Download presentation
Presentation is loading. Please wait.

1
Spinal cord protection in surgery of descending thoracic aorta Present by R1 康庭瑞

2
Case 55 y/o male, HTN for 20+ years with regular medical control for 5 years Chronic dissecting aortic aneurysm type III noted for 5 years Left chest pain for 1 week Denied other systemic diseases Laboratory data: within normal range

7
Case Normal screening spirometry 2-D echocardiography: dilated aortic root(diameter 63mm) & LA, mild MR, good LV contractility Planning: 1.Left post-lat thoracotomy 2. Femoral- femoral CPB 3. Hypothermia with circulation arrest and retrograde cerebral perfusion via high CVP 18~20mmHg by femoral artery perfusion and partial clamp of venous drain tube 4. Restore proximal aorta perfusion after proximal anastomosis through graft cannulation 5. Open distal anastomosis

11
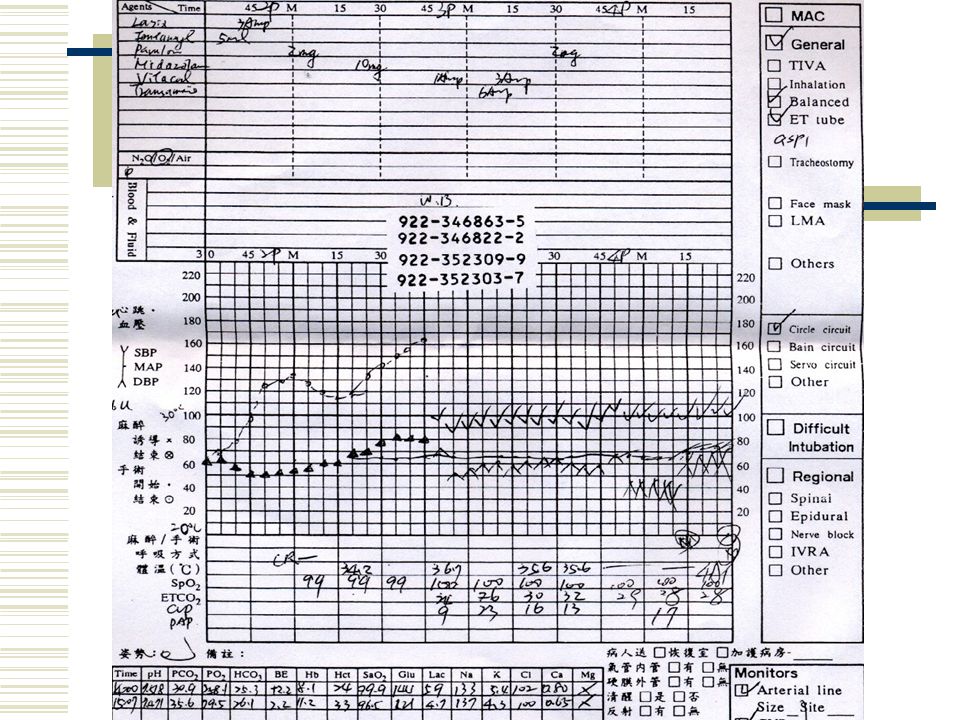
Case Cooling to 16 ℃ Partial bypass: 3hr25min Total bypass: 2hr30min Aortic cross clamp: ?min Circulatory arrest: 20min Double lumen single-lumen ET tube ICU weaning and extubation on post-op day 3 without major complications

12
Consequences of aortic cross- clamping Spinal cord ischemia Vascular anatomy: single ant. spinal a. from vertebral a. supply ant. 2/3 of spinal cord; pair of post. spinal a. from post. cerebellar a. supply remainder of spinal cord Spinal cord perfusion from: vertebral, deep cervical, intercostal, and lumbar a. radicular a. The largest radicular a. (artery of Adamkiewicz): origin from T9~12 intercostal a. supply the majority of blood to the lower 2/3 of the spinal cord
: origin from T9~12 intercostal a. supply the majority of blood to the lower 2/3 of the spinal cord.")
13
Spinal cord ischemia Paraplegia and paraparesis: major cause of morbidity and mortality after extensive TAAA repair Incidence: 2~40%, depending on the site and the degree of aortic lesion, with/without dissection (2- fold), cross-clamp duration (less than 30min), ligation of the artery of Adamkiewicz, elevation in CSF pressure, reperfusion injury, perioperative hyperglycemia
, cross-clamp duration (less than 30min), ligation of the artery of Adamkiewicz, elevation in CSF pressure, reperfusion injury, perioperative hyperglycemia")
14
Spinal cord perfusion pressure CSF pressure increases during aortic clamping “spinal cord compartment syndrome” Reduction of CSF pressure improves SCPP Lumbar drains Combined with distal aortic perfusion

15
Result CSF pressure was maintained at 10mmHg or less 148 nonemergent patients who received simple cross- clamping 105 with combined adjuncts, 43 with or without the addition of a single adjunct 0.9% vs 7% (p<0.04)
")
16
Result 2.6% vs 13.0% Reduced immediate deficits, particularly paraplegia Infrequent delayed neurologic deficits in both groups The longer the ischemic time were, the greater the benefit afforded with CSFD

17
Conclusions Significantly reduced the rate of neurologic deficit during nonemergent repair of descending thoracic aortic aneurysms The recently reports had convinced most surgeons of the benefit of CSF drainage in descending thoracic aortic aneurysm

18
Other adjuncts Selective cooling spinal cord via lavage of the epidural space: regional hypothemic (26 ℃ ) protection of at-risk thoracolumbar cord Corticosteroid, thiopental, NMDA antagonist, papaverine
 protection of at-risk thoracolumbar cord Corticosteroid, thiopental, NMDA antagonist, papaverine")
19
Complications of lumbar drainage after TAAA repair Postoperative lower extremity neurologic deficit: result of thromboembolic or delayed ischemic complication or resulting from lumbar drainage Intradural hematoma: 3.2% in this study CT, MRI

20
Hypothermic cardiopulmonary bypass and circulatory arrest Methylprednisone and thiopental are given during the period of cooling to 15 ℃ Circulatory arrest intervals: mean, 38min Postoperative neurologic injury: 2.7% Conclusion: hypothermic circulatory arrest offers certain advantages over other techniques and using of other adjunctive measures is not necessary

21
References Hypothermic cardiopulmonary bypass and circulatory arrest for operations on the descending thoracic and thoraco- abdominal aorta. Annals of thoracic surgery.74(5):S1885- 7,2002 Nov. Cerebrospinal fluid drainage reduces paraplegia after thoracoabdominal aortic aneurysm repair: results of a randomized clinical trial. Journal of vascular surgery.35(4):631-9,2002 Apr. Thoracoabdominal aneurysm repair: results with 337 operations performed over a 15-year interval. Annals of surgery.236(4):471-9,2002 Oct. Complications of lumbar drainage after thoracoabdominal aortic aneurysm repair. Journal of vascular surgery.34(4):623-7,2001 Oct.
:S ,2002 Nov. Cerebrospinal fluid drainage reduces paraplegia after thoracoabdominal aortic aneurysm repair: results of a randomized clinical trial. Journal of vascular surgery.35(4):631-9,2002 Apr. Thoracoabdominal aneurysm repair: results with 337 operations performed over a 15-year interval. Annals of surgery.236(4):471-9,2002 Oct. Complications of lumbar drainage after thoracoabdominal aortic aneurysm repair. Journal of vascular surgery.34(4):623-7,2001 Oct..")
22
Thanks for your attention !

Similar presentations








 ・ In 1998, we developed a modified elephant trunk (ET) technique using a single four-branched arch graft with a sewing “collar” and “long.>")






>")









