppt 4/15/2017 3:37:49 AM

50
References: Virkki R, Juven T, Rikalainen H, Svedström E, Mertsola J, Ruuskanen O. Differentiation of bacterial and viral pneumonia in children. Thorax ;57(5):438. Tan TQ, Mason EO Jr, Barson WJ, Wald ER, Schutze GE, Bradley JS, Arditi M, Givner LB, Yogev R, Kim KS, Kaplan SL. Clinical characteristics and outcome of children with pneumonia attributable to penicillin-susceptible and penicillin-nonsusceptible Streptococcus pneumoniae. Pediatrics. 1998;102(6):1369. Finnegan OC, Fowles SJ, White RJ. Radiographic appearances of mycoplasma pneumonia. Thorax. 1981;36(6):469. Korppi M, Kiekara O, Heiskanen-Kosma T, Soimakallio S. Comparison of radiological findings and microbial aetiology of childhood pneumonia. Acta Paediatr. 1993;82(4):360. Simpson W, Hacking PM, Court SD, Gardner PS. The radiological findings in respiratory syncytial virus infection in children. II. The correlation of radiological categories with clinical and virological findings. Pediatr Radiol. 1974;2(3):155. Dawson KP, Long A, Kennedy J, Mogridge N. The chest radiograph in acute bronchiolitis. J Paediatr Child Health. 1990;26(4):209. Bachur R, Perry H, Harper MB. Occult pneumonias: empiric chest radiographs in febrile children with leukocytosis. Ann Emerg Med ;33(2):166. Margolis P, Gadomski A. The rational clinical examination. Does this infant have pneumonia? JAMA. 1998;279(4):308. Klompas M. Complications of Mechanical Ventilation — The CDC’s New Surveillance Paradigm. NEJM 2013:368;16 Meyers, J., Shook, J., Pella, J., & Cron, S. G. Complete respiratory assessment score accurately predicts outcomes in children with acute reactive airway disease exacerbations [Abstract]. Academic Emergency Medicine, 1996: 3(5), 396. Rosenfeld M, Gibson RL, McNamara S, Emerson J, Burns JL, Castile R, Hiatt P, McCoy K, Wilson CB, Inglis A, Smith A, Martin TR, Ramsey BW. Early pulmonary infection, inflammation, and clinical outcomes in infants with cystic fibrosis. Pediatr Pulmonol. 2001;32(5):356.
:438. Tan TQ, Mason EO Jr, Barson WJ, Wald ER, Schutze GE, Bradley JS, Arditi M, Givner LB, Yogev R, Kim KS, Kaplan SL. Clinical characteristics and outcome of children with pneumonia attributable to penicillin-susceptible and penicillin-nonsusceptible Streptococcus pneumoniae. Pediatrics. 1998;102(6):1369. Finnegan OC, Fowles SJ, White RJ. Radiographic appearances of mycoplasma pneumonia. Thorax. 1981;36(6):469. Korppi M, Kiekara O, Heiskanen-Kosma T, Soimakallio S. Comparison of radiological findings and microbial aetiology of childhood pneumonia. Acta Paediatr. 1993;82(4):360. Simpson W, Hacking PM, Court SD, Gardner PS. The radiological findings in respiratory syncytial virus infection in children. II. The correlation of radiological categories with clinical and virological findings. Pediatr Radiol. 1974;2(3):155. Dawson KP, Long A, Kennedy J, Mogridge N. The chest radiograph in acute bronchiolitis. J Paediatr Child Health. 1990;26(4):209. Bachur R, Perry H, Harper MB. Occult pneumonias: empiric chest radiographs in febrile children with leukocytosis. Ann Emerg Med. 1999;33(2):166. Margolis P, Gadomski A. The rational clinical examination. Does this infant have pneumonia JAMA. 1998;279(4):308. Klompas M. Complications of Mechanical Ventilation — The CDC’s New Surveillance Paradigm. NEJM 2013:368;16. Meyers, J., Shook, J., Pella, J., & Cron, S. G. Complete respiratory assessment score accurately predicts outcomes in children with acute reactive airway disease exacerbations [Abstract]. Academic Emergency Medicine, 1996: 3(5), 396. Rosenfeld M, Gibson RL, McNamara S, Emerson J, Burns JL, Castile R, Hiatt P, McCoy K, Wilson CB, Inglis A, Smith A, Martin TR, Ramsey BW. Early pulmonary infection, inflammation, and clinical outcomes in infants with cystic fibrosis. Pediatr Pulmonol. 2001;32(5):356.")
51
References cont Emerson J, Rosenfeld M, McNamara S, Ramsey B, Gibson RL. Pseudomonas aeruginosa and other predictors of mortality and morbidity in young children with cystic fibrosis. Pediatr Pulmonol. 2002;34(2):91. Speert DP. Advances in Burkholderia cepacia complex. Paediatr Respir Rev. 2002;3(3):230. Fauroux B, Hart N, Belfar S, BouléM, Tillous-Borde I, Bonnet D, Bingen E, Clément A. Burkholderia cepacia is associated with pulmonary hypertension and increased mortality among cystic fibrosis patients. J Clin Microbiol. 2004;42(12):5537. Kalish LA, Waltz DA, Dovey M, Potter-Bynoe G, McAdam AJ, Lipuma JJ, Gerard C, Goldmann D. Impact of Burkholderia dolosa on lung function and survival in cystic fibrosis. Am J Respir Crit Care Med. 2006;173(4):421. Rosenfeld M, Emerson J, Williams-Warren J, Pepe M, Smith A, Montgomery AB, Ramsey B. Defining a pulmonary exacerbation in cystic fibrosis. J Pediatr. 2001;139(3):359. Aaron SD, Vandemheen KL, Ferris W, Fergusson D, Tullis E, Haase D, Berthiaume Y, Brown N, Wilcox P, Yozghatlian V, Bye P, Bell S, Chan F, Rose B, Jeanneret A, Stephenson A, Noseworthy M, Freitag A, Paterson N, Doucette S, Harbour C, Ruel M, MacDonald N. Combination antibiotic susceptibility testing to treat exacerbations of cystic fibrosis associated with multiresistant bacteria: a randomised, double-blind, controlled clinical trial. Lancet. 2005;366(9484):463. Waters V, Ratjen F. Combination antimicrobial susceptibility testing for acute exacerbations in chronic infection of Pseudomonas aeruginosa in cystic fibrosis. Cochrane Database Syst Rev. 2008 Simon RH. Cystic fibrosis: Antibiotic therapy for lung disease. UpToDate (found at: therapy-for-lung-disease?source=search_result&search=cystic+fibrosis+and+pneumonia&selectedTitle=1%7E150) Saiman L, Siegel J, Cystic Fibrosis Foundation Consensus Conference on Infection Control Participants. Infection control recommendations for patients with cystic fibrosis: Microbiology, important pathogens, and infection control practices to prevent patient-to-patient transmission. Am J Infect Control. 2003;31(3 Suppl):S1.
:91. Speert DP. Advances in Burkholderia cepacia complex. Paediatr Respir Rev. 2002;3(3):230. Fauroux B, Hart N, Belfar S, BouléM, Tillous-Borde I, Bonnet D, Bingen E, Clément A. Burkholderia cepacia is associated with pulmonary hypertension and increased mortality among cystic fibrosis patients. J Clin Microbiol. 2004;42(12):5537. Kalish LA, Waltz DA, Dovey M, Potter-Bynoe G, McAdam AJ, Lipuma JJ, Gerard C, Goldmann D. Impact of Burkholderia dolosa on lung function and survival in cystic fibrosis. Am J Respir Crit Care Med. 2006;173(4):421. Rosenfeld M, Emerson J, Williams-Warren J, Pepe M, Smith A, Montgomery AB, Ramsey B. Defining a pulmonary exacerbation in cystic fibrosis. J Pediatr. 2001;139(3):359. Aaron SD, Vandemheen KL, Ferris W, Fergusson D, Tullis E, Haase D, Berthiaume Y, Brown N, Wilcox P, Yozghatlian V, Bye P, Bell S, Chan F, Rose B, Jeanneret A, Stephenson A, Noseworthy M, Freitag A, Paterson N, Doucette S, Harbour C, Ruel M, MacDonald N. Combination antibiotic susceptibility testing to treat exacerbations of cystic fibrosis associated with multiresistant bacteria: a randomised, double-blind, controlled clinical trial. Lancet. 2005;366(9484):463. Waters V, Ratjen F. Combination antimicrobial susceptibility testing for acute exacerbations in chronic infection of Pseudomonas aeruginosa in cystic fibrosis. Cochrane Database Syst Rev Simon RH. Cystic fibrosis: Antibiotic therapy for lung disease. UpToDate (found at: therapy-for-lung-disease source=search_result&search=cystic+fibrosis+and+pneumonia&selectedTitle=1%7E150) Saiman L, Siegel J, Cystic Fibrosis Foundation Consensus Conference on Infection Control Participants. Infection control recommendations for patients with cystic fibrosis: Microbiology, important pathogens, and infection control practices to prevent patient-to-patient transmission. Am J Infect Control. 2003;31(3 Suppl):S1.")
52
References con’t Cystic Fibrosis Foundation, Borowitz D, Robinson KA, Rosenfeld M, Davis SD, Sabadosa KA, Spear SL, Michel SH, Parad RB, White TB, Farrell PM, Marshall BC, Accurso FJ. Cystic Fibrosis Foundation evidence-based guidelines for management of infants with cystic fibrosis. J Pediatr ;155(6 Suppl):S73. Brook I. Bacterial Colonization, Tracheobronchitis, and Pneumonia following Tracheostomy and Long-Term Intubation in Pediatric Patients. CHEST 1979: 76: Simpson VS, Bailey A, Higgerson RA and Christie L M. Ventilator-Associated Tracheobronchitis in a Mixed Medical/Surgical Pediatric ICU. CHEST 2013; 144(1):32–38 Nseir S, Di Pompeo C, Soubrier S, et al . Effect of ventilatorassociated tracheobronchitis on outcome in patients without chronic respiratory failure: a case-control study . Crit Care 2005 ; 9 ( 3 ): R238 - R245 . Agrafi otis M Siempos II, Falagas ME . Frequency, prevention, outcome and treatment of ventilator-associated tracheobronchitis: systematic review and meta-analysis . Respir Med ; 104 ( 3 ): Dallas J, Skrupky L, Abebe N, Boyle WA III, Kollef MH . Ventilator-associated tracheobronchitis in a mixed surgical and medical ICU population . Chest ; 139 ( 3 ): Kun SS, Edwards JD, Davidson Ward SL, Keens TG. Hospital Readmissions for Newly Discharged Pediatric Home Mechanical Ventilation Patients. Pediatr Pulmonol. 2012; 47:409–414. Graf JM, Montagnino BA, Hueckel R, McPherson ML. Pediatric tracheostomies: a recent experience from one academic center. Ped Crit Care Med Jan;9(1): Fishman JA. Pulmonary infections in immunocompromised patients. Found at: immunocompromised-patients?source=search_result&search=pneumonia+in+immunocompromised&selectedTitle=2%7E150 Fishman JA, Rubin RH. Infection in organ-transplant recipients. N Engl J Med. 1998;338(24):1741.
:S73. Brook I. Bacterial Colonization, Tracheobronchitis, and Pneumonia following Tracheostomy and Long-Term Intubation in Pediatric Patients. CHEST 1979: 76: Simpson VS, Bailey A, Higgerson RA and Christie L M. Ventilator-Associated Tracheobronchitis in a Mixed Medical/Surgical Pediatric ICU. CHEST 2013; 144(1):32–38. Nseir S, Di Pompeo C, Soubrier S, et al . Effect of ventilatorassociated tracheobronchitis on outcome in patients without chronic respiratory failure: a case-control study . Crit Care 2005 ; 9 ( 3 ): R238 - R245 . Agrafi otis M Siempos II, Falagas ME . Frequency, prevention, outcome and treatment of ventilator-associated tracheobronchitis: systematic review and meta-analysis . Respir Med ; 104 ( 3 ): Dallas J, Skrupky L, Abebe N, Boyle WA III, Kollef MH . Ventilator-associated tracheobronchitis in a mixed surgical and medical ICU population . Chest ; 139 ( 3 ): Kun SS, Edwards JD, Davidson Ward SL, Keens TG. Hospital Readmissions for Newly Discharged Pediatric Home Mechanical Ventilation Patients. Pediatr Pulmonol. 2012; 47:409–414. Graf JM, Montagnino BA, Hueckel R, McPherson ML. Pediatric tracheostomies: a recent experience from one academic center. Ped Crit Care Med Jan;9(1): Fishman JA. Pulmonary infections in immunocompromised patients. Found at: immunocompromised-patients source=search_result&search=pneumonia+in+immunocompromised&selectedTitle=2%7E150. Fishman JA, Rubin RH. Infection in organ-transplant recipients. N Engl J Med. 1998;338(24):1741.")
53
Bradley, J. S. , Byington, C. L. , Shah, S. S. , Alverson, B
Bradley, J. S., Byington, C. L., Shah, S. S., Alverson, B., Carter, E. R., Harrison, C., et al.. The management of communityacquired pneumonia in infants and children older than 3 months of age: Clinical practice guidelines by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America. Clinical Infectious Diseases 2011: 53(7), e25-e76. Michelow, I. C., Olsen, K., Lozano, J., Rollins, N. K., Duffy, L. B., Ziegler, T., et al. (2004). Epidemiology and clinical characteristics of communityacquired pneumonia in hospitalized children. Pediatrics, 2004:113(4), S.A. Friedberg, T.E. Griffith, G.M. Hass. Histologic changes in the trachea following tracheostomy. Ann Otol Rhinol Laryngol, 74 (1965), pp. 785– 798 M.S. Niederman, R.D. Ferranti, A. Zeigler et al. Respiratory infection complicating long term tracheostomy. The implication of persistent gram- negative tracheobronchial colonization. Chest, 85 (1984), pp. 39–44 J.G. Barlett, L.G. Faling, S. Willey. Quantitative Tracheal bacteriologic and cytologic studies in patients with long term tracheostomies. Chest, 74 (1978), pp. 635–639 Graf J, Stein F. Tracheitis in pediatric patients. Semin Pediatr Infect Dis 2006:17:11. Brilli RJ, Sparling KW, Lake MR, Butcher J, Myers, SS, Clark MD, Helpling A, Stutler ME.The Business Case for Preventing Ventilator-Associated Pneumonia in Pediatric Intensive Care Unit Patients. The Joint Commission Journal on Quality and Patient Safety 2008: 34(11) 629.
, e25-e76. Michelow, I. C., Olsen, K., Lozano, J., Rollins, N. K., Duffy, L. B., Ziegler, T., et al. (2004). Epidemiology and clinical characteristics of communityacquired pneumonia in hospitalized children. Pediatrics, 2004:113(4), S.A. Friedberg, T.E. Griffith, G.M. Hass. Histologic changes in the trachea following tracheostomy. Ann Otol Rhinol Laryngol, 74 (1965), pp. 785– 798. M.S. Niederman, R.D. Ferranti, A. Zeigler et al. Respiratory infection complicating long term tracheostomy. The implication of persistent gram- negative tracheobronchial colonization. Chest, 85 (1984), pp. 39–44. J.G. Barlett, L.G. Faling, S. Willey. Quantitative Tracheal bacteriologic and cytologic studies in patients with long term tracheostomies. Chest, 74 (1978), pp. 635–639. Graf J, Stein F. Tracheitis in pediatric patients. Semin Pediatr Infect Dis 2006:17:11. Brilli RJ, Sparling KW, Lake MR, Butcher J, Myers, SS, Clark MD, Helpling A, Stutler ME.The Business Case for Preventing Ventilator-Associated Pneumonia in Pediatric Intensive Care Unit Patients. The Joint Commission Journal on Quality and Patient Safety 2008: 34(11) 629.")
Similar presentations














>")






, and the parenchyma.>")
