Download presentation
Presentation is loading. Please wait.

1
ADHESIVE CAPSULITIS THANATHEP TANPOWPONG ASSISTANT PROFESSOR CHULALONGKORN UNIVERSITY

2
“difficult to define difficult to treat difficult to explain” Codman

3
Codman first define “frozen shoulder” 1945 : Nevaiser describe pathological lesion of fibrosis, inflammation and capsular contracture

4
Prevalence 2-3% of population (Female) 40-60 year Non-dominant hand 20-30% involve opposite side
 year Non-dominant hand 20-30% involve opposite side")
5
Etilogy Unknown – Trauma – Inflammation (TGF-β) – Associate with diabetes, thyroid dysfunction, Dupuytrens contracture, autoimmune disease, treatment of breast cancer, cerebrovascular accident, MI
 – Associate with diabetes, thyroid dysfunction, Dupuytrens contracture, autoimmune disease, treatment of breast cancer, cerebrovascular accident, MI")
6
Diagnosis Primary : idiopathic process, global capsular inflammation and fibrosis Secondary : known injury or disesase prior to adhesion

7
62% of idiopathic adhesive capsulitis were found to have partial thickness tear of supraspinatus Yoo et al Orthapaedics. 2009;32(1):22
:22.")
8
Staging (Neviaser et al CORR 1987) SymptomSignFinding 1painFull ROM under GAsynovitis 2Severe night pain, early stiff Stiff (external rotation)Christmas tree synovitis 3Stiff, pain at end of motion Significant loss motionMinimal synovitis,loss axillary fold 4Profound stiff, minimal pain Motion loss but start to improve Difficult to identify joint
 SymptomSignFinding 1painFull ROM under GAsynovitis 2Severe night pain, early stiff Stiff (external rotation)Christmas tree synovitis 3Stiff, pain at end of motion Significant loss motionMinimal synovitis,loss axillary fold 4Profound stiff, minimal pain Motion loss but start to improve Difficult to identify joint")
9
Stage 1 – Pain, stiff – Gain full ROM after GA or intra-articular anesthetic injection – Duration 3 month

10
Stage 2 (freezing) – Progressive capsular contracture – Limit ROM (not fully recovered) – “Christmas tree appearance”
 – Progressive capsular contracture – Limit ROM (not fully recovered) – Christmas tree appearance")
11
Acknowledgement to Neviaser AMJ Sport 2010;38:2346

12
Stage 3 (frozen) – Progressive loss of motion – Not improve after intraarticular anesthetic injection – Duration 9-15month
 – Progressive loss of motion – Not improve after intraarticular anesthetic injection – Duration 9-15month")
13
Stage 4 (thawing) – Minimal pain – Gradual improve ROM – Fully mature adhesion – Difficult to identify intra-articular structure during arthroscope
 – Minimal pain – Gradual improve ROM – Fully mature adhesion – Difficult to identify intra-articular structure during arthroscope")
14
Natural history No true study of natural history Self-limiting Grey: complete recovery in 2 years Miller: normal function and minimal pain after home therapy 4 year after home therapy JBJS Am 1978;60(4):564 Orthopaedics 1996;19(10):849-853
:564 Orthopaedics 1996;19(10):")
15
94% of idiopathic frozen shoulder recover to normal level, range of motion, function without treatment Vastamaki et al CORR 2012;470(4):1133.43
:")
16
TREATMENT Address underlying pathology Treatment according to clinical stage at presentation

17
NSAIDs Theoretical benefit No level I or II study to prove effectiveness Improve pain but not improve motion Cox-2 have comparable efficacy compare to Cox-1 ( better night pain control) Rhind Rhumatol Rehabil 1982;21(1):51-53 Duke Rhumatol Rehabil 1981;20(1):54-59 Otha et al. Mod Rhumatolol. Feb 2013

18
Oral steroid Provide rapid relief of pain (similar to intraarticular steroid injection) but not sustain at long term Possible long term systemic effects Not recommend Buchbinder Ann Rhum Dis 2004;63(11):1460-1469
 but not sustain at long term Possible long term systemic effects Not recommend Buchbinder Ann Rhum Dis 2004;63(11):")
19
Intra-articular steroid injection Rizk et al : transient (2-3 week) improvement of pain compare to placebo Bulgen et al : improve pain and motion in 4 weeks Arch Phys Med Rehabil 1991;72(1):20-22 Ann Rheum Dis 1984;43(3):353-360
 improvement of pain compare to placebo Bulgen et al : improve pain and motion in 4 weeks Arch Phys Med Rehabil 1991;72(1):20-22 Ann Rheum Dis 1984;43(3):")
20
Van der Windt – 109 patient – 40 mg of triamcinolone vs physical therapy 2/wks – 2.2 injection/6 weeks – Passive joint motion, exercise, ice, hot, electrotherapy – 1 year follow up – Self-assessment and functional score – 77% success in injection group vs 46% in physical therapy group BMJ 1998;317(7168):1292-1296
:")
21
Intraarticular steroid injection gives better result in early stage of disease Stage 1recover in 6 weeks Stage 2 recover in 7 months Marx HHS J 2007;3(2):202-207
:")
22
Physical therapy Most consistently prescribe for latter stage Cochrane database review – Little overall evidence (4/26) – No evidence that physiotherapy alone is of benefit in adhesive capsulitis Cochrane Database Syst Rev 2003;(2):CD004258
 – No evidence that physiotherapy alone is of benefit in adhesive capsulitis Cochrane Database Syst Rev 2003;(2):CD004258")
23
Carette and Bulgen found no difference between physiotherapy and no treatment (control group)—level I study – Low number of participants Arthritis Rheum 2003;48(3):829-838 Ann Rhum Dis 1984;43(3):353-360
—level I study – Low number of participants Arthritis Rheum 2003;48(3): Ann Rhum Dis 1984;43(3):")
24
Level I study by Vermeulen – Low grade mobilization have little difference compare with high grade technique – Low grade : movement with in pain free zone – High grade: movement into stiff and painful range – “reflex muscle acivity” Phys Ther 2006;86(3):355-368
:")
25
Surgical intervention In most series 10% of patients do not respond to non-operative treatment

26
Surgical intervention 1.Suprascapular nerve blocks 2.Hydrodilation 3.Manipulation under anesthesia 4.Arthroscopic release 5.Open release

27
Suprascapular nerve block – Unclear therapeutic mechanism – Disruption of efferent and afferent pain signaling – May normalization pathological and neurological process – Insufficient data to prove it’s efficacy

28
Hydrodilation (Brisement) – Increase intracapsular pressure until rupture – Compare hydrodilation with MUA No diiference in ROM Better Constant and VAS score – Small number of trials to proof it’s efficacy Quraishi JBJS Br. 2007;89(9):1197-1200
:")
29
Manipulation (MUA) MUA vs home exercise (level II) – Slight better moblility at 3 month – No difference in 6 and 12 month MUA have effect of improve motion and pain relief for approx 23 years Kivimaki J Shoulder Elbow Surg 2007;16(6):722-726 CORR 2013;471(4):1245-50
 MUA vs home exercise (level II) – Slight better moblility at 3 month – No difference in 6 and 12 month MUA have effect of improve motion and pain relief for approx 23 years Kivimaki J Shoulder Elbow Surg 2007;16(6): CORR 2013;471(4):")
30
Arthroscopic release Advantage – Accurate and complete – Ability to perform synovectomy – Improve mobility of musculotendinous unit compare with open surgery – Minimal pain – Identify intrinsic pathology – Post operative motion can be done immidiately

31
Contraindication – Unable to cooperate postoperative program – Pateint cannot tolerate stress from fluid challenge (renal or cardiac failure)
")
32
Surgical technique Release rotator interval, SGHL

33
MGHL

34
Posterior capsular release

35
Release axillary pouch and IGHL (multiple perforation or direct cut)
")
36
My practice Stage 3 or 4 No intraarticular steroid are injected Jackin’s exercise (low grade) Nsaids prior and ice after If 3-6 month not improve MUA or scope release
 Nsaids prior and ice after If 3-6 month not improve MUA or scope release")
37
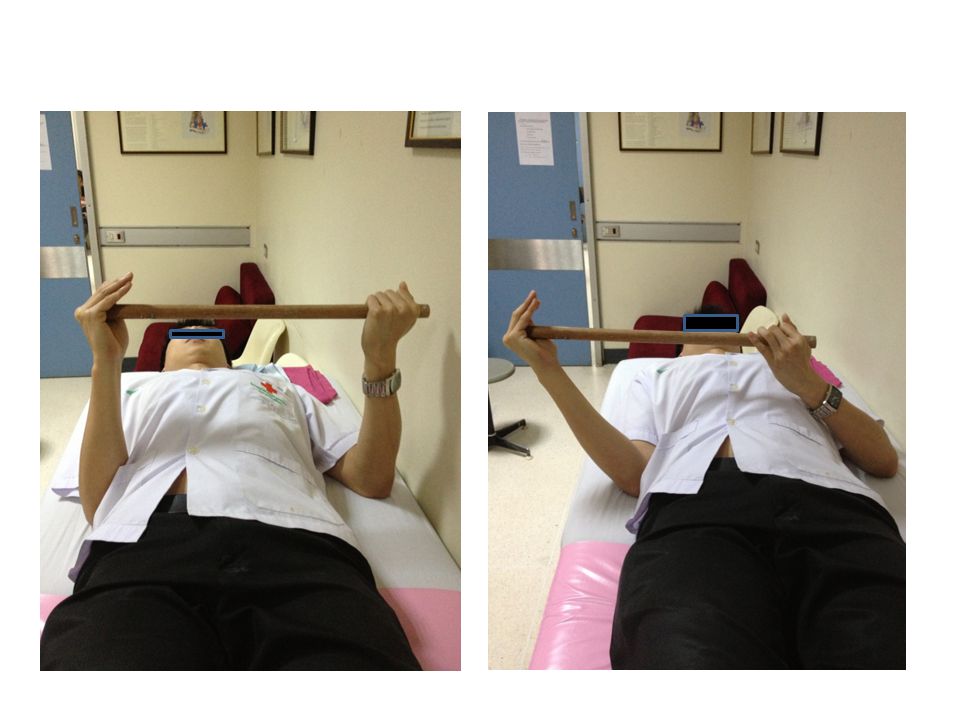
Jackin’s exercise program Each 4 position are perform 10 times/round 5 round/day

41
Post operative protocol – Regional nerve block ( interscalene, SSN, brachial) – Immediate post-op : pendulum exercise – Passive stretching ( Forward flexion, IR, ER, ABD) – 2 times/day, 15 minutes/session – Follow up: post-op week 1,2,4,6,8
 – Immediate post-op : pendulum exercise – Passive stretching ( Forward flexion, IR, ER, ABD) – 2 times/day, 15 minutes/session – Follow up: post-op week 1,2,4,6,8")
42
Thank you

Similar presentations

















>")



