Download presentation
Presentation is loading. Please wait.

1
Annual Review of Nursing Services Staffing Plan Sample Outcome Metrics NH Nurse Staffing Toolkit 2010

2
Annual Review Core principles mandate at least a yearly review by the hospital-wide nursing staffing committee: A.Ensure the most current nursing services staffing plan does all of the following: 1)Improve inpatient care outcomes; 2)Positively affects clinical management; 3)Facilitates cost-effective quality nursing care 4)Remains consistent with acceptable and prevailing standards of safe nursing care and evidenced-based guidelines established by national nursing organizations. B.Make recommendations, based on the most recent review conducted, regarding how the most current nursing services staffing plan should be revised, if at all.

3
Don’t Reinvent the Wheel Use data you have that is consistent with what you require for credible metrics and adds value to the analysis Assess data that is currently collected for required reporting, voluntary reporting or internal quality (outcome and process) purposes
 purposes")
4
Inpatient Care Outcomes / Clinical Management / Cost Effective Care NDNQI metrics – Patient falls – Pressure ulcer prevalence – NHPPD – Nurse satisfaction Other metrics – Medication errors, adverse drug events and near misses – Care events – Patient satisfaction (HCHAPS nursing questions) – Patient complaints / grievances – Turnover rate – Vacancy rate – Overtime usage – Agency/traveler usage – ALOS – Costs/UOS – Costs/discharge – MD satisfaction – Staff satisfaction – TJC Core Measures
 – Patient complaints / grievances – Turnover rate – Vacancy rate – Overtime usage – Agency/traveler usage – ALOS – Costs/UOS – Costs/discharge – MD satisfaction – Staff satisfaction – TJC Core Measures")
5
Evidence Based Outcomes Needleman & Buerhaus et al. (2001) Strong consistent relationships between nurse staffing and –UTI, –pneumonia, –LOS, –UGI bleeds –shock. –In major surgical patients failure to rescue was also related to nurse staffing. Cho et al. (2003) An increase of 1 HPPD was associated with –8.9% decrease in odds of pneumonia, –10% increase in RN proportion was associated with 9.5% decrease in odds of pneumonia, –increased nursing HPPD > higher probability of pressure ulcers
 Strong consistent relationships between nurse staffing and –UTI, –pneumonia, –LOS, –UGI bleeds –shock. –In major surgical patients failure to rescue was also related to nurse staffing. Cho et al. (2003) An increase of 1 HPPD was associated with –8.9% decrease in odds of pneumonia, –10% increase in RN proportion was associated with 9.5% decrease in odds of pneumonia, –increased nursing HPPD > higher probability of pressure ulcers.")
6
Evidence Based Outcomes Aiken et al. (2002) Each additional patient cared for by a nurse was associated with –a 7% increase likelihood of dying within 30 days of admission, and –a 7% increase in failure to rescue rates, –a 23% increase in nurse burnout –a 15% increase in job dissatisfaction. Rogers et al. (2004) Errors and near errors more likely to occur when nurses work >12 hours.
 Each additional patient cared for by a nurse was associated with –a 7% increase likelihood of dying within 30 days of admission, and –a 7% increase in failure to rescue rates, –a 23% increase in nurse burnout –a 15% increase in job dissatisfaction. Rogers et al. (2004) Errors and near errors more likely to occur when nurses work >12 hours..")
7
Evidence Based Outcomes 2007 AHRQ Report Increased RN to Patient Ratios was associated with decreased hospital mortality, LOS, failure to rescue (but not necessarily causal) For every increase 1 RN FTE per patient day, decrease in mortality in ICU by 9% and in surgical patients by 16%. For Every additional patient per RN per shift— –7% increase risk of hospital acquired pneumonia –45% increased risk of unplanned extubation –17% increased risk of medical complications

8
Evidence Based Outcomes 2007 AHRQ Report An increase of 1 RN FTE per day in ICU –28% decrease in risk of CPR, –51% decrease in risk of unplanned extubation, –60% decrease risk of pulmonary failure –30% decreased risk of hospital acquired pneumonia An increase of 1 RN FTE per day in Surgery patients –16% decreased risk of failure to rescue, –30% decreased risk of nosocomial blood stream infections

9
Evidence Based Outcomes 2007 AHRQ Report Death rate decreased by 1.98% for every additional total nurse hour per day. Nurse satisfaction and autonomy was associated with reduction of risk of death. Increased nurse turnover was associated with a 0.2% increase in falls. No research on the effect of agency or temporary staff or international nurses in staffing.

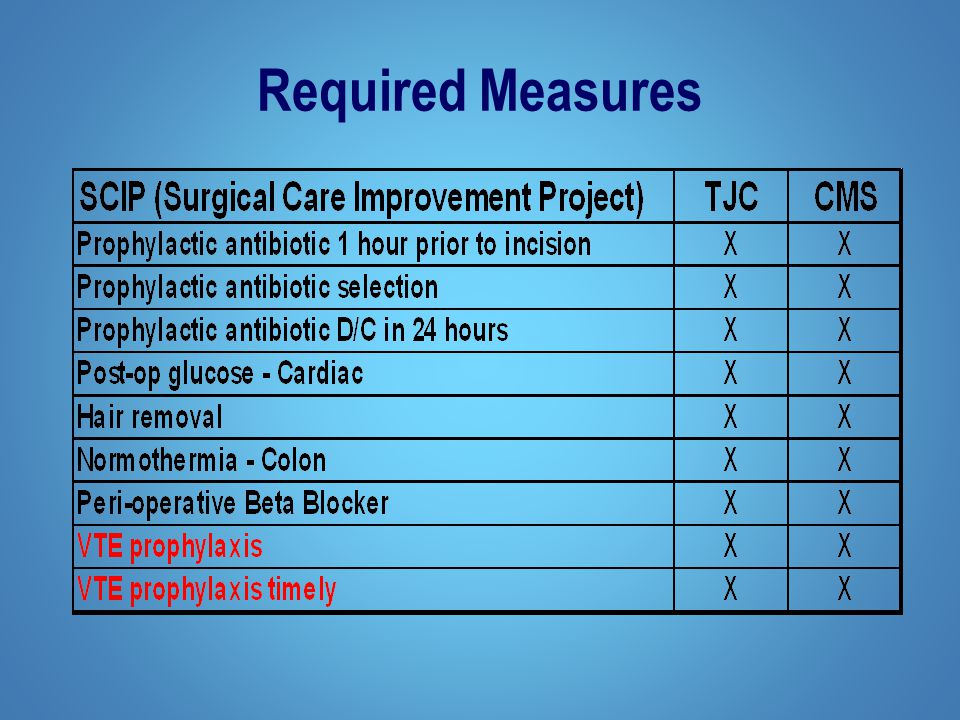
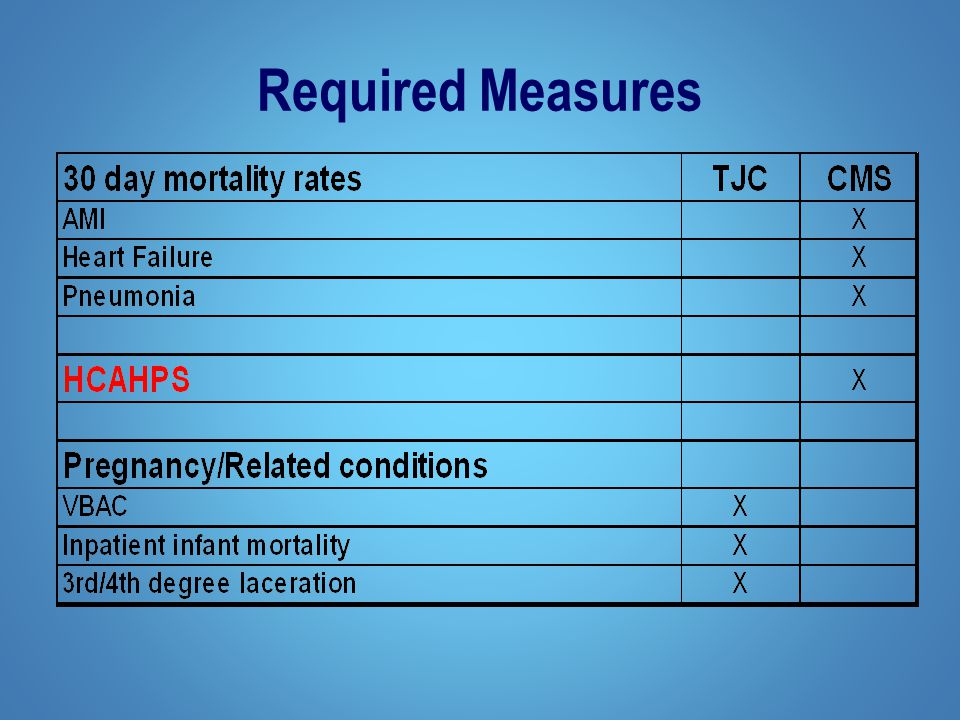
10
Required Measures

16
Measures on the Horizon

17
Required Measures – HCAHPS Hospital Consumer Assessment of Healthcare Providers and Systems Communication with nurses Communication with doctors Responsiveness of staff Pain management Communication about medication Cleanliness of hospital Discharge information Overall rating Willingness to recommend

18
CMS Hospital Acquired Conditions (never events) CABG Mediastinitis Catheter Associated Urinary Tract Infection Pressure Ulcers Vascular Catheter- Association Infection Object Left in Surgery Hospital Acquired Injuries (i.e. falls/burns/fractures, etc) Air Embolism Blood Transfusion Incompatibility
 Air Embolism Blood Transfusion Incompatibility.")
19
TJC Proposed Nurse Sensitive Measures Patient-centered Outcome Measures: 1.Death among surgical inpatients with treatable serious complications (failure to rescue): The percentage of major surgical inpatients who experience a hospital- acquired complication and die. 2.Pressure ulcer prevalence: Percentage of inpatients who have a hospital acquired pressure ulcer. 3.Falls prevalence: Number of inpatient falls per inpatient days. 4.Falls with injury: Number of inpatient falls with injuries per inpatient days. 5.Restraint prevalence: Percentage of inpatients who have a vest or limb restraint.

20
TJC Proposed Nurse Sensitive Measures Patient-centered Outcome Measures: 6.Urinary catheter-associated urinary tract infection for intensive care unit (ICU) patients: Rate of urinary track infections associated with use of urinary catheters for ICU patients. 7.Central line catheter-associated blood stream infection rate for ICU and high-risk nursery patients: Rate of blood stream infections associated with use of central line catheters for ICU and high-risk nursery patients. 8.Ventilator-associated pneumonia for ICU and high-risk nursery patients: Rate of pneumonia associated with use of ventilators for ICU and high-risk nursery patients.

21
TJC Proposed Nurse Sensitive Measures Nursing-centered Intervention Measures: 9.Smoking cessation counseling for acute myocardial infarction. 10.Smoking cessation counseling for heart failure. 11.Smoking cessation counseling for pneumonia. Each measures the percentage of patients with a history of smoking within the past year who received smoking cessation advice or counseling during hospitalization.

22
TJC Proposed Nurse Sensitive Measures System-centered Measures: 12.Skill mix: Percentage of registered nurse, licensed vocational/practical nurse, unlicensed assistive personnel, and contracted nurse care hours to total nursing care hours. 13.Nursing care hours per patient day: Number of registered nurses per patient day and number of nursing staff hours (registered nurse, licensed vocational/practical nurse, and unlicensed assistive personnel) per patient day.
 per patient day..")
23
TJC Proposed Nurse Sensitive Measures System-centered Measures: 14.Practice Environment Scale ― Nursing Work Index: Composite score and scores for five subscales: a.nurse participation in hospital affairs; b.nursing foundations for quality of care; c.nurse manager ability, leadership and support of nurses; d.staffing and resource adequacy; and e.collegiality of nurse-physician relations. 15.Voluntary turnover: Number of voluntary uncontrolled separations during the month by category (RNs, APNs, LVN/LPNs, NAs).
..")
24
Don’t Reinvent the Wheel Use data you have that is consistent with what the statute requires and adds value to the analysis Assess data that is currently collected for required reporting, voluntary reporting or internal quality (outcome and process) purposes As new measures of performance are added/required consider incorporating them into the annual review process
 purposes As new measures of performance are added/required consider incorporating them into the annual review process")
25
Questions?

Similar presentations










 Richard M Jones, Specialist Nurse.>")





 Key Facts Three year demo (2003-2006); extended for three additional years through Oct. 2009 225 hospitals.>")





