Download presentation
Presentation is loading. Please wait.

1
Leukaemia

2
* Definition of leukemia:
Leukemia is malignant proliferation of hematopoietic cells in the bone marrow followed by blood dissemination and soft tissue infiltration. Leukemic cells produce symptoms because of: Bone marrow failure (i.e. anemia, neutropenia, thrombocytopenia). Infiltration of body organs (e.g. liver, spleen, lymph nodes, meninges, brain, skin or testes).
. Infiltration of body organs (e.g. liver, spleen, lymph nodes, meninges, brain, skin or testes).")
3
* Classification of leukemia:
1. Acute Leukemia: Acute lymphoblastic leukemia (ALL): L1 – L3. Acute myeloblastic leukemia: (AML): M0 – M7. 2. Chronic Leukemia: Chronic lymphocytic leukemia (CLL). Chronic myelocytic leukemia (CML).
: L1 – L3. Acute myeloblastic leukemia: (AML): M0 – M7. 2. Chronic Leukemia: Chronic lymphocytic leukemia (CLL). Chronic myelocytic leukemia (CML).")
4
* Etiology of leukemia:
1. Congenital disorder: Down syndrome, Immunodeficiency syndrome. 2. Ionizing radiation: X-ray, radiotherapy. 3. Chemicals: (alkylating agent, Benzene). 4. Viruses: Human T-lymphocyte leukemia virus (HTLV1), EBV.
. 4. Viruses: Human T-lymphocyte leukemia virus (HTLV1), EBV.")
5
Lymph node infiltration is common in leukaemia of lymphocytic origin e
Lymph node infiltration is common in leukaemia of lymphocytic origin e.g. acute lymphoblastic leukaemia and chronic lymphocytic leukaemia.

6
* Clinical features of ALL:
The disease affects children. Pallor, lethargy, malaise and dyspnea due to anaemia. Fever, malaise, features of mouth, skin, respiratory infections due to neutropenia. Spontaneous bruises, pupura, bleeding gums due to thrombocytopenia. Generalized lymphadenopathy. Hepatomegaly. Splenomegaly. Organ infiltration: Bony infiltration. Testicular infiltration. C.N.S. infiltration. Fever.

7
* Laboratory Investigations of ALL:
1. CBC: ↑↑ WBCs with lymphoblasts in the peripheral blood. RBCs: ↓ (anaemia). Platelets: ↓ 2. Bone marrow: BM Aspirate: - All normal marrow elements are depressed and replaced by abnormal blast cells.
. Platelets: ↓ 2. Bone marrow: BM Aspirate: - All normal marrow elements are depressed and replaced by abnormal blast cells.")
8
ALL: Lymphoblasts have condensed chromatin, inconspicuous nucleoli, and scant agranular cytoplasm

9
* Clinical features of CLL:
The disease occurs in older patients (> 50 years old). Generalized lymphadenopathy: enlargement of cervical, axillary or inguinal lymph nodes. Hepato-splenomegaly occurs in 50-60% of cases. Features of anemia …….. Spontaneous bruises, pupura, bleeding gums due to thrombocytopenia. Immunosuppression is a significant problem. - Bacterial infections followed by viral and fungal infections such as herpes zoster are also seen.
. Generalized lymphadenopathy: enlargement of cervical, axillary or inguinal lymph nodes. Hepato-splenomegaly occurs in 50-60% of cases. Features of anemia …….. Spontaneous bruises, pupura, bleeding gums due to thrombocytopenia. Immunosuppression is a significant problem. - Bacterial infections followed by viral and fungal infections such as herpes zoster are also seen.")
10
Cervical lymphadenopathy

11
* Laboratory investigations of CLL:
1. CBC: WBCs: high total leucocytic count (TLC) with absolute lymphocytosis . The lymphocytes appear small mature looking RBCs: ↓ (anaemia). Platelets: ↓ 2. Bone marrow: shows lymphocytic replacement of normal marrow elements.
 with absolute lymphocytosis . The lymphocytes appear small mature looking. RBCs: ↓ (anaemia). Platelets: ↓ 2. Bone marrow: shows lymphocytic replacement of normal marrow elements.")
12
METHODS OF LYMPH NODE EVALUATION

13
Physical examination. Imaging: Sampling Chest radiography
Ultrasonography Computed tomography (CT) Magnetic resonance imaging (MRI) Sampling Fine needle aspiration cytology (FNAC). Needle core biopsies. Excisional biopsy.
 Magnetic resonance imaging (MRI) Sampling. Fine needle aspiration cytology (FNAC). Needle core biopsies. Excisional biopsy.")
14
Physical examination Localized or generalized. Size of nodes.
Texture (consistency). Presence or absence of nodal tenderness. Signs of inflammation over the node. Skin lesions. Splenomegaly.
. Presence or absence of nodal tenderness. Signs of inflammation over the node. Skin lesions. Splenomegaly.")
15
Generalized lymphadenopathy has been defined as involvement of three or more noncontiguous lymph node areas.

16
Lymph nodes that are tender and soft are more likely to be due to an infectious process, whereas painless lymphadenopathy raises the concern of malignancy. Lymph nodes containing metastatic carcinoma are hard in consistency. Lymph nodes containing lymphoma are firm and rubbery. The larger the lymph node, the more likely a serious underlying cause exists, and lymph nodes greater than 3 to 4 cm in diameter in an adult are very significant.

17
Imaging Chest radiographs provide the most economical and easiest method to assess mediastinal and hilar lymphadenopathy but are not as accurate as CT of the chest. CT and ultrasound provide the most useful ways to assess abdominal and retroperitoneal lymphadenopathy. Ultrasound has the advantage of being less expensive and not requiring radiation exposure.

18
Sampling 1. Fine-needle aspiration cytology (FNAC):
Currently popular and is often an accurate way to diagnose infection or carcinoma It is inappropriate as an initial diagnostic maneuver for lymphoma. 2. Needle core biopsies: Will occasionally provide sufficient material for an unequivocal diagnosis of lymphoma.

19
3. Excisional biopsy: Which is most likely to provide the pathologist with adequate material to perform histologic, immunologic, and genetic studies, is the most appropriate approach.

21
1. Does the patient have a known illness e. g
1. Does the patient have a known illness e.g., infectious mononucleosis) that causes lymphadenopathy? Treat and monitor for resolution. 2. Are the nodes very large and/or very firm and thus suggestive of malignancy? Perform a biopsy. 3. Is the patient is very concerned about malignancy and unable to be reassured that malignancy is unlikely? Perform a biopsy.
 that causes lymphadenopathy Treat and monitor for resolution. 2. Are the nodes very large and/or very firm and thus suggestive of malignancy Perform a biopsy. 3. Is the patient is very concerned about malignancy and unable to be reassured that malignancy is unlikely Perform a biopsy.")
22
Cases

23
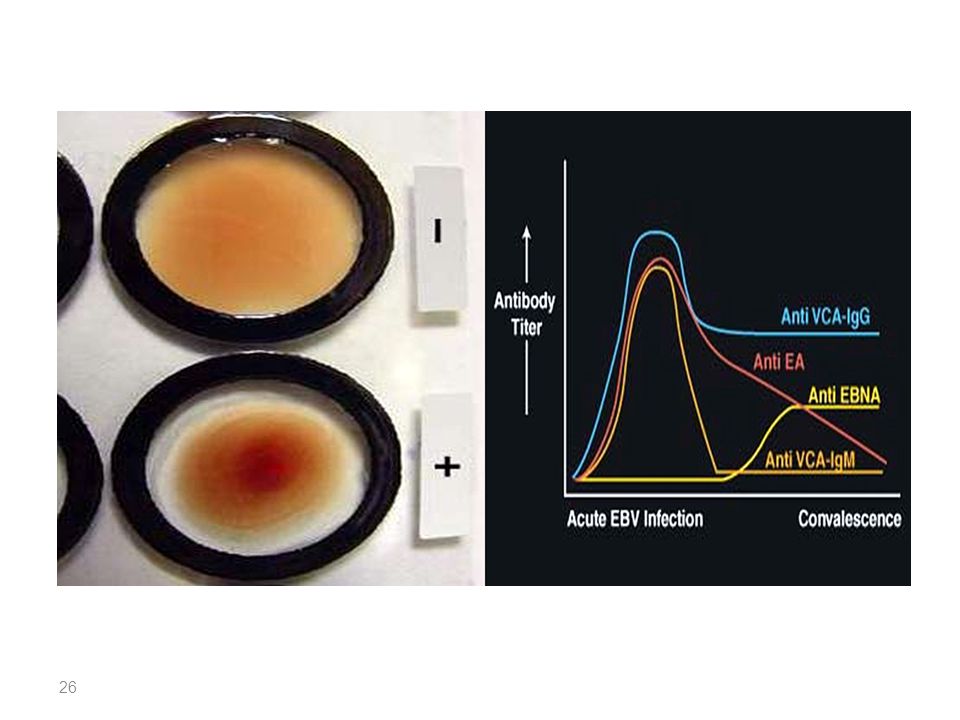
Case-1 A 19-year-old man had a severe sore throat and fever for the previous 3 days and was not getting better. On examination, his blood pressure, his pulse, and his respiratory rate were all normal. But his temperature was 39. His tonsils were markedly enlarged with overlying exudates. Tender lymph nodes were palpated in the cervical, axillary, and inguinal areas. Abdominal examination was significant for an enlarged liver and spleen.

24
A CBC showed an increased WBC count with many atypical lymphocytes
A CBC showed an increased WBC count with many atypical lymphocytes. A rapid heterophil antibody test was positive. He was given an analgesic/antipyretic and sent home to rest. Over the next 2 weeks, his sore throat, fever, and lymphadenopathy resolved.

27
What is your diagnosis?

28
Infectious mononucleosis

29
Case-2 A 3-year-old boy presents with epistaxis and fever. Multiple cutaneous petechae are evident, and there is generalized enlargement of lymph nodes, as well as palpable splenomegaly. The hemoglobin and platelet count is markedly decreased and WBC count elevated to 40,000 cells/μL, with a preponderance of lymphoblasts. What is your diagnosis ?

30
ALL (acute lymphoblastic leukaemia)
")
31
Case-3 A male child complaining of enlarged cervical lymph node. The lymph node was excised and examined by a pathologist who noticed the presence of extensive caseation necrosis, epithelioid granuloma consists of epithelioid cells, langhan’s giant cells and lymphocytes. The most probable diagnosis of this lymph node enlargement is………….

32
Tuberculous lymphadenitis

33
Good luck

Similar presentations






1 CHILDHOOD LEUKAEMIA. TA OGUNLESI (FWACP)2 LEUKAEMIA Heterogenous group of malignant disorders Characterised by uncontrolled clonal.>")













>")
i.>")