Download presentation
Presentation is loading. Please wait.

1
Aortic Intervention & Spinal Cord Ischemia Alexander J Gregory MD, FRCPC Department of Anesthesia, University of Calgary Calgary, Alberta, Canada May 30, 2014 Thoracic Aortic Rounds aorta.ca

2
OBJECTIVES

4
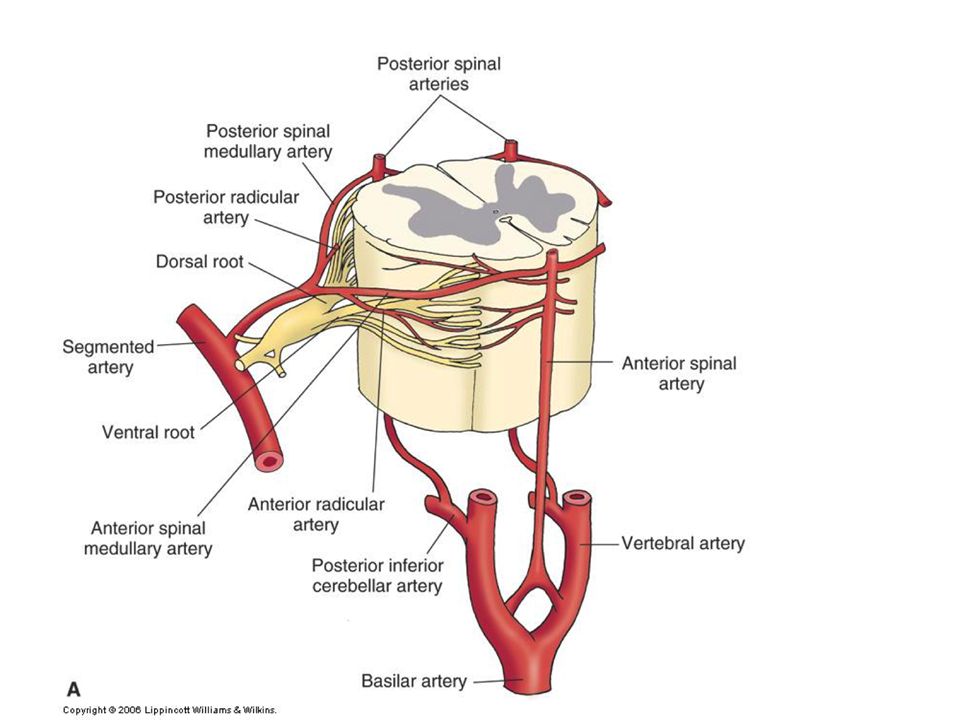
Cervical Plexus (Vertebrals) Hypogastric Plexus (Iliacs) Lumbar Segmentals Intercostal Segmentals
 Hypogastric Plexus (Iliacs) Lumbar Segmentals Intercostal Segmentals")
6
Risk

7
SCI incidence TAAA= 8-28% TAA= 2-3% TEVAR = 2-3% HAR = 0-4%

8
Risk Factors > 1 territory of blood supply lost Peri-operative hypotension Chronic renal failure Stent coverage Artery of Adamkiewicz sacrifice Atherosclerotic aorta Smoking Complicated Type-B, HAR & aortic transection Age

9
Risk Factors > 1 territory of blood supply lost Peri-operative hypotension Chronic renal failure ? Stent coverage ? Artery of Adamkiewicz sacrifice ?? Atherosclerotic aorta ?? Smoking ?? Complicated Type-B, HAR & aortic transection ?? Age

11
LSCA Bypass

12
Semin Thorac Cardiovasc Surg 2009; 21:347-354 Ishimaru Classification

13
Arm Ischemia

14
Vertebrobasilar Ischemia

15
SCI

16
Recommendation 1: In patients who need elective TEVAR where achievement of a proximal seal necessitates coverage of the left subclavian artery, we suggest routine preoperative revascularization, despite the very low-quality evidence (GRADE 2, level C). J Vasc Surg 2009;50:1155-8

17
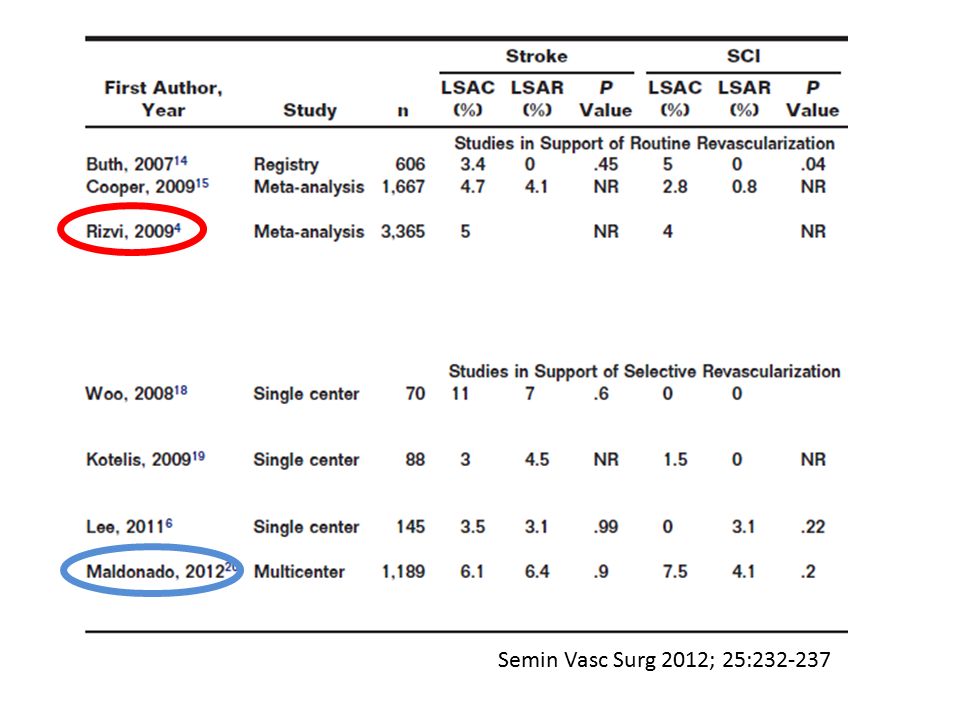
Semin Vasc Surg 2012; 25:232-237

19
Routine revascularization is unnecessary in the majority of patients requiring zone II coverage during thoracic endovascular aortic repair: A longitudinal outcomes study using United States Medicare population data. Wilson JE, Galiñanes EL, Hu P, Dombrovskiy Vym and Vogel TR. Vascular. 2013 Sep 3. [Epub ahead of print] Medicare & Medicaid Services- Inpatient claims 2006-07 n= 2676 TEVAR, 869 LSCA covered, 49 LSCA bypassed TEVAR + LSCA w/out bypass = 1.9% bypassed in 1 st year TEVAR + LSCA + bypass = 12.8% vs 3.8% stroke & higher mortality

20
LSCA bypass Prophylactic LSCA bypass: LIMA AV fistula L hand dominance Supra-aortic or COW abnormalities LSCA bypass for clinically relevant malperfusion SCI does not appear to be substantially increased in most patients

22
Collateral Network

25
J Thorac Cardiovasc Surg 2011;141:1020-8 = ASA = DP T L

26
J Thorac Cardiovasc Surg 2011;141:1020-8

28
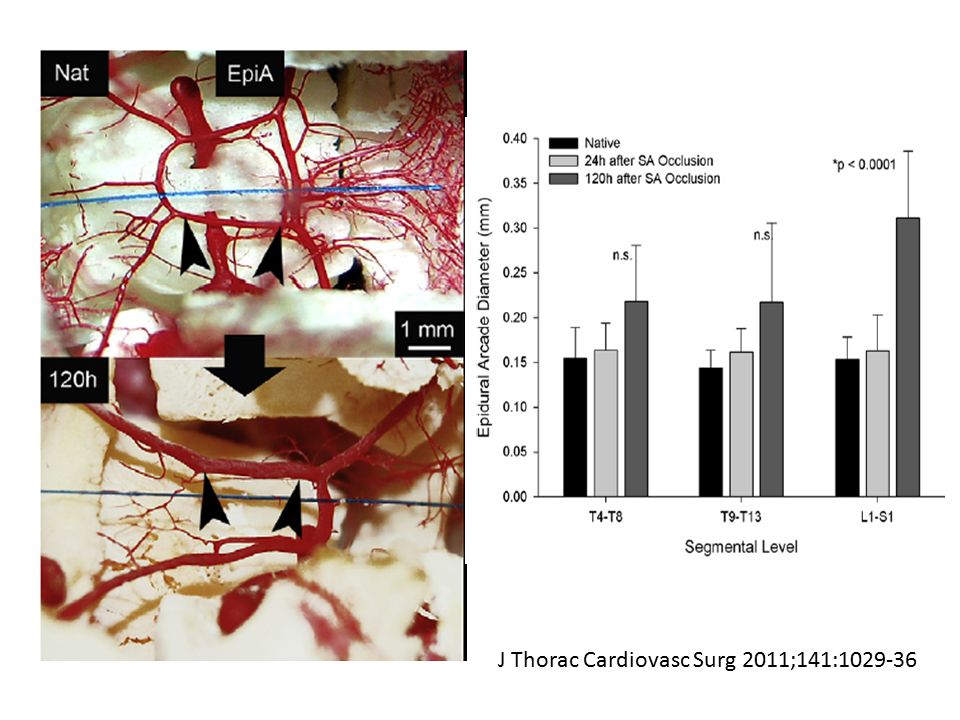
J Thorac Cardiovasc Surg 2011;141:1029-36

31
Nat 24h 120h

32
J Thorac Cardiovasc Surg 2011;141:1029-36

33
J Thorac Cardiovasc Surg 2010;140:S125-30

34
T & L SA sacrifice

35
J Thorac Cardiovasc Surg 2010;140:S125-30 T & L SA sacrifice L only SA sacrifice

36
J Thorac Cardiovasc Surg 2010;140:S125-30 T & L SA sacrifice L only SA sacrifice T SA sacrifice 7d later

38
CSF Drains

40
Hanna et al 2013 2002-2012, TEVAR, n=381 Prev aortic surgery + >75% + below T6 or Hybrid repair Crawford I-III Pre-op CSFd= 21% (81/381) Post-op CSFd for SCI= 1% (3/300) Group SCI= 6.6% (25/381), 1.8% (7/381) permanent Pre-op CSFd SCI= 14.8% (12/81), 7.4% (6/81) permanent No CSFd SCI= 4.3% (13/300), 0.3% (1/300) permanent CSFd complications= 11.1% (9/81), HA 5, leak 2, minor SDH 2 No CSF drained 32% (26/81) Keith et al 2012 2000-2010, TEVAR, n=266 Pre-op CSFd excluded, post-op SCI protocol SCI= 6% (16/266), 3.4% (9/266) permanent CSFd req’d= 3.8% (10/266) CSFd reversed SCI= 30% (3/10) CSFd complications= 10% (1/10), SDH 1 Time of SCI onset to CSFd= 8.2 +/- 10.5 hrs
 Post-op CSFd for SCI= 1% (3/300) Group SCI= 6.6% (25/381), 1.8% (7/381) permanent Pre-op CSFd SCI= 14.8% (12/81), 7.4% (6/81) permanent No CSFd SCI= 4.3% (13/300), 0.3% (1/300) permanent CSFd complications= 11.1% (9/81), HA 5, leak 2, minor SDH 2 No CSF drained 32% (26/81) Keith et al , TEVAR, n=266 Pre-op CSFd excluded, post-op SCI protocol SCI= 6% (16/266), 3.4% (9/266) permanent CSFd req’d= 3.8% (10/266) CSFd reversed SCI= 30% (3/10) CSFd complications= 10% (1/10), SDH 1 Time of SCI onset to CSFd= 8.2 +/ hrs")
41
Hanna et al 2013 2002-2012, TEVAR, n=381 Prev aortic surgery + >75% + below T6 or Hybrid repair Crawford I-III Pre-op CSFd= 21% (81/381) Post-op CSFd for SCI= 1% (3/300) Group SCI= 6.6% (25/381), 1.8% (7/381) permanent Pre-op CSFd SCI= 14.8% (12/81), 7.4% (6/81) permanent No CSFd SCI= 4.3% (13/300), 0.3% (1/300) permanent CSFd complications= 11.1% (9/81), HA 5, leak 2, minor SDH 2 No CSF drained 32% (26/81) Keith et al 2012 2000-2010, TEVAR, n=266 Pre-op CSFd excluded, post-op SCI protocol SCI= 6% (16/266), 3.4% (9/266) permanent CSFd req’d= 3.8% (10/266) CSFd reversed SCI= 30% (3/10) CSFd complications= 10% (1/10), SDH 1 Time of SCI onset to CSFd= 8.2 +/- 10.5 hrs
 Post-op CSFd for SCI= 1% (3/300) Group SCI= 6.6% (25/381), 1.8% (7/381) permanent Pre-op CSFd SCI= 14.8% (12/81), 7.4% (6/81) permanent No CSFd SCI= 4.3% (13/300), 0.3% (1/300) permanent CSFd complications= 11.1% (9/81), HA 5, leak 2, minor SDH 2 No CSF drained 32% (26/81) Keith et al , TEVAR, n=266 Pre-op CSFd excluded, post-op SCI protocol SCI= 6% (16/266), 3.4% (9/266) permanent CSFd req’d= 3.8% (10/266) CSFd reversed SCI= 30% (3/10) CSFd complications= 10% (1/10), SDH 1 Time of SCI onset to CSFd= 8.2 +/ hrs")
42
Hanna et al 2013 2002-2012, TEVAR, n=381 Prev aortic surgery + >75% + below T6 or Hybrid repair Crawford I-III Pre-op CSFd= 21% (81/381) Post-op CSFd for SCI= 1% (3/300) Group SCI= 6.6% (25/381), 1.8% (7/381) permanent Pre-op CSFd SCI= 14.8% (12/81), 7.4% (6/81) permanent No CSFd SCI= 4.3% (13/300), 0.3% (1/300) permanent CSFd complications= 11.1% (9/81), HA 5, leak 2, minor SDH 2 No CSF drained 32% (26/81) Keith et al 2012 2000-2010, TEVAR, n=266 Pre-op CSFd excluded, post-op SCI protocol SCI= 6% (16/266), 3.4% (9/266) permanent CSFd req’d= 3.8% (10/266) CSFd reversed SCI= 30% (3/10) CSFd complications= 10% (1/10), SDH 1 Time of SCI onset to CSFd= 8.2 +/- 10.5 hrs
 Post-op CSFd for SCI= 1% (3/300) Group SCI= 6.6% (25/381), 1.8% (7/381) permanent Pre-op CSFd SCI= 14.8% (12/81), 7.4% (6/81) permanent No CSFd SCI= 4.3% (13/300), 0.3% (1/300) permanent CSFd complications= 11.1% (9/81), HA 5, leak 2, minor SDH 2 No CSF drained 32% (26/81) Keith et al , TEVAR, n=266 Pre-op CSFd excluded, post-op SCI protocol SCI= 6% (16/266), 3.4% (9/266) permanent CSFd req’d= 3.8% (10/266) CSFd reversed SCI= 30% (3/10) CSFd complications= 10% (1/10), SDH 1 Time of SCI onset to CSFd= 8.2 +/ hrs")
43
Hanna et al 2013 2002-2012, TEVAR, n=381 Prev aortic surgery + >75% + below T6 or Hybrid repair Crawford I-III Pre-op CSFd= 21% (81/381) Post-op CSFd for SCI= 1% (3/300) Group SCI= 6.6% (25/381), 1.8% (7/381) permanent Pre-op CSFd SCI= 14.8% (12/81), 7.4% (6/81) permanent No CSFd SCI= 4.3% (13/300), 0.3% (1/300) permanent CSFd complications= 11.1% (9/81), HA 5, leak 2, minor SDH 2 No CSF drained 32% (26/81) Keith et al 2012 2000-2010, TEVAR, n=266 Pre-op CSFd excluded, post-op SCI protocol SCI= 6% (16/266), 3.4% (9/266) permanent CSFd req’d= 3.8% (10/266) CSFd reversed SCI= 30% (3/10) CSFd complications= 10% (1/10), SDH 1 Time of SCI onset to CSFd= 8.2 +/- 10.5 hrs
 Post-op CSFd for SCI= 1% (3/300) Group SCI= 6.6% (25/381), 1.8% (7/381) permanent Pre-op CSFd SCI= 14.8% (12/81), 7.4% (6/81) permanent No CSFd SCI= 4.3% (13/300), 0.3% (1/300) permanent CSFd complications= 11.1% (9/81), HA 5, leak 2, minor SDH 2 No CSF drained 32% (26/81) Keith et al , TEVAR, n=266 Pre-op CSFd excluded, post-op SCI protocol SCI= 6% (16/266), 3.4% (9/266) permanent CSFd req’d= 3.8% (10/266) CSFd reversed SCI= 30% (3/10) CSFd complications= 10% (1/10), SDH 1 Time of SCI onset to CSFd= 8.2 +/ hrs")
44
Hanna et al 2013 2002-2012, TEVAR, n=381 Prev aortic surgery + >75% + below T6 or Hybrid repair Crawford I-III Pre-op CSFd= 21% (81/381) Post-op CSFd for SCI= 1% (3/300) Group SCI= 6.6% (25/381), 1.8% (7/381) permanent Pre-op CSFd SCI= 14.8% (12/81), 7.4% (6/81) permanent No CSFd SCI= 4.3% (13/300), 0.3% (1/300) permanent CSFd complications= 11.1% (9/81), HA 5, leak 2, minor SDH 2 No CSF drained 32% (26/81) Keith et al 2012 2000-2010, TEVAR, n=266 Pre-op CSFd excluded, post-op SCI protocol SCI= 6% (16/266), 3.4% (9/266) permanent CSFd req’d= 3.8% (10/266) CSFd reversed SCI= 30% (3/10) CSFd complications= 10% (1/10), SDH 1 Time of SCI onset to CSFd= 8.2 +/- 10.5 hrs
 Post-op CSFd for SCI= 1% (3/300) Group SCI= 6.6% (25/381), 1.8% (7/381) permanent Pre-op CSFd SCI= 14.8% (12/81), 7.4% (6/81) permanent No CSFd SCI= 4.3% (13/300), 0.3% (1/300) permanent CSFd complications= 11.1% (9/81), HA 5, leak 2, minor SDH 2 No CSF drained 32% (26/81) Keith et al , TEVAR, n=266 Pre-op CSFd excluded, post-op SCI protocol SCI= 6% (16/266), 3.4% (9/266) permanent CSFd req’d= 3.8% (10/266) CSFd reversed SCI= 30% (3/10) CSFd complications= 10% (1/10), SDH 1 Time of SCI onset to CSFd= 8.2 +/ hrs")
45
Hanna et al 2013 2002-2012, TEVAR, n=381 Prev aortic surgery + >75% + below T6 or Hybrid repair Crawford I-III Pre-op CSFd= 21% (81/381) Post-op CSFd for SCI= 1% (3/300) Group SCI= 6.6% (25/381), 1.8% (7/381) permanent Pre-op CSFd SCI= 14.8% (12/81), 7.4% (6/81) permanent No CSFd SCI= 4.3% (13/300), 0.3% (1/300) permanent CSFd complications= 11.1% (9/81), HA 5, leak 2, minor SDH 2 No CSF drained 32% (26/81) Keith et al 2012 2000-2010, TEVAR, n=266 Pre-op CSFd excluded, post-op SCI protocol SCI= 6% (16/266), 3.4% (9/266) permanent CSFd req’d= 3.8% (10/266) CSFd reversed SCI= 30% (3/10) CSFd complications= 10% (1/10), SDH 1 Time of SCI onset to CSFd= 8.2 +/- 10.5 hrs
 Post-op CSFd for SCI= 1% (3/300) Group SCI= 6.6% (25/381), 1.8% (7/381) permanent Pre-op CSFd SCI= 14.8% (12/81), 7.4% (6/81) permanent No CSFd SCI= 4.3% (13/300), 0.3% (1/300) permanent CSFd complications= 11.1% (9/81), HA 5, leak 2, minor SDH 2 No CSF drained 32% (26/81) Keith et al , TEVAR, n=266 Pre-op CSFd excluded, post-op SCI protocol SCI= 6% (16/266), 3.4% (9/266) permanent CSFd req’d= 3.8% (10/266) CSFd reversed SCI= 30% (3/10) CSFd complications= 10% (1/10), SDH 1 Time of SCI onset to CSFd= 8.2 +/ hrs")
46
CSFd Current FMC Strategy Selective use Intra-op CSF pressure 70 mmHg CSF drainage < 10 mL/hr SSEP Fast-track general anesthesia Post-op q1h neuro vitals Neuro normal= CSF pressure 65 mmHg SCI protocol

Similar presentations









 Arch Debranching vs. Elephant Trunk for Hybrid Repair of the Proximal Thoracic Aorta Arch Debranching versus Elephant Trunk Procedures for Hybrid Repair.>")











>")






